
Abstract
Aim
This randomized, controlled trial examined the medium-term effectiveness of online behavioral training in migraine self-management (oBT; N = 195) versus waitlist control (WLC; N = 173) on attack frequency, indicators of self-management (primary outcomes), headache top intensity, use of rescue medications, quality of life and disability (secondary outcomes).
Methods
An online headache diary following the ICHD-II and questionnaires were completed at baseline (T0), post-training (T1) and six months later (T2). Missing data (T1: 24%; T2: 37%) were handled by multiple imputation. We established effect sizes (ES) and tested between-group differences over time with linear mixed modelling techniques based on the intention-to-treat principle.
Results
At T2, attack frequency had improved significantly in oBT (−23%, ES = 0.66) but also in WLC (−19%; ES = 0.52). Self-efficacy, internal and external control in migraine management – and triptan use – improved only in oBT, however. This indicates different processes in both groups and could signify (the start of) active self-management in oBT. Also, only oBT improved migraine-specific quality of life to a sizable extent.
Conclusions
oBT produced self-management gains but could not account for improved attack frequency, because WLC improved as well. The perspective that BT effects develop gradually, and that online delivery will boost BT outreach, justifies further research.
Keywords
Introduction
Migraine attacks of pounding headache impede work performance and family or social life (1) and are the seventh disabler worldwide according to the World Health Organization (WHO) Global Burden of Disease Survey 2010 (2). Early treatment of the pain is more effective than waiting until the attack is fully developed (3), and attack prevention and proactive migraine management are gaining increasing emphasis (3–5). Behavioral training (BT) pursues proactive management and is advocated in neurological guidelines as a supplementary preventive treatment (6). A first focus of BT is on anticipating attacks by the timely recognition of premonitory symptoms. Because the prodromal stage of the attack is badly demarcated, this task is neither plain nor easy. Electronic diaries pointed at the relevance of the last 12 hours before attack onset when distinct symptoms emerge (7) and attacks are predicted relatively well (8). This substantiates the aim that early symptom detection is possible and could be learned (3). A second focus of BT is on self-regulation skills through relaxation training and cognitive-behavioral intervention (9). BT is targeted at increasing perceived control over migraine, reducing attack frequency and intensity, and decreasing migraine-specific disability (9,10).
Clinic-based BT can reduce attack occurrence by 35%–55% (11), but this form of BT is scarcely available. To increase BT access and engage patients more in self-management, we involved trained patient trainers who offered BT at home (12–14). The lay trainers were well received (14), and BT yielded strong and stable improvements in migraine self-efficacy and perceived control (12,13). Yet, improved attack frequency post BT (−21%) did not reach significance (p = 0.07) compared to waitlist control (WLC) (−6%) (13), while we found significant attack improvement six months later (−23%; p < 0.000) in an uncontrolled study (13). Importantly, all outcomes were maintained for three years on average (15).
Since the Internet amplifies the promise of BT outreach (16), we converted the former BT protocol (12,13) to an Internet application delivered with minimal guidance, and we extended the effectiveness trial of online BT (oBT) versus WLC up to six months after post-treatment (e.g. 10 months after baseline). Most prior studies in oBT (17–23) were confined to post-training measurement (17–20,22) four of which yielded significant headache improvement (17,19,20,22) also compared to WLC (17,19) or active control (22). Unfortunately the comparison with two recent oBT studies with control over six months post-training is limited given differences in study group (youngsters aged 12 years on average) (21) and the exclusion of headache as an outcome variable (23).
The oBT post-training effects are reported elsewhere (24) and closely matched those of BT offered by patient trainers (12), but attack frequency improved in WLC as well (24). However, compared to WLC, oBT yielded positive change in self-efficacy and perceived control indicating improved self-management. Since BT has a longer time to benefits than drugs (25), this study aims to establish oBT effectiveness relative to WLC for six months post-treatment regarding the parameters employed in the study with patient trainers (12–15). The question is whether oBT improves attack frequency and migraine self-efficacy and locus of control (LOC) over time (primary outcomes) as well as migraine-specific quality of life and disability (secondary outcomes). Effects over time were also tested for headache top intensity and use of rescue medications (secondary outcomes). Among the explorative analyses we examined whether attack improvement while on the waitlist resulted from consuming other health care, or from using the online migraine monitor provided in this study (24).
