
Abstract
Objective
The objective of this article is to compare acute primary headache patient outcomes in those initially treated with parenteral opiates or non-opiate recommended headache medications in a large academic medical emergency department (ED).
Background
Many acute primary headache patients are not diagnosed with a specific headache type and are treated with opiates and nonspecific pain medications in the ED setting. This is inconsistent with multiple expert recommendations.
Methods
Electronic charts were reviewed from 574 consecutive patients who visited the ED for acute primary headache (identified by chief complaint and ICD9 codes) and were treated with parenteral medications.
Results
Non-opiate recommended headache medications were given first line to 52.6% and opiates to 22.8% of all participants. Patients given opiates first had significantly longer length of stays (median 5.0 vs. 3.9 hours, p < 0.001) and higher rates of return ED visits within seven days (7.6% vs. 3.0%, p = 0.033) compared with those given non-opiate recommended medications in univariate analysis. Only the association with longer length of stay remained significant in multivariable regression including possible confounding variables.
Conclusions
Initial opiate use is associated with longer length of stay compared with non-opiate first-line recommended medications for acute primary headache in the ED. This association remained strong and significant even after multivariable adjustment for headache diagnosis and other possible confounders.
Introduction
Non-opiate first-line recommended parenteral agents for acute primary headache in the ED from prior research.

Migraine headache-specific treatment. ED: emergency department; NSAID: nonsteroidal anti-inflammatory drug.
Despite the many recommendations, parenteral opiates remain one of the most widely used medications for the treatment of acute migraine or primary headache for patients presenting to the EDs in the United States. Prior studies have shown parenteral opiates are given to 25%–60% of these patients (3,16,17). Multiple expert reviews have reported that opiates should not be used as first-line therapy for migraine headaches in the ED or clinic (9,19–22). A recent American Academy of Neurology recommendation from the Choosing Wisely campaign advises against using opiates, except as a last resort for migraine (23). Additionally, opiates are not recommended in the treatment of tension-type headache (14), which, after headache NOS and migraine, is the third most common primary headache in the ED (3). Headache persistence and recurrence with opiate use is more common than when using headache-specific medications for migraine and tension-type headaches (9). Migraine-specific studies have also shown opiates to be associated with increased length of hospital stay, more rescue medications (24) and increased rates of return ED visits (20,25).
Unspecified diagnosis of primary headache in the ED may have a significant effect on treatment choice. Headache NOS makes up a large portion of headache patients in nationwide EDs (4–6), but this is likely due to a vast under-diagnosis of more specific headache types. Up to 89% of ED diagnosis of non-migraine headache were changed to migraine or transformed migraine in a single-center chart review (26). Nonspecific pain medications like opiates are likely overused in this headache NOS population because of under-diagnosis of specific headache types such as migraine or tension headache. Thus, a large proportion of those with headache NOS could likely be more effectively diagnosed and specifically treated in the ED following prior research recommendations.
Without a clear algorithm or treatment recommendations for primary headache patients in the ED, treatment is based on the individual physician’s discretion. We provide analysis of a large number of primary headache patients who were diagnosed and treated at a single, large academic ED with various parenteral medications (at the discretion of the treating emergency physician) and explore differences in medication treatment choice and final diagnosis, revisit rates, and length of hospital stay. Since parenteral medications, rather than oral agents, are the most well-studied and effective medications for treatment of acute primary headache in the ED (9,19), we limited our analysis to parenteral agents. To our knowledge this is the largest comprehensive review of primary headache patients with parenteral treatment and return visit data in an ED population.
Our objectives were to determine if non-opiate first-line recommended medications for acute primary headache were associated with improved patient outcomes regardless of specific headache diagnosis. Our pre-determined treatment categories of interest were parenteral opiates compared with non-opiate recommended first-line headache medications derived from prior expert and society reviews and guidelines (see Methods and Table 1). Our primary outcome measures were length of hospital stay and return ED visits for recurrent headache. Secondary outcomes included discharge pain scores and total number of headache medications used. Potential confounders including orders for neuroimaging (a measure of diagnostic uncertainty), specific headache discharge diagnosis, and initial triage headache pain scores were included for multivariable analysis. We hypothesized based on prior migraine-specific research that acute primary headache patients initially given opiates would have longer hospital stays and more frequent return visits compared with those initially given non-opiate first-line recommended medications.
