
Abstract
Background
Mathematical modeling approaches are becoming ever more established in clinical neuroscience. They provide insight that is key to understanding complex interactions of network phenomena, in general, and interactions within the migraine-generator network, in particular.
Purpose
In this study, two recent modeling studies on migraine are set in the context of premonitory symptoms that are easy to confuse for trigger factors. This causality confusion is explained, if migraine attacks are initiated by a transition caused by a tipping point.
Conclusion
We need to characterize the involved neuronal and autonomic subnetworks and their connections during all parts of the migraine cycle if we are ever to understand migraine. We predict that mathematical models have the potential to dismantle large and correlated fluctuations in such subnetworks as a dynamic network biomarker of migraine.
Introduction
Although migraine sufferers often are convinced that certain food, stress, bright light, neck pain, and other factors may trigger attacks, under controlled experimental conditions, there is very little if any evidence that these putative trigger factors can actually provoke attacks (1,2). Instead of being the trigger initiating an attack, craving certain food, perceiving normal events as stressful or normal light intensities as too bright, and experiencing neck pain in the few hours to days prior to the clinical manifestation of a migraine attack more likely are early premonitory symptoms of an attack. Premonitory symptoms are actually expected as early-warning signs of an imminent transition and they are easy to confuse for trigger factors, if migraine attacks are initiated by a transition caused by a tipping point and therefore exhibiting universal behavior (3) (see Figure 1). We addressed this question with mathematical migraine models in two recent articles (4,5).
Illustration of tipping point behavior: A changing landscape with potential wells and unique (violet landscape) or two (all other) stable attractors, representing the pain state (left) and attack-free state (right). The balls represent the current state and its variability (yellow dashed line) under constant influence of noise as putative trigger factors (hammer). In this schematic illustration, a gradual increase of excitability over time lowers the potential well and the local landscape of the current state becomes shallower. The curvature of the well is inversely proportional to the system-imminent time scale (τ) that determines the response to natural noise. The incipient loss of the threshold separating the attack-free minimum state from the attack state, that is, the prodromal phase, is indicated by both large amplitudes and critical slowing down (large τ) of the fluctuations of the ball. These large amplitudes and critical slowing down of fluctuations can lead to confusing this for trigger factors, when in fact even purely internal noise (absence of hammer) will cause these eventually. Figure modified from Lenton et al. (3) and Scheffer et al. (4).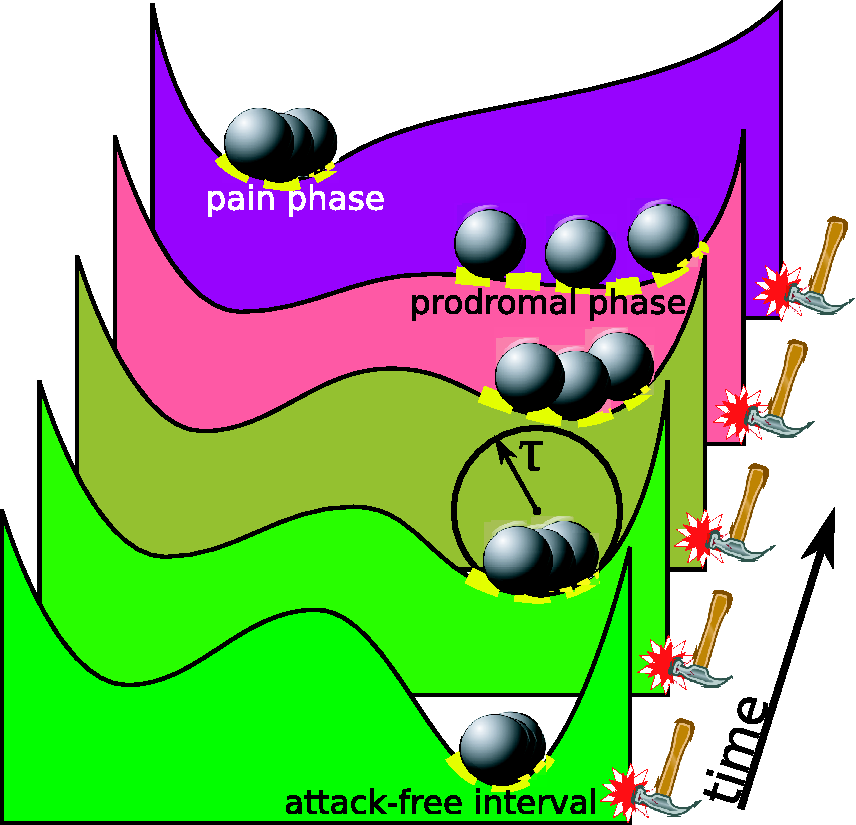
Universal tipping point behavior explains premonitory symptoms
The theoretical concept of tipping points, if transferred to migraine research, addresses the role of reduced resilience (4). As the brain comes to a tipping point, a small stimulus can trigger a slow cortical wave experienced as aura symptoms (6). The most important “cause” or “explanation” of migraine as a chronic disease with episodic manifestations is therefore the dynamic change in excitability bringing the brain to this tipping point, rather than the small perturbation that finally tipped the balance leading to the attack as such. Although perturbations can be reduced, for example using exercise, stress relaxation techniques or cognitive behavioral therapy, they cannot be excluded entirely near tipping points (Figure 1). When the state of the brain gets again farther away from the tipping point, i.e. in a remissions phase of the migraine cycle, even very large perturbations—as recently published (1)—will not be able to trigger episodes. This refractoriness of hyperexcitability to external stimuli in the postictal and interictal phase can also be predicted as a general feature of chronic disorders with episodes caused by recurrently passing through a tipping point.
