
Abstract
Background
Migraine is associated with sleep disturbances in men and non-pregnant women. However, relatively little is known about sleep disturbances among pregnant migraineurs. We investigated sleep disturbances among pregnant women with and without history of migraine.
Methods
This cross-sectional study was conducted among 1324 women who were recruited during early pregnancy. Migraine diagnoses were based on the International Classification of Headache Disorders-II criteria. The Pittsburgh Sleep Quality Index (PSQI) questionnaire was used to evaluate sleep-related characteristics including sleep duration, sleep quality, excessive daytime sleepiness, and other sleep traits. Multivariable logistic regression procedures were used to estimate adjusted odds ratios (AORs) and 95% confidence intervals (CIs).
Results
Migraineurs were more likely than non-migraineurs to report short sleep duration (<6.5 hours) (AOR = 1.47, 95% CI 1.07–2.02), poor sleep quality (PSQI>5) (AOR = 1.73, 95% CI 1.35–2.23), and daytime dysfunction due to sleepiness (AOR = 1.51, 95% CI 1.12–2.02). Migraineurs were also more likely than non-migraineurs to report taking sleep medication during pregnancy (AOR = 1.71, 95% CI 1.20–2.42). Associations were generally similar for migraine with or without aura. The odds of sleep disturbances were particularly elevated among pre-pregnancy overweight migraineurs.
Conclusion
Migraine headache and sleep disturbances are common comorbid conditions among pregnant women.
Introduction
Migraine, a neurological disorder, is marked by episodic disabling headache attacks that are often characterized by episodes of unilateral, severe throbbing, and pulsatile headache associated with nausea, vomiting, photophobia, phonophobia, and aversion to physical activity (1). Migraine is particularly common among women of childbearing age (2), with age-specific prevalence estimates for women of childbearing age ranging from 5% to 45% (2). Migraine attacks have been reported to diminish, disappear in most pregnant women, remain unchanged, worsen, or appear for the first time during pregnancy (3). Migraine headache has substantive adverse financial effects in the workplace due to associated disability, days of work lost to disability, and low work performance (4). Moreover, associations between a history of migraine and an increased risk of preeclampsia (5), placental abruption (6), and preterm delivery (7) have been previously reported.
Sleep disturbances, common complaints among migraineurs, have been identified as precipitating factors for headache attacks in some studies (8). Substantial literature indicates that sleep disturbances and migraine are closely related, with the latter having considerable impact on sleep quality (9,10). Insufficient sleep duration and poor sleep quality are considered to be endemic in modern society (11). According to the National Sleep Foundation’s 2007 Sleep in America Poll, poor sleep quality (27%) and daytime sleepiness (21%) are common among American women (11). Furthermore, pregnancy-associated physiological and hormonal changes are known to contribute to increased prevalence and severity of sleep disturbances and complaints among pregnant women (12). Sleep disturbances negatively affect the daily life of women. Notably, migraineurs often experience pain relief with sleep, while rest without sleep has been shown to be less effective (13). In addition, investigators have reported associations of migraine with prolonged sleep onset latency, increased wake after sleep onset, and reduced sleep efficiency in studies that used questionnaires (14–16) or actigraphy (17) to assess sleep disturbances. These observations were recently confirmed by a study that used polysomnography (PSG) to assess sleep disorders among migraineurs (18).
The high prevalence of migraine and sleep disturbances, together with the potential for co-occurrence of these disorders is a concern because of the disability attributable to both conditions. Furthermore, clinical diagnosis of one should lead to increased vigilance for screening and treating of the other. We are aware of only one publication that assessed the co-occurrence of migraine and sleep disorders among pregnant women (19). Given that there are few published reports on the co-occurrence of migraine and sleep disturbances among pregnant women, we examined the cross-sectional relationship between women’s history of migraine prior to pregnancy and early pregnancy sleep disturbances in a cohort of pregnant women.