Methods
Study design
The study is a retrospective electronic chart review using data collected and stored in a clinical research database (using STRIDE) (27). Study dates (May 1, 2011 to September 1, 2012) were chosen based on the first date (May 1, 2011) on which complete records of ED visits including medications given were regularly included in the research database. This study was approved by the Stanford University Institutional Review Board.
Data collection
All study data were obtained directly from the electronic medical record (EMR) clinical research database and were entered into the EMR for routine clinical care. International Classification of Diseases, ninth revision (ICD9) codes that were entered into the EMR for clinical care (by providers) and billing (by professional medical coders) were used to document headache types and co-occurring diagnosis. Medications given were entered electronically into the EMR when administered by nursing staff as part of routine clinical care. Pain scores were recorded in the EMR as routine patient care by nursing staff from patient-reported pain values 0–10 (10 is worst pain, 0 is no pain). Length of stay was calculated from the difference between the recorded discharge time and the ED arrival time.
Participants
All consecutive patients aged 18 and older who presented to the Stanford Emergency Department during the study period with a chief complaint of headache or migraine and a discharge diagnosis of headache were considered for inclusion. Discharge diagnosis of headache was determined by an ICD9 code of headache NOS (784.0), tension headache (307.81), migraine (346.*), or other headache syndrome (339.*).
Individuals were excluded from analysis if any secondary cause for headache was identified by the researchers in review of their ICD9 coded problem lists. Reasons for exclusion were derived from the definitions of primary headache from the International Classification of Headache Disorders (28). Additional individuals were excluded if they had a significant diagnosis that would limit options for headache treatment such as current pregnancy, recent hemorrhage, coagulopathy, or acute or chronic renal failure.
Patient data were anonymized before download from the clinical research database and no demographic information or personally identifiable information was obtained for this research.
Non-opiate first-line recommended medications
Parenteral medications were categorized as first-line recommended based on a compilation of prior evidence-based society and expert recommendations for treatment of acute migraine, tension, and other primary headache (see Table 1). Medications were classified as first-line recommended treatments if they were included as recommended in both a recent systematic review of acute migraine treatments (9) and also in the recent Canadian Headache Society guideline for acute migraine treatment in the ED (29) or were recommended as best evidence parenteral treatment of acute tension-type headaches by the European Federation of Neurological Societies (EFNS) guideline (14). Intranasal lidocaine, intravenous magnesium, droperidol, ergotamine, and promethazine were excluded from the final recommended list as they were not included as recommended agents in both migraine reviews. Aspirin and acetaminophen were included as recommended parenteral treatment of tension headache from the EFNS guidelines.
Medications given to each patient were sorted by their recorded administration times (recorded by nursing routinely on administration) and medications given first (alone or in combination if administered within five minutes of the first medication, a cutoff used in a prior study (30)) were used for comparison. Combinations of medications were categorized as opiates or non-opiate first-line recommended agents or non-opiate other medications. Combinations of initial medications that included first-line recommended agents with opiates (e.g. metoclopramide and morphine) were included in the opiates category.
Diagnostic and outcome variables
Variables attainable from our dataset with known or suspected association with headache treatment and outcomes were included for evaluation for possible confounding in our analysis. These included headache severity, number of medications given, neuroimaging performed, duration of hospital stay, and return ED visits. Headache pain severity was dichotomized into severe (7–10) and not severe (0–6) based on prior research into the numeric pain scale (31). Missing data in our dataset were found only for pain scores (17% of encounters did not have pain scores recorded) and missing values were imputed to the median values for initial (median 5) and discharge (median 2) pain scores for analysis.
Outcome variables of interest were based on prior study associations with migraine treatment and included length of stay and early return visits. Duration of ED stay was dichotomized for ease of interpretation as a “long stay” based on the 75th percentile of the duration of stay in the study population (six hours). Return visits were dichotomized as “early return visit” or not, to assess for recurrent headache with ED return visit within seven days of initial visit, which is similar to a previous study (25). In analysis of return visits, only a patient’s first early return visit after the index visit was counted in the analysis, and subsequent return visits were censored from analysis.