The neural correlates of early-warning signs caused by tipping points can be described as dynamical network biomarkers (DNBs) (7). A DNB describes certain behavior in a subnetwork of a complex disease, namely signals that announce the reduced resilience at an imminent tipping point by large and correlated amplitudes and critical slowing down of fluctuations in this subnetwork. In Figure 1, this subnetwork is represented by the cross-section within a higher-dimensional landscape. Only in this particular cross-section the well is becoming shallower, while in all other directions perpendicular to this cross-section the well keeps its steep depth profile. DNBs have been found for lung injury disease, liver cancer, and lymphoma cancer (7,8). The theoretical concept and established methods of DNBs can be transferred from such sudden deterioration diseases to chronic disorders with paroxysmal episodic manifestations like migraine (5).
Tipping points as a transdisciplinary concept
Tipping points may be better known with respect to the earth climate system (3). However, tipping points can be found in medicine, financial markets, traffic, power grid systems to which a large amount of renewable energy is introduced and that therefore may fail, ecosystems where wildlife populations may be threatened, and in the global climate system (9)—not too surprising, as all these are complex systems that exhibit nonlinear behavior and therefore are very likely to show tipping points.
Although mere coincidence, there are metaphors about migraine and the brain’s climate, migraine being a thunderstorm or lightning in the head. It can be fruitful to see beyond such metaphors the consequences of tipping points and the related common structure of causal misinterpretation, both schematically illustrated in Figure 1. Consider the statement of Kleinen et al. (10) referring to the North Atlantic currents: “It is becoming increasingly evident that there are critical thresholds in the Earth system, where the climate may change dramatically ( … ). The exact positions of these thresholds are, however, still unclear and it might be doubted whether they can be determined with enough precision to give concrete information on the threat of crossing the threshold. Therefore, additional independent methods for assessing the closeness of the system to these thresholds are needed. These methods could contribute to an early warning system for assessing the danger of crossing a threshold and possibly provide the information necessary for controlling the system” (10). One arrives at a central question in migraine research that will profit from complex systems theory, when in this citation “Earth” is replaced with “brain” and “climate” with “neural dynamics” and when we start to use established concepts in climate research: How can we assess the proximity of a migraine threshold and, if the risk is large, control in this early stage the imminent migraine attack?
Climate change over decadal time scales probably involves changes in the ocean’s conveyor belt, the thermohaline circulation, which was modeled in Kleinen et al. (10). Dahlem et al. (5) proposed considering migraine pain caused by central sensitization in an analogy as an overturning circulation in nerve traffic of the brain’s migraine-generator network (MGN) (11). What are early warning signals of this overturning circulation? Again, let us consider the climate system in an analogy: It is easy to mistake cold winters for contradicting global warming, while in fact, severe winters like the ones of 2005–2006 and 2009 do not conflict with the global warming picture, but rather supplement it as an integral part of the large and correlated amplitude fluctuations (12).
Neural correlate of premonitory symptoms in a subnetwork
There are no simple answers to simple questions in nonlinear systems; in particular a causality interpretation is difficult. Reduced resilience and consequently large and slow fluctuations can explain the above-mentioned situations where events that belong to the natural variability are mistaken near tipping points for triggers even if this is not intuitive for the patients concerned. It was actually also suggested that migraine patients are driven or have the urge to exercise as a premonitory symptom (13). Unchallenged is that excessive yawning is a well-known prodromal symptom in migraine; the same holds true for rapid mood changes, fatigue and craving for certain foods to name but a few. However, active coping, such as biofeedback (14) including contingent negative variation (CNV) (15) but also behavioral treatments including relaxation training, stress-management training and cognitive-behavior therapy (16) clearly showed that the pre-transition state is in principle reversible, at least in some of the attacks. Where in the proposed subnetworks would such behavioral therapy take its effects? Brainstem activation is thought to be specific for migraine attacks, and specifically the dorsolateral pons has been repeatedly demonstrated by imaging data (17–19), while it also was suggested that this area alone cannot be the migraine generator (20). Given that the premonitory (21) and the subsequent attack symptoms (22) are characterized by interdependent networks, which explains many of the facets of each event, the possible interplay between these networks has been coined the MGN (11).
If a DNB can be found in migraine it will identify the neural correlate for multiple early-warning signs as a common subnetwork of the MGN. In fact, there is a unitary hypothesis that identifies such a subnetwork—but only for multiple triggers causing migraine pain and strain (23). Therefore, if indeed triggers and symptoms are often mistaken at the incipient tipping point, this unitary hypothesis would suggest that large and correlated fluctuations in this subnetwork are crucial, that is, given the clinical picture, in the limbic system as well as the pre- and postganglionic parasympathetic neurons that control the sympathetic/parasympathetic balance. We predict therefore large and correlated fluctuations in this subnetwork as a DNB of migraine (5).
Conclusion
To summarize, quantitative modeling approaches are becoming ever-more established as a transdisciplinary research field. At the same time, the clinical research audience faces the difficult task, if not to penetrate mathematical concepts, at least to take away the message relevant for their own research. The particular message for clinical research is that our prediction must be tested: We need to characterize these neuronal, i.e. cortical, subcortical and autonomic subnetworks and their connections in the prodromal phase and the cortical slow wave during the aura phase if we are ever to understand the true beginnings of an attack. The general message from complex systems theory is that migraine is an inherently dynamic disease (24) with a complex network generating interdependent events.
Clinical implications
This article highlights the use of mathematical models in migraine research. It explains causality confusion between triggers and premonitory symptoms by tipping points. This explanation makes specific predictions of large-scale correlated fluctuations that need to be tested by noninvasive imaging.
Footnotes
Funding
This work was supported by the Seventh Framework EU-project EuroHeadPain (#602633) to AM and MF and the FIRST program from JSPS, initiated by CSTP to KA.