Methods
Design
We conducted a randomized, controlled trial to establish oBT effectiveness relative to WLC up to 10 months after baseline (T0), with assessments post-training (T1) and six months later (T2). The average completion time of the study was 11.6 months in oBT (SD = 1.7) and 11.1 months in WLC (SD = 0.5).
Participants
Participants were recruited through referral of the Dutch Headache Centers (www.hoofdpijncentra.nl) (26%) and the website of the Dutch Society of Headache Patients (www.hoofdpijnpatienten.nl) (21%); the remaining participants enlisted mostly in response to flyers in general practitioner (GP) offices.
The inclusion criteria were (1) an age of 18 to 65 years, (2) migraine according to the International Classification of Headache Disorders, second edition (ICHD-II) criteria (International Classification of Diseases (ICD)-10 NA; migraine without (G43.0) or with (G43.1) aura) (26)), (3) two to six migraine attacks in the month prior to randomization. The exclusion criteria were (1) headache occurring on more than 15 days or (2) medication overuse (≥10 triptans, or analgesics on ≥15 days) in the month before randomization, (3) a score ≥178 on the Symptom Checklist (SCL)-90 R screening instrument for psychopathology, (4) migraine onset in the previous year, (5) current or planned pregnancy.
Procedure
The study was approved by the Medical Ethics Committee of the University Medical Centre Utrecht (no. 10-304). Eligibility was assessed in the study’s protected web-portal (www.mymigraine.nl) where questionnaires (ID Migraine™ SCL-90 R) were completed and a prospective headache diary designed according to trial guidelines (8,27) was kept.
Eligible participants signed for informed consent, completed the T0 measures and were assigned with equal probability to either the oBT or WLC condition (unrestricted randomization based on a computerized scheme) by a research assistant who was unaware of the next group allocation; blinding was not possible since the study concerned a psychological intervention (8). Non-eligible patients were advised of and received contact information of a nearby headache center if desired. Psychosocial help was suggested in case of problems indicated by the SCL-90 R. Although this was allowed, participants were kindly requested not to change their medication or start other treatments during the study.
Intervention
oBT aims at attack prevention. It incorporates training in relaxation and cognitive behavioral techniques attested with grade-A for non-pharmacological migraine prophylaxis (5) and includes 70% of established behavioral change techniques (BCTs) advocated for web-based interventions (28). (Important BCTs pertain to graded tasks, specific goal setting and review of behavioral goals; behavior self-monitoring with teaching the use of prompts and cues, feedback on performance and barrier identification; behavioral modeling and social comparison, a focus on time- or stress-management, and relapse prevention.) It was closely adopted from the manual formerly used by patient trainers (12–15), which in turn was grafted on a cognitive behavioral therapy protocol for headache (29). oBT consists of eight lessons offered with voiceover, four relaxation audios, 26 videos of exemplary patients, interactive exercises, homework, and email support (30). Each lesson pursues two steps under the catchwords “face your migraine” and “ease your migraine.” “Face your migraine” subsumes exercises to detect patterns of premonitory symptoms and triggers of the attack well before the headache strikes. “Ease your migraine” incorporates techniques for physical relaxation and cognitive-behavioral self-regulation (priority setting, time management, reshaping of involuntary thoughts and behavioral habits). Additional techniques focus on body posture and a healthy lifestyle and on handling the pain during an attack. Lesson 1 provides an introduction, health education, and explanation of the training goals. Lessons 2–4 aim at graded acquisition and practice of self-management skills, while lessons 5–7 focus on skill application in daily life. Lesson 8 summarizes the acquired skills, and contains the planning of skill maintenance and strategies for relapse prevention. Each lesson takes approximately one hour to complete, plus one to two hours for homework and daily relaxation exercises (30 minutes in the first and 10 minutes in the second half of oBT). Completion of assignments within and between lessons was obligatory in order to enter the next lesson (ascertained by a “selective release” function in the MyMigraine web-portal). Participants were advised to complete each lesson within seven to 10 days (12–15), but given the mean training completion time (3.6 months; SD = 1.4 (24)) this took two weeks on average. A trained postgraduate psychologist or master’s level psychology student under supervision of a clinical psychologist provided the email support, which consisted of weekly reminders, encouragement and tips (≤5 minutes) and of assistance, motivational support, and concluding comments upon completion of lessons 1–7 (10–15 minutes). Most participants (85%) preferred to be contacted biweekly or only when completing a lesson. The total time investment for support thus was 1.5 hours on average in most cases and two hours for 15% who preferred weekly contacts.