Statistical analysis
Statistical analysis was performed using STATA version 10 (Stata Corp LP, College Station, TX). Patient data were included only from the first ED visit during the study period and any subsequent encounter data were used only to determine days until return ED visit. Descriptive statistics for nonparametric variables are listed as medians with interquartile range (IQR) (25%–75%). Alpha was set at 0.05 for statistical significance and hypothesis testing was two tailed. Comparison between nonparametric variables (e.g. hours of stay) were performed using the Mann-Whitney Rank-Sum test and proportions with the Chi-square test. Univariate logistic regressions were used to compare binary outcomes with reporting of odds ratios, 95% confidence intervals, and p values. Multivariable logistic regression analysis was performed with the primary study outcomes of a long ED stay (>6 hours) and rate of early return visits. The final multivariable models included only pre-specified diagnostic or initial patient level variables with significant univariate associations with the outcome. Statistical interaction was measured in the final models by including the interaction terms in the logistic regression.
Results
Participants
There were a total of 2849 unique patients seen in the ED during our study period where the chief complaint and discharge diagnosis included headache or migraine. Of those encounters, 1114 (39.1%) had an alternative primary discharge diagnosis or a possible secondary headache etiology. The most common alternative or secondary headache diagnosis was fever or infection in 524 (18.4%) followed by trauma in 294 (10.3%) and pre-existing or incident intracranial lesions in 77 (2.7%). Furthermore, 415 (14.6%) were excluded for a diagnosis that would have limited or influenced initial medication choice for a primary headache such as pregnancy, active bleeding, coagulopathy or renal or hepatic failure. Of the remaining 1320 unique patients, we excluded 744 (56.4%) from analysis who received an oral headache medication rather than parenteral medication as their first-line treatment. The remaining 574 individuals who were included for final analysis had all visited the ED during our study period with a chief complaint of headache and a principal discharge diagnosis of headache, without significant complicating comorbidities, and received a parenteral first-line headache treatment.
Diagnosis
At their initial ED visit during the study period, participants had discharge diagnosis of headache NOS in 420 (73.2%), migraine headache in 138 (24.0%), tension headache in 11 (1.9%), cluster headache in five (0.9%) and occipital neuralgia in one individual. One patient was coded both with migraine and tension headaches. The most common non-headache co-occurring diagnostic codes were, in order of frequency: nausea and/or vomiting, dizziness and giddiness, hypertension, numbness, neck pain, chest pain, generalized weakness, dehydration, near syncope, and photophobia.
Medication treatments
Initial treatment with parenteral medication by headache diagnosis—alone or in initial combination.

Does not include opiate combinations. There was no use of chlorpromazine or IV aspirin in our cohort. bDoes not include opiate combinations. Other medications given without concurrent parenteral headache medications included (in frequency order): Other antiemetics (ondansetron and promethazine), benzodiazepines, and antihistamines. NOS: not otherwise specified; NSAIDs: nonsteroidal anti-inflammatory drugs; DHE: dihydroergotamine.
Of the 574 study participants, 140 (24.4%) were treated initially with an alternative parenteral medication (non-opiate and non-recommended first-line agent). The most common was ondansetron, which was given as the initial parenteral agent without concomitant analgesics in 72 (12.5%) of all primary headache patients, including 23 (16.7%) of those with migraine and 48 (11.4%) of those with headache NOS. Other common alternative first-line medications given without concomitant analgesics included promethazine in 33 (5.7%) and lorazepam in 10 (1.7%) of all primary headache participants.
Subject characteristics comparison by initial parenteral medication.

NOS: not otherwise specified; IQR: interquartile range (25th–75th percentile).
Neuroimaging
Neuroimaging (computed tomography (CT) head or magnetic resonance imaging (MRI) brain) was performed in a total of 266 of the 574 initial patient visits (46.3%). Individuals diagnosed with headache NOS were much more likely to receive neuroimaging compared with those diagnosed with migraine headache (53.7% vs. 23.7%, p < 0.001). Neuroimaging was significantly more likely to be performed in patients who were given parenteral opiates first compared with those given first-line recommended parenteral agents first (Table 3).
Pain scores
The average initial pain score was 5.5 out of 10 (median 6), and 235 (40.9%) of study participants had severe headaches (7–10 out of 10 on the numeric pain scale). Individuals given opiates initially had significantly higher initial pain scores but were not more likely to have a severe headache at presentation compared with patients given first-line recommended headache agents (Table 3). The average discharge pain score was 2.3 out of 10 (median 2) for included patients at their initial visit. On discharge, participants given opiates first had similar pain scores compared with those given first-line recommended headache agents, and had similar proportions that were pain free at discharge (Table 3).
Length of stay
Long length of stay associations.