Materials and methods
Study setting and study population
This study is based on 1324 pregnant women enrolled in the Migraine and Pregnancy Study, a prospective cohort study of pregnant women, enrolled during the period between November 2009 and March 2013. The Migraine and Pregnancy Study was designed to investigate the relationship between maternal history of migraine and risk of developing preeclampsia later in pregnancy. Participants were recruited from women attending prenatal care at clinics affiliated with Swedish Medical Center in Seattle, Washington. Women were ineligible if they initiated prenatal care after 20 weeks’ gestation, were younger than 18 years of age, did not speak and read English, did not plan to carry the pregnancy to term, or did not plan to deliver at Swedish Medical Center. The procedures used in the study were in agreement with the protocol approved by the institutional review board of Swedish Medical Center, Seattle, WA. All participants provided written informed consent.
Data collection
Participants completed a questionnaire administered by trained interviewers at enrollment in early pregnancy (14 weeks on average). Research methodologists, neurologists and perinatologists trained interviewers. Interviews were conducted in person at prenatal care clinics or on the phone. Information on maternal demographics and socioeconomic characteristics was collected as part of the interview. We used body mass index (weight (kg) divided by height2 (m2)) (BMI) as a measure of maternal adiposity. Pre-pregnancy BMI was computed based on maternal self-reported weight three months prior to pregnancy and on height measured during her initial prenatal visit. We used pre-pregnancy BMI instead of early pregnancy BMI (with measured weight at first prenatal visit) to avoid biases attributable to variations in the timing of prenatal care onset, variations in maternal experiences with early pregnancy maternal medical conditions (e.g. nausea, vomiting or hyperemesis gravidarum) and alterations in maternal early pregnancy diet and physical activity that may influence measured weight taken in prenatal care clinics. We categorized study participants into four groups as follows: <20.0 (lean), 20.0–24.9 (high normal), 25.0–29.9 (overweight), and ≥30.0 kg/m2 (obese). The interview included a structured migraine assessment questionnaire (adapted from the deCODE Genetics migraine questionnaire (DMQ3) (20) and an assessment of disability associated with headaches experienced before pregnancy. In a previous validation study, using a physician-conducted interview as an empirical index of validity, the deCODE Migraine Questionnaire (DMQ3) diagnosed migraine with a sensitivity of 99%, a specificity of 86%, and a kappa statistic of 0.89 (21). The detailed migraine-specific questionnaire used in current study contained questions addressing age at migraine onset, physician diagnosis of migraine, family history of migraine, details about migraine attacks, and medications used. Headache classification was determined using the International Classification of Headache Disorders, second edition (ICHD-II) criteria established by the International Headache Society (IHS) (22). Women with “any migraine” refer to the combination both of women with definitive migraine (IHS category 1.1) and probable migraine (IHS category 1.6). Migraine with aura (MA) was further defined using the IHS criteria (IHS category 1.2.1). Among the study cohort of 1324 pregnant women, we identified 375 participants with a history of “any migraine.” Among these 375 migraineurs, 123 women were identified as having a history of MA, and 252 were diagnosed with migraine with not history of having aura with their migraines (MO). Hence, our coding scheme allowed for two mutually exclusive and exhaustive groupings of women with a history of migraine (i.e. those with a history of migraine and a history of ever having experienced aura with a migraine episode; and those with a history of migraine, but never having experienced aura with their migraine episodes).
