
Abstract
Abstract
Objective
This study aims to investigate pregnancy and perinatal outcomes in women with tension-type headache, migraine without aura and migraine with aura by comparing them to women without any headache disorders.
Study design
Prospective cohort study including singleton pregnancies attending the first trimester aneuploidy screening at the University Hospital of Modena, in Northern Italy, between June 2018 and December 2019.
Results
A total of 515 consecutive women were included and headache disorders were reported in 43.5% of them (224/515). Tension-type headache was diagnosed in 24.3% of the cases, while 14% suffered from migraine without aura and 5.2% from migraine with aura. Birthweight was significantly lower in women affected by migraine with aura respective to other groups, and a significantly higher rate of small for gestational age infants was found in tension-type headache (10.4%) and in migraine with aura (24.9%) groups respective to the others (p < 0.001). Moreover, the admission to the neonatal intensive care unit was significantly higher in all the headache groups (p = 0.012). Multivariate analysis showed that women presenting tension-type headache (OR 4.19, p = 0.004), migraine with aura (OR 5.37, p = 0.02), a uterine artery pulsatility index >90th centile (OR 3.66, p = 0.01), low multiple of the median (MoM) of Pregnancy-associated plasma protein-A (PAPP-A) (OR 0.48, p = 0.05) and high MoM of Inhibin-A (OR 3.24, p = 0.03) at first trimester, are independently associated with the delivery of small for gestational age infants when compared to women without headache disorders.
Conclusion
Migraine with aura and tension type headache expose women to an increased risk of delivering small for gestational age infants, in association with some utero-placenta markers evaluated at first trimester. These women with headache disorders have an additional indication to undergo first trimester aneuploidy screening and would possibly benefit from specific interventions.
Introduction
Headache during pregnancy should be investigated because it can be a symptom of secondary conditions, including cerebral vascular thrombosis, hypertensive disorders, stroke, and pituitary apoplexy (1). On the other hand, pre-existing primary headache conditions, can influence the course of pregnancy and delivery leading to a higher risk of vascular and hypertensive complications. Indeed, pre-existing migraine is correlated with ischemic and hemorrhagic stroke, myocardial infarction, thromboembolic conditions and pregnancy-related hypertension (2–5). A prospective study performed by our group confirmed the strong correlation between migraine and hypertensive disorders and also demonstrated that the risk is exacerbated in women who still suffer with migraine during pregnancy. Such women showed an increased risk of preeclampsia associated with a low birth weight, independent from age, smoking or other already known risk factors (6). Moreover, a more recent retrospective study performed in the African-American and Hispanic population suffering from migraine during pregnancy shows a higher risk of developing preeclampsia, preterm labour and lower birth weight (7).
However, few studies investigated other primary headache conditions during pregnancy. In a sample of pregnant women suffering from migraine and tension-type headache (TTH) a higher risk of abruptio placenta was reported (8). A further Italian study demonstrated that women suffering from headache disorders although not distinguishing migraine and tension type headache showed an increased incidence of small for gestational age (SGA) neonates in women with cephalalgia (9). Moreover, no specific studies are available about the possible correlations between tension-type headache and pregnancy complications.
On this ground, our prospective study aims to deep evaluate pregnancy and perinatal outcomes in women with tension-type headache (TTH), migraine without aura (MwoA) and migraine with aura (MA) in a cohort of women attending the first trimester aneuploidy screening. This leaves the possibility to look at markers of vascular and placental function and relate them with adverse perinatal outcomes.
Materials and methods
A population of singleton pregnancies between June 2018 and December 2019 were included in the prospective study. All women attended to the first trimester aneuploidy screening at the University Hospital of Modena (North of Italy).
The study was approved by Local Ethical Committee (protocol AOU: 0001395/20). Women were included if the embryo looked healthy, with crown–rump length ranging 45–80 mm and no signs of miscarriage. Pregnancies with major fetal abnormalities, twins and those with a maternal age of <18 years were excluded from the study. Before inclusion, a written consent to participate in the study was obtained.
A validated questionnaire with 32 questions asking for general and gynecological/obstetrical history and headache symptoms was administered to the women (10). In the sub-group of women reporting headache the presence of migraine without and with aura was investigated throughout the ID migraine questionnaire, also known as PIN (photophobia, impairment, nausea). Two out of three symptoms were considered enough to diagnose migraine. This questionnaire was previously validated in the Italian language in a mixed population of men and women (11).