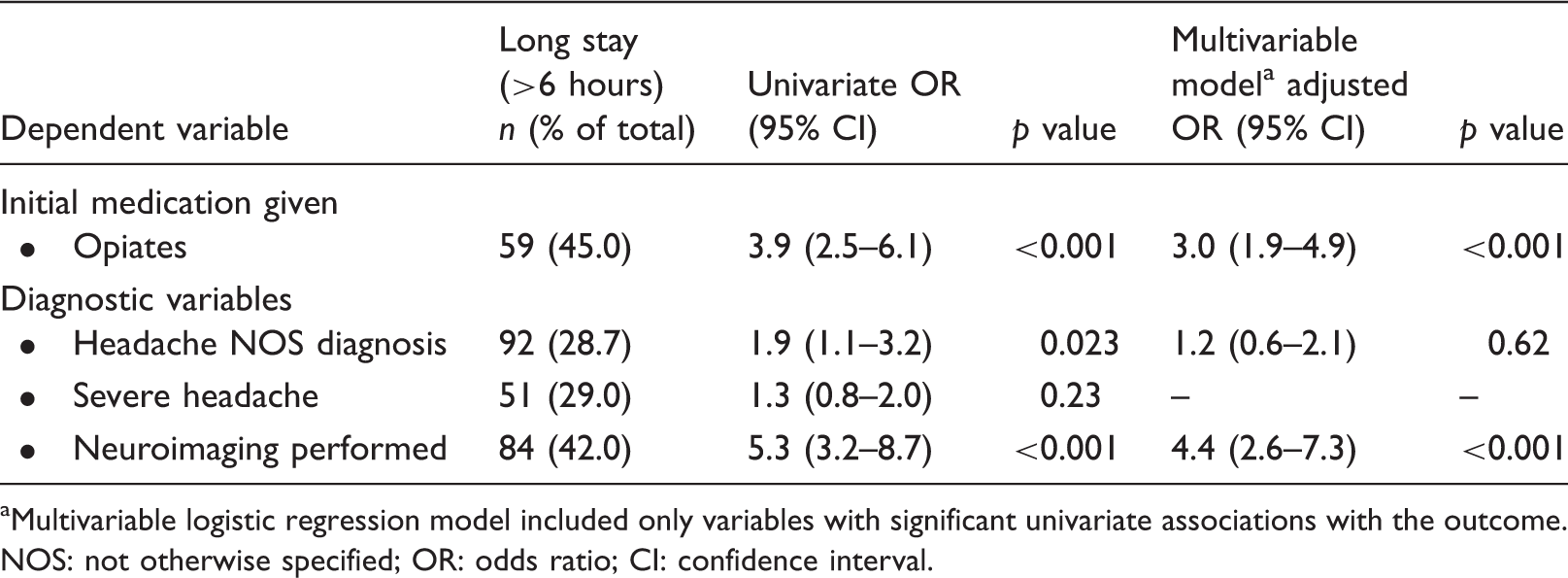
Multivariable logistic regression model included only variables with significant univariate associations with the outcome. NOS: not otherwise specified; OR: odds ratio; CI: confidence interval.
Those given opiates initially had univariate associations with significantly longer ED lengths of stay (Table 3) and were significantly more likely to have a long ED stay (Table 4). Subjects given opiates initially had a univariate 3.9 times higher odds of having a long stay compared with those given first-line recommended medications (odds ratio (OR) 3.9, 95% confidence interval (CI): 2.5–6.1, p < 0.001). This association with opiate use and longer lengths of stay remained strong and significant in the multivariable model after adjustment for possible confounders including headache diagnosis and neuroimaging performed (Table 4).
Return visits
Early return visits associations.

Multivariable logistic regression model included only variables with significant univariate associations with the outcome. NOS: not otherwise specified; OR: odds ratio; CI: confidence interval.
Those given opiates first were more likely to have early return visits than those given first-line recommended agents (7.6% vs. 3.0%, p = 0.033, Table 3). Patients given opiates first had a 2.7 times higher likelihood of an early return visit (OR 2.7, 95% CI: 1.1–6.8, p = 0.035) in univariate analysis. In multivariable analysis, the addition of the neuroimaging variable significantly attenuated the association with early return visits and opiate initial use and the association was no longer statistically significant (p = 0.15, see Table 5). The interaction term between opiates given first and neuroimaging performed was not statistically significant on inclusion into the model (p = 0.45).
