
Abstract
A 17-year-old female with migraine with aura complained of fatigue and was diagnosed with anemia. Three years later, changes in her headache pattern prompted hospital referral. Brain MRI showed a bi-lobed extra-axial intracerebral tumor encroaching both parieto-occipital regions. The resection specimen yielded a rare diagnosis of primary intracranial angiomatoid fibrous histiocytoma (AFH). Tumor removal resulted in cessation of her migraine and anemia. AFH may cause systemic symptoms – in this case fatigue and anemia – long before focal neurological symptoms are present. This is the first report of an intracranial AFH presenting as migraine with visual aura and anemia.
Angiomatoid fibrous histiocytoma (AFH) is a very rare, low-grade malignant soft tissue tumour originally described as angiomatoid ‘malignant’ fibrous histiocytoma (1). To date, just two cases of primary intracranial AHF have been published (2,3). This is a report of an unusual case of a primary intracranial AFH.
A 17-year-old female was diagnosed with anaemia and also started experiencing migraine headaches with typical visual aura. Three years later, the headache changed and was now constant, described as pressing with a more diffuse distribution, often felt as if originating in the neck. The headache was intense (VRS 8-10). Treatment with benzodiazepine, over the counter analgesics and triptans had only temporary relieving effect. In the emergency room, a physical examination revealed blurry vision in the lower field of vision bilaterally, without scotomas and a discrete hyper-reflexia in the left arm. Brain magnetic resonance imaging (MRI) showed a well-delineated bi-lobed extra-axial intracerebral tumour encroaching both parieto-occipital regions (Figure 1). Radical tumour resection was accomplished in two operations. The tumour was difficult to classify. Based on histology and immunohistochemistry (Figure 2), the principal differential diagnosis was a rhabdoid meningioma (WHO grade III), but lack of SSTR2A expression would be unusual for a meningioma and a rhabdoid meningioma would typically show higher proliferative indices and often other features of malignancy. In addition, the ultrastructural features were not typical for a meningioma. After external consultation, our conclusion was that of a low-grade mesenchymal neoplasm, most compatible with AFH.
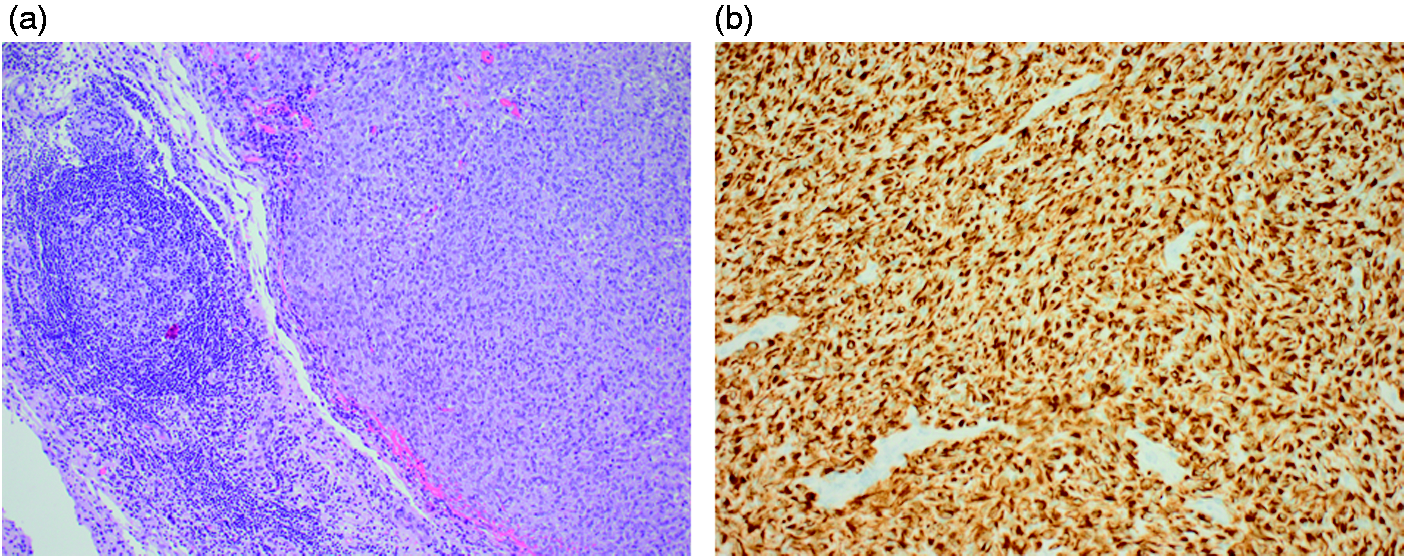
Preoperative imaging. (a) T2-weighted MR image showing the bi-lobed occipital tumour surrounded by a rim of hypo intensity likely delineating the tumour capsule. There is extensive perifocal oedema especially at the left side. (b) Contrast enhanced T1-weighted MR image of the brain showing the tumor as a heterogeneously enhancing parieto-occipital lesion. Whole-body 18-fludeoxyglucose (FDG) Positron emission tomography/computed tomography (PET/CT) showed no other tumour foci. Histo-pathology of AFH. Histological sections demonstrated a well-demarcated tumour composed of epithelioid cells with round to oval nuclei. The nuclei were uniform with finely dispersed chromatin and prominent nucleoli. Electron microscopic examination showed that the cytoplasm of tumour cells contained numerous mitochondria, as well as thin filaments. The diagnosis of AFH is based on histopathology and immunohistochemistry. AFH is often associated with three characteristic translocations: EWSR1-CREB1; FUS-ATF1; EWSR1-ATF1, leading to the formation of chimeric fusion genes. Fluorescence in situ hybridisation (FISH) probes to EWSR1 and FUS, in theory, should detect all three translocations/gene