For MA diagnosis, we used the visual aura rating scale (VARS), based on the International Headache Society’s diagnostic criteria. The VARS score is the weighted sum of the presence of five visual symptom characteristics: duration 5–60 min (3 points), gradual development over at least 5 minutes (2 points), scotoma (2 points), zig-zag lines (2 points), and homonymous hemianopia (1 point). A VARS score of 5 or more out of a maximum score of 10 points has a sensitivity of 96% [95% CI 92–99%] and a specificity of 98% [95% CI 95–100%] for migraine aura (12). It has been validated in Italian version (10). The classification of headache disorders was considered mutually exclusive.
Each woman admitted for the first trimester aneuploidy screening underwent to a first trimester algorithm of the Fetal Medicine Foundation for preterm preeclampsia prediction (13). The algorithm utilizes mean arterial blood pressure (MAP), uterine artery Doppler and various biochemical markers as such as Placental Associated Plasma Protein-A (PAPP-A) and Placental Growth Factor (PlGF) (14,15). We also added Inhibin-A, a possible predictor of abnormal fetal growth (16).
A blood sample was collected in fasting conditions and the serum centrifuged and stored at minus 80° C, for subsequent biochemical analyses. The biochemical markers have been measured with the automated DELFIA EXPRESS system (Thermo Fisher Scientific, MA, USA).
The MAP was measured with validated automated devices (Dinamap, BLTV6XX). After the women were seated and allowed to rest for 3–5 min, adult cuffs (22–32 cm) were fitted to both their arms. This was repeated two times with 1 min break in between. The MAP was calculated with the formula MAP = DBP + 1/3(SBP–DBP) (DBP represents diastolic blood pressure and SBP the systolic blood pressure). We calculated the final MAP as the average of all four measurements (17). Uterine artery Doppler studies including pulsatility index were measured through trans-abdominal ultrasound examinations (Voluson E10). All ultrasound and Doppler studies were carried out by a physician who had received the appropriate certificate of competence from the Fetal Medicine Foundation (13).
Finally, data on pregnancy outcome such as weight gain according to the Institute of Medicine (IOM) recommendations, gestational diabetes, stillbirth, abruptio placenta, gestational hypertension and preterm delivery were collected from the hospital maternity records or directly from patients if delivered in another setting. Medical records were reviewed by research associates to obtain anonymized data on mothers and their newborns and included birthweight, gender, Apgar scores, admission to the neonatal intensive care unit (NICU), length of stay, neonatal morbidities, and mortality. Neonatal anthropometric measures were collected to define newborns as small, appropriate, or large for gestational age (SGA, AGA, LGA, respectively) according to the Italian curves for neonatal growth validated by Bertino et al. 2010 (18). These curves/charts take into account not only the birthweight (BW), but also the body length (BL), and head circumference (HC), sex, and birth order. Therefore, neonates whose BW, BL and HC values fell below the 10th centile were considered SGA. All data were organized in a password protected database.
Statistical analysis
Stata 16.1 (StataCorp. 2019. College Station, TX, USA) was used to analyze data. Statistical tests were designed to compare pregnancy and perinatal outcomes in women with different headache diagnoses. Comparisons between groups were made using a One-way ANOVA test for continuous variables and chi-square test for categorical ones.
The multivariable model was developed by carrying out the following steps. Firstly, univariate logistic regression models were used to assess the relationship among each relevant independent variable and the risk of having a SGA infant. The variables that were associated to SGA risk with p-value <0.05 in the univariate analyses were considered for inclusion in a multivariable logistic model. The final model was determined by a stepwise backward selection procedure in which only independent variables associated to SGA risk with p-value < 0.05 were retained. Results of logistic models were reported as the Odds Ratio (OR) with 95% confidence interval and Wald p-value.
Continuous data are reported as mean ± standard deviation (SD). Categorical data are reported as the absolute and percentage frequencies. All probability values were 2-tailed, and a probability value of <0.05 was considered statistically significant.
Results
Headache disorders were reported in 43.5% of the women (224/515). In detail, 125 (24.3%) suffered from TTH, 72 (14%) from MwoA and 27 (5.2%) from MA.
Maternal baseline features did not differ in women with or without headache disorders except for the smoking habit which significantly higher in women suffering from TTH (Table 1).