Discussion
Primary headache patients presenting to an academic medical center ED are treated with a variety of medications and commonly with opiates. Our retrospective analysis suggests that the initial use of parenteral opiates for acute primary headaches is associated with an increased length of stay and increased rates of return visits and is consistent with prior reports that looked specifically at migraine headache treatment (24,25,32). Our analysis shows this association holds for not only migraine but for a large proportion of patients with acute primary headache who present to the ED with a diagnosis of headache NOS. Encouraging the initial use of first-line recommended headache medications rather than opiates in all acute primary headaches (regardless of migraine diagnosis), as encouraged in prior literature, could improve patient outcomes.
The association between longer length of stay with initial opiate use likely reflects, in part, a class effect as opiates have shown less headache pain reduction, higher rates of headache recurrence, and increased sedation compared with first-line recommended specific headache medications (9,33). Furthermore, the associations between length of stay and return visit rate with opiate use are modified by diagnostic uncertainty. As seen in our study, there were significantly higher rates of opiate use in patients with headache NOS diagnosis and those with neuroimaging performed. The diagnostic uncertainty as to whether the patient has a secondary headache disorder (e.g. subarachnoid hemorrhage) drives the decision to order neuroimaging and likely influences initial medication choices. This includes avoiding medications that can worsen intracranial bleeding such as NSAIDs and likely avoiding migraine-specific medications such as triptans or DHE. This diagnostic uncertainty then likely influences the final diagnosis coding, discharge prescriptions, and follow-up recommendations that, in turn, modify patient outcomes. Neuroimaging is a significant confounding factor in our analysis that attenuates the relationships between initial opiate use and patient outcomes, which likely represents their shared associations with diagnostic uncertainty.
Although migraine-specific serotonin receptor agonist medications (e.g. DHE or triptans) and dopaminergic antiemetics were used more frequently in individuals with migraine, they were likely far underutilized in our study population, which is, again, consistent across the literature of ED headache treatment. The high utilization of ondansetron in headache patients is concerning given its lack of evidence in treatment of headache or headache-related nausea compared with the dopaminergic antiemetics (e.g. prochloperazine or metoclopramide) and given a number of case reports that suggest ondansetron may initiate migraine headache (34).
Because our analysis is retrospective, we are limited in our ability to attribute cause and effect to the relationship of medication use and outcome. Given that the emergency physicians chose medical treatments at their own discretion, there could be a bias of treatment of certain patients (e.g. patients with known or self-described refractory headaches treated with opiates first line). Additionally, we did not analyze the patients’ list of adverse drug reactions or allergies, which may have biased treatment decisions and increased opiate use if they were allergic or intolerant to first-line recommended agents in the past. Furthermore, secondary headache or complicating comorbid diagnoses were more commonly seen in our study population than expected. This may reflect the fact that headache is a common complaint in patients with multiple other diagnosis (e.g. upper respiratory infection, trauma), and may be over-documented in our system as a chief complaint when there are other inciting events (e.g. fall, infection). Also, the diagnosis of migraine headache, compared with headache NOS, was less common in our study than in prior reports, which may be due to differences in our patient population, physician diagnostic and documentation practices, or billing and coding criteria.
Headache is a common reason for admission to the ED and while there are many recommendations on treatment of specific headache types (e.g. acute migraine), the use of medications for primary headache NOS in ED patients still varies widely. Opiates are commonly used despite multiple expert recommendations against their first-line use in treating acute primary headaches. Further study is needed to evaluate if changes to standard practice medical treatment of all types of acute primary headache disorders in the ED could improve patient outcomes, reduce costs of care, and improve ED efficiency.
Clinical implications
Acute primary headache is often diagnosed and treated as nonspecific headache in the emergency department (ED). Opiates are still commonly used for acute primary headache treatment and non-opiate first-line recommended headache medications are likely underutilized in the ED. Initial opiate use is associated with longer lengths of stay and higher rates of early return visits compared with non-opiate first-line recommended headache medications. Opiate use is highly associated with diagnostic uncertainty, including higher rates of neuroimaging utilization and nonspecific headache diagnosis, which modified the association with length of stay and early return visits.
Footnotes
Funding
This work was supported in part by a National Institutes of Health (NIH) Clinical and Translational Science Award (CTSA) number UL1 RR025744.
Conflict of interest
None declared.
Acknowledgment
The authors are grateful for the work of Gomathi Krishnan, PhD, in data extraction from the electronic medical record research database (STRIDE).