The early pregnancy interview and sleep-related characteristics were evaluated once using the Pittsburgh Sleep Quality Index (PSQI) (23). The PSQI is a 19-item self-reported questionnaire that evaluates sleep habits over the past month. The PSQI yields seven clinical components of sleep habits including sleep duration, sleep disturbances, sleep latency, habitual sleep efficiency, use of sleep medicine, daytime dysfunction due to sleepiness, and subjective sleep quality. Each sleep component yielded a score ranging from 0 to 3, with 3 indicating the greatest dysfunction (23). Subsequently, the sleep component scores are summed to yield a global sleep quality score (range 0 to 21) with higher scores indicating poor sleep quality during the previous month. Based on prior literature, participants with a global score >5 were classified as poor sleepers and those with a score ≤5 were classified as good sleepers (24). In accordance with PSQI for sleep quality subscales, subjective sleep efficiency, sleep latency, sleep medication use, and daytime dysfunction due to sleepiness, we computed a dichotomous variable of optimal and suboptimal sleep quality. Specific categories were long sleep latency (≥30 vs <30 minutes); estimates of poor sleep efficiency (<85% vs ≥85%); daytime dysfunction due to sleepiness (any vs never); and sleep medication use during the past month (any vs never). Sleep duration was assessed using the PSQI questionnaire, which queried how many hours per night a participant slept during the previous month. We also classified participants as short- (≤6 hours), normal- (7–8 hours), and long- (≥9 hours) duration sleepers. These categorizations were decided a priori, as decisions were guided by cut-points used by previous investigators, particularly those who focused on sleep disturbances among pregnant migraineurs (8).
Maternal report of snoring during early pregnancy was ascertained by asking women: “Since becoming pregnant, when you have been asleep, to the best of your knowledge, have you snored?” Response choices were: (1) none of the time; (2) a little of the time; (3) some of the time; (4) most of the time; and (5) all of the time. For multivariable analyses, we collapsed responses into a dichotomous variable with “no” comprising the responses none of the time, and “yes” comprising the other four responses.
We also used the Epworth Sleepiness Scale (ESS) to assess maternal excessive daytime sleepiness status during early pregnancy. Participants were asked to rate themselves on a scale of 0 to 3 (where 0 = would never doze; 1 = slight chance of dozing; 2 = moderate chance of dozing; and 3 = high chance of dozing). The scale yields a total score that ranges from 0 to 24, with higher ESS scores representing more severe subjective daytime sleepiness. Scores of 0–9, 10–12 and 13–24 are considered to represent normal, borderline and abnormal daytime sleepiness, respectively. For multivariable analyses, we created a dichotomous variable where participants with scores of ≥13 were classified as having excessive daytime sleepiness.
Statistical analysis
Maternal characteristics of study population according to migraine diagnosis.

Italic values indicate the subtypes. Data in mean ± SD or number (%). aP value from two-sample Student’s t test <0.05 when comparing any migraine to no migraine.
We evaluated the joint effect of migraine and pre-pregnancy overweight status on the risk of sleep disturbances. We classified women by the joint distribution of ICHD-II migraine diagnosis (no vs yes) and pre-pregnancy overweight status (<25 vs ≥25 kg/m2) resulting in the following categories: no migraine and no overweight; migraine and no overweight; no migraine and overweight; and migraine and overweight. This analytical approach allowed for estimating ORs for sleep disturbances among non-overweight women with migraine (i.e. to estimate the effect of migraine, independent of overweight/obese status) and the ORs for sleep complaints among overweight women without migraine (i.e. to estimate the effect of overweight status, independent of migraine status) when using non-overweight women without migraine as the referent group. The joint effect (or combined effect both of migraine and overweight status) was determined by comparing those positive for both characteristics with the referent group. Test for a linear trend across migraine and pre-pregnancy overweight categories was assessed by modeling the four-level variables as continuous. All analyses were performed using Stata 13.1 (Stata, College Station, TX) statistical analysis software. All reported confidence intervals were calculated at the 95% level, and all reported p values are two tailed.
Results
Approximately 28% (N = 375) of the cohort had a lifetime history of migraine based on ICHD-II criteria. Among pregnant women with history of migraine, 123 had MA and 252 had MO. Characteristics of women with no migraine, women with any migraine and their subclasses (MA and MO) are summarized in Table 1. Women with any migraine were more likely to have a family history of migraine or headache and to be overweight and obese when compared with women who did not have migraine. Women with a history of MA, as compared with MOs, were more likely to report that their index pregnancy was unplanned; otherwise the two groups were similar for other socio-demographic, medical history and behavioral characteristics.