Measurements
The online headache diary was freely available, while daily entries were required for 30 days at T0, T1 and T2. Per day, headache occurrence could separately be indicated for the morning, afternoon, evening, and night, accompanied by intensity ratings on a visual analog scale (VAS, range 0.1–10.0). ICHD-II characteristics (26), and medication use for headache (yes/no), could be ticked off. Yes for medications opened a personal list established at baseline for the marking of agents used; administration quantities could be added but this was not mandatory. Text boxes allowed registering new drugs and premonitory features of the attack; women also logged their menstruation. Diary entries took a few minutes, and were visually available in an online migraine monitor (see online Supplementary Material, part 1). The monitor showed the course of headache in monthly graphs and distinguished the migraine attacks as classified according to the ICHD-II (26); symbols indicated the number of pharmacological agents used and the occurrence of menstruation in women; clicking a day permitted review, but not revision, of all diary answers. A diary entry could represent a day with or without headache; inclusion in the data analysis required ≥25 entries per measure point.
Attacks had to fulfill the ICHD-II criteria (26,31) of ≥2 migraine characteristics (unilateral location, pulsating quality, moderate or severe intensity, aggravation by physical activity) and ≥1 accompanying symptoms (nausea and/or vomiting; photo- and phonophobia). Attack frequency was counted, considering that recurrence within 48 hours from attack onset or within 24 hours after end of the attack covered one attack. For headache top intensity we counted the number of ratings with VAS pain intensity >7.0. Medications were classified as triptans, analgesics and prophylactic agents. Use of rescue medication was calculated separately for triptans and analgesics by counting the number of headache days each agent was taken (27).
Self-efficacy was assessed with the Dutch translation of the Headache Management Self-Efficacy questionnaire (HMSE) (32) consisting of 25 items with answers ranging from 1 (absolutely disagree) to 7 (absolutely agree). A higher score (range 25–175) indicates stronger confidence in one’s behavioral skills to prevent and manage recurrent headaches.
Perceived control over migraine was assessed with the Dutch translation of the Headache-Specific Locus of Control Scale (HSLC) (33) reflecting the expectation that the onset, course and severity of one’s migraine can be influenced by one’s own actions (11 items), fate/chance (11 items), or actions of medical professionals (11 items). Item responses range from 1 (strongly disagree) to 5 (strongly agree) and higher scores indicate more control. Because oBT was not designed to influence trust in health care, we included the subscales for internal (perceived self-control over migraine; range 11–55) and external LOC (the conviction that migraine is a matter of fate or chance; range 11–55).
Migraine-specific quality of life was measured with the Dutch version of the Migraine-Specific Quality of Life questionnaire (MSQOL) (34) consisting of 20 items with agreement scores ranging from 1 (very much) to 4 (not at all). A higher score reflects a better quality of life between attacks (range 20–80).