Maternal baseline features.

Continuous data are reported as mean ± standard deviation (SD). Categorical data are reported as the absolute and percentage frequencies. A p value lower than 0.05 was considered significant.
Women suffering from headache reported similar pregnancy complications than unaffected women, as shown in Table 2. Also, no differences were observed in labour inductions (due to pregnancy complications) as well as in the rate of caesarean section. Relevant biochemical and biophysical markers are reported in Table 3, it is worth noting that PAPP-A MoM levels are significantly lower among TTH and MA women, while the other markers resulted to be similar among groups.
Pregnancy outcomes data.
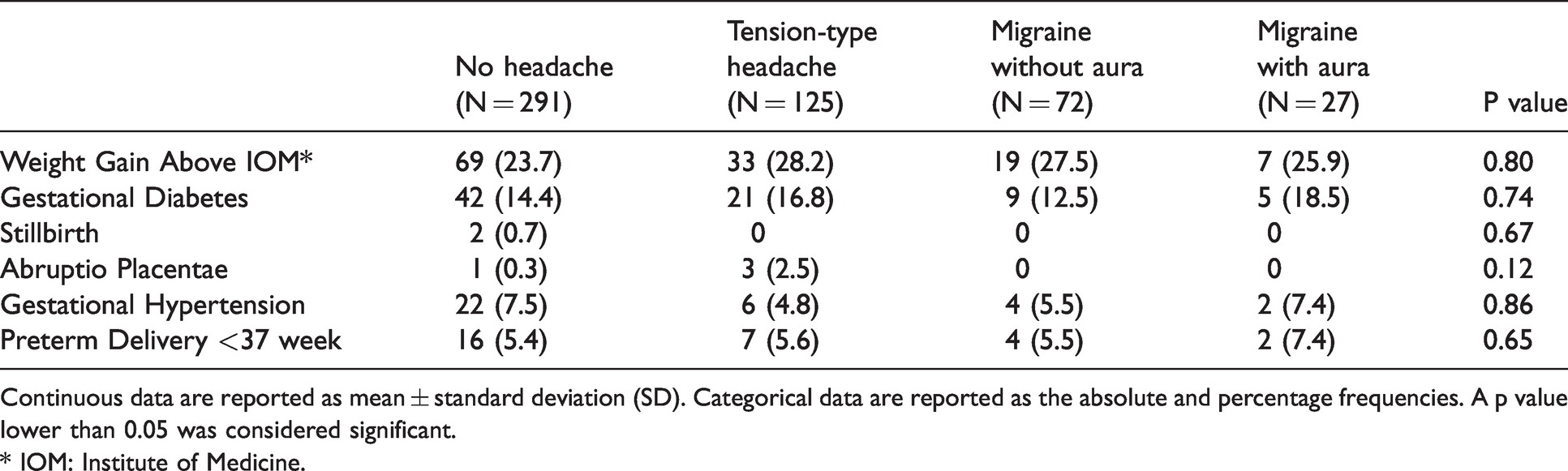
Continuous data are reported as mean ± standard deviation (SD). Categorical data are reported as the absolute and percentage frequencies. A p value lower than 0.05 was considered significant.
* IOM: Institute of Medicine.
Biochemical and biophysical markers during pregnancy.

Continuous data are reported as mean ± standard deviation (SD). Categorical data are reported as the absolute and percentage frequencies. A p value lower than 0.05 was considered significant.
*MoM: multiple of the median.
On the contrary, birthweight was significantly lower in women affected by MA in respect to other groups. Indeed, they showed a significantly higher rate of SGA than the remnants (Table 4). The indicators of neonatal hypoxia as low venous pH (≤7.2) in umbilical cord blood and Apgar score at 5th minute ≤7 were similar between groups while the admission rate to the neonatal intensive care unit (NICU) was significantly higher in all the headache diagnostic groups.
Neonatal outcomes data.

Continuous data are reported as mean ± standard deviation (SD). Categorical data are reported as the absolute and percentage frequencies. A p value lower than 0.05 was considered significant.
Multivariate analysis showed that women presenting TTH (OR 4.19, p = 0.004) or MA (OR 5.37, p = 0.02), a mean uterine artery doppler PI > 90° centile (OR 3.66, p = 0.01), low levels of PAPP-A (OR 0.48, p = 0.05) and high levels of Inhibin-A (OR 3.24, p = 0.03) at first trimester are more likely to deliver SGA infants as compared to women without any headache disorders (Table 5).