Summary of Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale, and sleep duration according to migraine status.

Italic values indicate the subtypes. aP value in two-sample Student’s t test or Rank sum test when comparing any migraine to no migraine. bP value from ANOVA or Kruskal-Wallis nonparametric ANOVA across three groups (no migraine, migraine without aura, and migraine with aura). IQR: interquartile range; ANOVA: analysis of variance.
Pittsburgh Sleep Quality Index (PSQI) components by migraine status.

Italic values indicate the subtypes.
Adjusted odds ratios (AOR) and 95% confidence intervals (CI) for sleep characteristics according to migraine status.
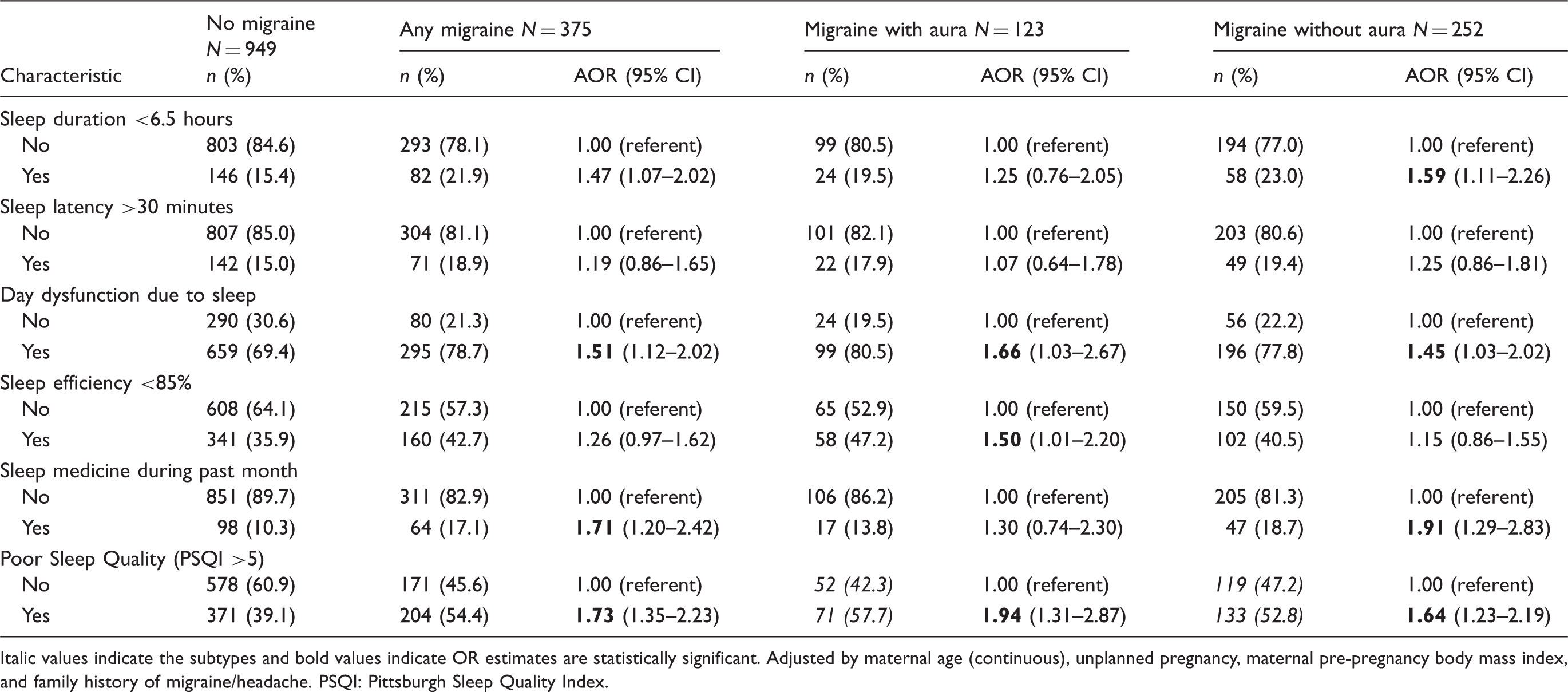
Italic values indicate the subtypes and bold values indicate OR estimates are statistically significant. Adjusted by maternal age (continuous), unplanned pregnancy, maternal pre-pregnancy body mass index, and family history of migraine/headache. PSQI: Pittsburgh Sleep Quality Index.