fusions. FISH analyses for EWS- and FUS-rearrangements were negative. RT-PCR-analysis did not reveal EWS/ATF-1 translocation. Although the characteristic translocations involving the EWS- or FUS-genes were not detected in this case, previous reports suggest that around one in four cases may be translocation-negative (4). Alternatively, apparent translocation-negative patients may in fact harbour new undefined translocation/gene fusions outside EWSR1 or FUS. In our case the morphologic and immunohistochemical features are highly suggestive of AFH. (a) Tumour morphology shows a well-demarcated tumour surrounded by a fibrous capsule with prominent chronic inflammation, sometimes with germinal centre formation. Haematoxylin and eosin (× 100). The tumour was surrounded by a dense fibrous capsule with prominent chronic inflammation, sometimes with germinal centre formation. There were a few small foci of necrosis. There were relatively few mitoses, but focally a maximum of four mitoses in 10 high power fields were counted and whorls or psammoma bodies were not observed. (b) Immunohistochemistry demonstrated widespread staining for desmin (X 200) and therefore a rhabdomyosarcoma or a leiomyomatous tumour was initially considered, but negative stains for all other myogenic markers excluded this possibility. The histological picture and lack of nuclear STAT6 expression ruled out haemangiopericytoma or solitary fibrous tumour of the meninges. Negative stains for all glial end neuronal markers excluded the possibility of a glioma. The cells were also positive for epithelial membrane antigen and there was patchy positivity for CD99. The Ki67 index was approximately 3%. INI1 staining was retained in tumour nuclei. The following stains were negative: somatostatin receptor 2A (SSRT2A), MYF4, myoglobin, smooth muscle actin, muscle specific actin, caldesmon, ALK1, CK, TTF1, AFP, PLAP, CD117, HCG, CD34, STAT6, CD56, GFAP, synaptophysin, chromogranin, NF, S-100, IDH1, OLIG2, SOX2, ER, PGR, CD68, CD1A, melan A, HMB45 and Fli-1.
Removal of the tumour resulted in complete cessation of her migraine when assessed 1 and 4 months after the second operation. Her haemoglobin levels were normal and, clinically, she appeared less anaemic. Three months after the second surgery MRI showed no signs of residual or recurrent tumour. Perimetry-exam ad modum Donders found no scotoma and slightly blurry vision inferiorly bilaterally. Post-OP visual acuity was 1.0.
Given the intermediate malignant potential of the tumour, the patient will require continued clinical and radiographic surveillance.
This is the first report of an intracranial AFH presenting as migraine-like headache with visual aura and anaemia. AFH may cause systemic symptoms – in this case fatigue and anaemia – long before focal neurological symptoms are present.
Conclusion
We report a case of a young woman with migraine with aura and anaemia who noted a change in her headache presentation leading to a MRI showing bi-occipital tumour masses. Based on clinical, radiographic and histopathologic features, the diagnosis was a rare incidence of intracranial AFH. Radical tumour resection was accomplished in two operations, resulting in complete cessation of migraine and anaemia. The patient will require follow-ups for possible recurrence. This case underscores that change in prior headache pattern should always prompt the search for secondary headache causes even in a young patient.
Informed consent
The patient gave informed consent to the publication of this case report.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.