Logistic regression for the risk of SGA infant.

A p value lower than 0.05 was considered significant.
Discussion
This prospective study reported perinatal outcomes of women suffering from different headache disorders, in a sample of women undergoing genetic prenatal screening. In such reproductive age group, it is confirmed that a significant proportion of women suffer from headache disorders, and the prevalence of the main headache subtypes agrees with previously reported cases series (1,19).
A specific adverse outcome characterizes both women suffering from MA and TTH, i.e. a higher rate of SGA, together with an increased rate of neonates admitted to intensive care unit. This finding partly corroborates previous data which reported an increased risk for low birthweight babies in different migraine populations (5,6). However, neither of the previous studies unfortunately differentiate among migraine with or without aura. It is generally accepted that pregnancy has a positive effect relieving MwoA attacks while MA symptoms remain unchanged (20). Our study, however, cannot add information over headache course and drugs use since follow-up was not planned, also considering that drugs, namely triptans, seem not to affect pregnancy outcomes (21). Anyway, among the two main forms of migraine it becomes apparent that MA shows worst perinatal outcomes, and future research should concentrate on this relatively less common form of headache.
Fetal growth is affected by several factors including maternal anthropometry, placenta activity and vascular adaptation to pregnancy (22). An abnormal fetal growth could be the result of different factors such as obesity, excessive weight gain and unhealthy behaviors including smoking (23–25). Although a smoking habit is effectively more prevalent in women with TTH in our cohort (while not associated with MA), this factor does not enter the multivariate analysis for the risk of SGA while utero-placental markers did so. Indeed, low PAPP-A and increased Inhibin-A levels at first trimester together with increased uterine artery resistances are significantly associated with SGA babies.
PAPP-A, secreted by syncytiotrophoblast and detected in maternal serum, placental tissue, amniotic fluid is an enzyme that cleaves insulin-like growth factor binding protein thereby increasing bioactivity of insulin-like growth factors in the fetal compartment (26). Low PAPP-A serum levels indicate impaired placentation, and its growth regulatory activity explains the already demonstrated inverse relationship between its levels and the incidence of fetal growth restriction (26–28). Interestingly, also Inhibin-A has been found to be related with fetal growth abnormalities (16).
On the other hand, the relationship between migraine and gestational hypertension, we and others already reported (6,7), was not confirmed in this cohort. In addition to the actual small sample size being unable to correctly detect a low-incident phenomenon, this was possibly due to the diverse features of the population, as well as the recent popularity of low-dose aspirin administration reported to reduce the onset of hypertensive disorders of pregnancy, namely preeclampsia (29).
Headaches and preeclampsia are characterized by platelet hyper aggregation, decreased prostacyclin production and endothelial dysfunction leading to a poor vascular adaptation (30), to pregnant status. The increased uterine artery resistances at first trimester we found and the well-known related reduced fetal growth (31) is just another clinical expression of impaired vascular adaptation, different than maternal hypertension/preeclampsia. Interestingly, in patients affected by migraine decreased serum VEGF angiopoietin-2 and thrombopoietin compared to controls has been found. The two substances are associated with both endothelial dysfunction and increased risk of vascular disorders (32,33).
An increased rate of NICU admission was found in all headache groups and therefore cannot be solely attributed to SGA which represents an obvious indication. Since the reduced number of this outcome, it is not possible to identify other neonatal explainitory conditions, in addition to prematurity. Certainly, increased neonatal admission cannot be attributed to intrapartum events, since the occurrence of acidemia at birth was found irrespective of headache diagnosis.
In conclusion, migraine with aura and tension type headache expose women to an increased risk of delivering SGA infants, in association with some utero-placenta markers evaluated at first trimester. Thus, those categories of women have an additional indication to underwent first trimester aneuploidy screening and would possibly benefit from specific interventions.
Clinical implications
This study confirms that headache disorders in pregnancy are associated with unfavorable perinatal outcomes with an increased rate of NICU admission irrespective of headache diagnoses. Migraine with aura and tension type headache expose women to an increased risk of having SGA infants together with markers of vascular and placental adaptation to pregnancy. These categories of women have an additional indication to undergo first trimester aneuploidy screening and would possibly benefit from specific interventions.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.