Adjusted odds ratios (AOR) and 95% confidence intervals (CI) for maternal sleep characteristics according to migraine status.
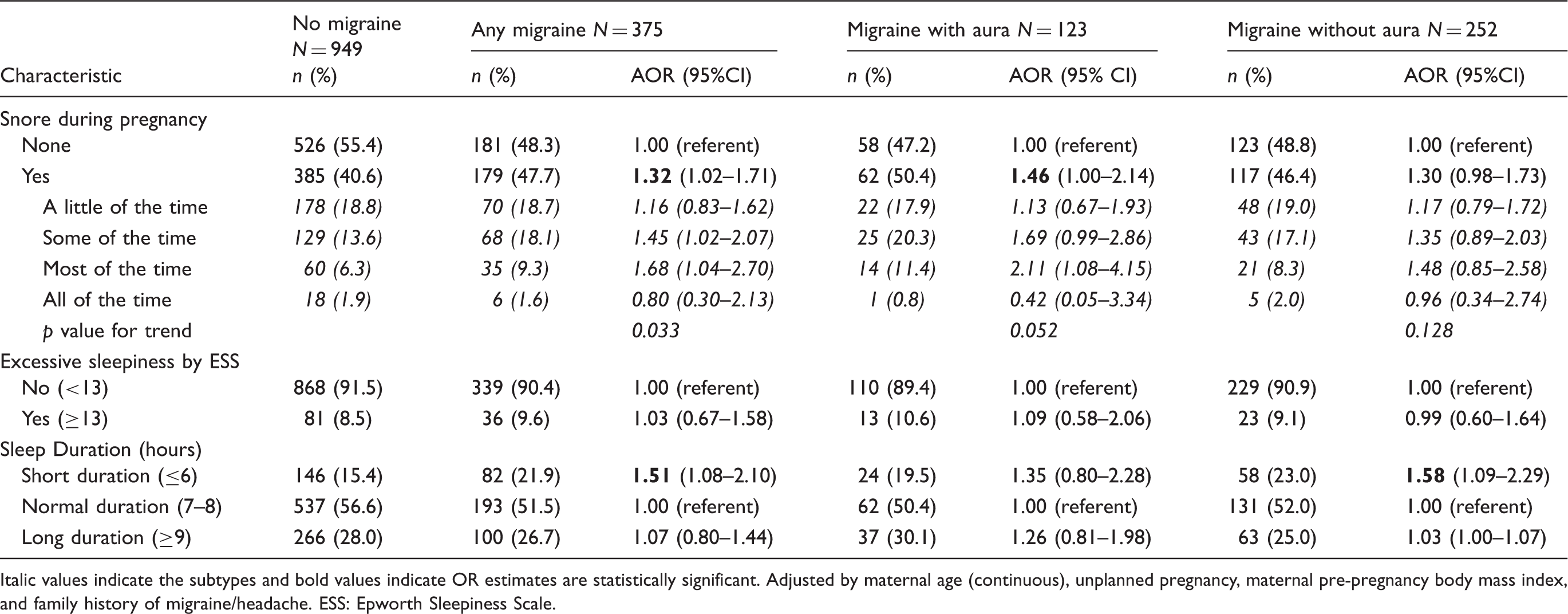
Italic values indicate the subtypes and bold values indicate OR estimates are statistically significant. Adjusted by maternal age (continuous), unplanned pregnancy, maternal pre-pregnancy body mass index, and family history of migraine/headache. ESS: Epworth Sleepiness Scale.
We evaluated the joint effect of migraine and pre-pregnancy overweight status (Supplemental Table 1) and noted that overweight migraineurs, compared with lean non-migraineurs, had the highest odds of short sleep duration, long sleep duration, long sleep latency, snoring, sleep medication use, daytime dysfunction, and being poor sleeper (PSQI >5) during pregnancy. Compared with lean non-migraineurs, the multivariable-adjusted ORs among overweight migraineurs for short sleep duration (≤6 hours) during early pregnancy was 3.40 (95% CI 2.07–5.60). Statistically significant associations were also observed for long sleep duration during pregnancy (AOR = 1.92; 95% CI 1.18–3.12), long sleep latency (AOR = 1.70; 95% CI 1.04–2.77), taking sleep medicine (AOR = 2.27; 95% CI 1.33–3.88), daytime dysfunction (AOR = 2.31; 95% CI 1.36–3.94) and being a poor sleeper (AOR = 2.72; 95% CI 1.79–4.11) among overweight migraineurs during early pregnancy.
Sixty-eight participants in our cohort met the diagnostic criteria for tension-type headache (TTH), with only four of them meeting the diagnostic criteria for migraine. Of note, the mean and standard deviation for PSQI scores for these 68 individuals with TTH was 5.6 ± 3.2, which is comparable to those non-migraineurs (5.3 ± 2.8). We completed a sensitivity analysis after excluding the 68 participants with TTH. The sensitivity analysis after excluding the TTH cases did not change the results. For instance, we found that after excluding the 68 individuals with THH, the AOR and 95% CI for poor sleep quality (PSQI score >5) was OR = 1.79 (95% CI 1.39–2.32) for all migraineurs; OR = 1.72 (95% CI 1.28–2.30) for MOs and 1.96 (95% CI 1.32–2.91) for MAs, respectively (data not shown).
Discussion
Approximately 28% of the cohort had an ICHD-II diagnosis of migraine. Overall, migraineurs (regardless of the presence or absence of aura) were more likely than non-migraineurs to report short or long sleep durations, daytime dysfunction, sleep medication use, snoring during pregnancy, and overall poor sleep quality based on the PSQI. The magnitude of association did not differ significantly among MAs or MOs. The odds of sleep disturbances were particularly elevated among overweight migraineurs when compared with lean non-migraineurs.
The findings from this study are similar to those from previous population-based studies of men and non-pregnant women (15,16,25) as well as children and adolescents (26). For example, using samples from United States adults, Lateef et al. reported a significant association between frequent severe headache, including MA and MO, and disordered sleep (25). Adults migraineurs reported more frequent difficulty initiating sleep (OR (95% CI): 2.0 (1.6–2.5)), difficulty staying asleep (2.5 (2.1–3)), early morning awakening (2.0 (1.7–2.5)), and daytime fatigue (2.6 (2.2–3.2)) and also were more than twice as likely to report three or more of these symptoms (2.5 (2.0–3.1)) compared to individuals without migraine (25). Walters et al. (16) identified 26.7% participants who met ICHD-II criteria for episodic migraine among 292 undergraduate students (70% female) and found that, compared with non-migraineurs, migraineurs reported poor sleep quality (PSQI global score: 8.9 ± 3.4 vs 6.6 ± 3.0, p < 0.001), with 86% reporting clinically significant poor sleep quality (vs 62% of controls, p < 0.005). Poor sleep quality was also significantly associated with headache frequency and disability due to headache (16). Sadeghniiat et al. (15) also found a positive correlation between migraine headache severity score and PSQI score (ρ = 0.6, p < 0.001). Taken together, these findings support hypothesized relationships between sleep deprivation and enhanced response to pain stimuli (27). Furthermore, our results, and those of others (15,16,25,26) are in general agreement with observations suggesting the importance of sleep disturbances as common triggers of migraine attacks (28).
The results from our study are also consistent with the few available studies that have assessed sleep traits using PSG methods (18,27). In a hospital-based study of 30 migraineurs without aura, Karthik and colleagues reported that migraineurs had longer latency to sleep onset, less non-rapid-eye-movement (NREM) sleep, lower arousal-index, more awakenings, longer time in bed, and more awake time as compared with 32 healthy controls (all p values < 0.05) (18). Furthermore, Engstrøm et al. (27) reported that migraineurs were more likely to endorse subjective sleep problems (in response to the PSQI) and to have poor sleep quality (measured objectively using the PSG methodology).
Results from population-based studies suggest that obesity is a risk factor for migraine, and both MA and obesity are known risk factors for cardiovascular disease (29). Furthermore, risk factors like migraine and obesity are associated with metabolic profiles such as reduced adiponectin concentrations (30) and elevated concentrations of pro-inflammatory cytokines suggestive of systemic inflammation, risk factors of neurovascular and cardiovascular disorders (31). We evaluated the joint effect of migraine and maternal overweight status and noted that overweight migraineurs had the highest odds of short sleep duration or long sleep duration, long sleep latency, snoring, sleep medication use, daytime dysfunction, and being poor sleepers (PSQI >5) during pregnancy.
The generally accepted biological mechanism for the observed association between migraine and poor sleep involves alterations of serotoninergic or dopaminergic neurotransmitter pathways (9). For example, the structure that is involved in migraine initiation is the trigeminal nucleus caudalis in the pons and midbrain as well as the hypothalamus, commonly considered to be dopaminergicaly modulated. The hypothalamus is connected with the limbic system, the pineal gland, and the serotonergic dorsal raphe, anatomical structures that are also involved in the control of the sleep-wake cycle as well as in the modulation of pain (10). Individuals susceptible to migraine appear to have genetic polymorphisms in the dopamine D2 receptor gene, which is also associated with sudden onset of sleep in dopaminergic agent users (32). The result is an imbalance of the dopaminergic system, which is responsible for some premonitory symptoms of migraine (33). Finally, melatonin, a chronological hormone, has some demonstrated therapeutic efficacy in some forms of migraine and headache (34).
The strengths of our study include the relatively large number of women with information from the detailed standardized questionnaire allowing us to apply ICHD-II criteria for migraine diagnosis in a large sample of pregnant women. We also had available data on migraine-related features of aura that allowed us to separately examine the association between MA or MO and sleep disturbance. However, some important limitations must be considered when interpreting the results of our study. First, the PSQI is primarily a subjective estimate of sleep quality and may have limitations in clinical diagnosis of sleep quality. While subjective estimates and objective measures of sleep such as PSG differ in actual amount, they are often moderately correlated (35). Second, the cross-sectional data collection design of our study does not allow for determination of the temporal relationship between poor sleep quality and migraine. Lastly, participants in this cohort were largely non-Hispanic white, well-educated and reported moderate to high annual household incomes; hence findings from this study may not be generalizable to all other obstetric populations.
Despite noted study limitations, our results are consistent with a larger body of work documenting associations between migraine and sleep disturbances in men and non-pregnant women (15,16,25,26). Enhanced understanding of the epidemiology and shared pathophysiological mechanisms between headaches and sleep disturbances is expected to provide important information for enhancing the diagnosis and treatment of these disorders in pregnant women.
Clinical implications
Migraineurs were more likely than non-migraineurs to report sleep disturbances based on the Pittsburgh Sleep Quality Index (PSQI). The magnitude of association did not differ significantly among migraineurs with aura or without aura. The odds of sleep disturbances were particularly elevated among overweight migraineurs when compared with lean non-migraineurs.
Footnotes
Funding
This work was supported by an award from the National Institutes of Health (R01HD-055566).
Conflict of interest
None declared.
Acknowledgment
The authors are indebted to the staff of the Center for Perinatal Studies for their expert technical assistance.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.