Migraine-related disability was assessed with the Dutch translation of the Migraine Disability Assessment Scale (MIDAS) (35). For the past three months the days lost – and those with 50% lost productivity – due to headache, are assessed separately for paid work and housework; for family, social and leisure activities the days lost to headache are assessed as well. The MIDAS score sums all missed days plus the days with less than 50% productivity at work or at home.
Health care use was assessed at T0 and T2 with the Trimbos and iMTA questionnaire for costs associated with psychiatric illness (TiC-P) (36). We used 10 items of part 1 for health care consumed in the preceding month regarding consultations with a GP or a neurologist, use of mental, paramedic or alternative health services, and hospital treatments or admissions.
Sample size
The sample size was grafted on migraine attack frequency. An effect size (ES) of 0.35 emerged for online interventions in headache (16) and was proposed as a benchmark for routine psychological treatments in chronic pain (37). A power of 0.80 in two-tailed testing with ES = 0.35 and α = 0.05 yielded N = 130 per group, and 370 participants were needed, accounting for 30% expected study attrition.
Statistical analyses
All analyses were based on the intention-to-treat principle (ITT). We used multiple imputation for handling missing data (38), employing a chain of conditional regression models (fully conditional specification (FCS) (39)). Computations were carried out separately per group by the package Mice (40) in R (41), with 50 iterations for the algorithm to converge and 100 multiply imputed datasets, specifying the model type for scale variables as predictive mean matching (PMM). The effectiveness outcomes of the 100 datasets were combined into one single estimate using Rubin’s rules (38). Cohen’s d (42) will indicate ES of the outcomes within (baseline to T2) and between the groups at T2 (negligible: d < 0.2, small: 0.2 ≤ d < 0.5, medium: 0.5 ≤ d < 0.8, large: d ≥ 0.8). Results are presented as the mean and standard deviations of the observed data; analyses are based on the imputed data with p = 0.05 as cut-off for statistical significance in two-tailed testing.
Between-group differences in the change trajectories per outcome measure were tested by a series of individual growth curve (IGC) models using linear mixed modelling (LMM) in SPSS with maximum likelihood (ML) expectation. The first step (unconditional model) established the intraclass correlation (ICC) representing the amount of variance due to differences between individuals. The next two steps determined the shape of the growth, with step 3 depending on significant results of time in step 2. Step 2 tested linear growth by including time as a predictor; in step 3 time2 was entered to examine quadratic growth and, if so, detect acceleration or deceleration over time. Step 4 included group and time*group interactions to examine the differential growth trajectories for oBT versus WLC. Initial models were tested with the covariance structure “variance compound.” All analyses were repeated with study completers only, and for log-transformed data to correct for skewedness in the measurements of analgesic use and migraine disability (sensitivity analyses). These results did not lead to different conclusions and are therefore not reported.
To explore reasons for attack reduction during the waitlist phase, improvement was compared between WLC participants who had used the migraine monitor frequently (≥80% of the days) versus those who had used it occasionally (≤20%) between T0 and T1 (mean 3.4 months; SD = 0.7). Also the WLC and oBT condition were compared regarding health care use prior to T2, and regarding extended medication use established by the headache diary at T1 and at T2. (We examined all changes in medications used for headache. Extended use entailed that a participant added a new medication category (triptans, analgesics or prophylactics) or replaced an analgesic purchased over the counter by an anesthetic that required medical prescription. Alterations of equivalent drugs within categories were ignored.)
Results
Patient flow through the study and participant characteristics
Figure 1 shows the flow through the study of 368 randomized participants (oBT: N = 195; WLC: N = 173) consistent with the Consolidated Standards of Reporting Trials (CONSORT) statement (43). Study attrition was 24% from T0 to T1 (oBT: 32%; WLC: 14%) and 37% from T0 to T2 (oBT: 43%; WLC: 29%). Among participants with known reasons for drop-out, loss of interest occurred less in oBT (16%) than in WLC (41%).
Participant flow through the study.
Baseline characteristics of the participants.
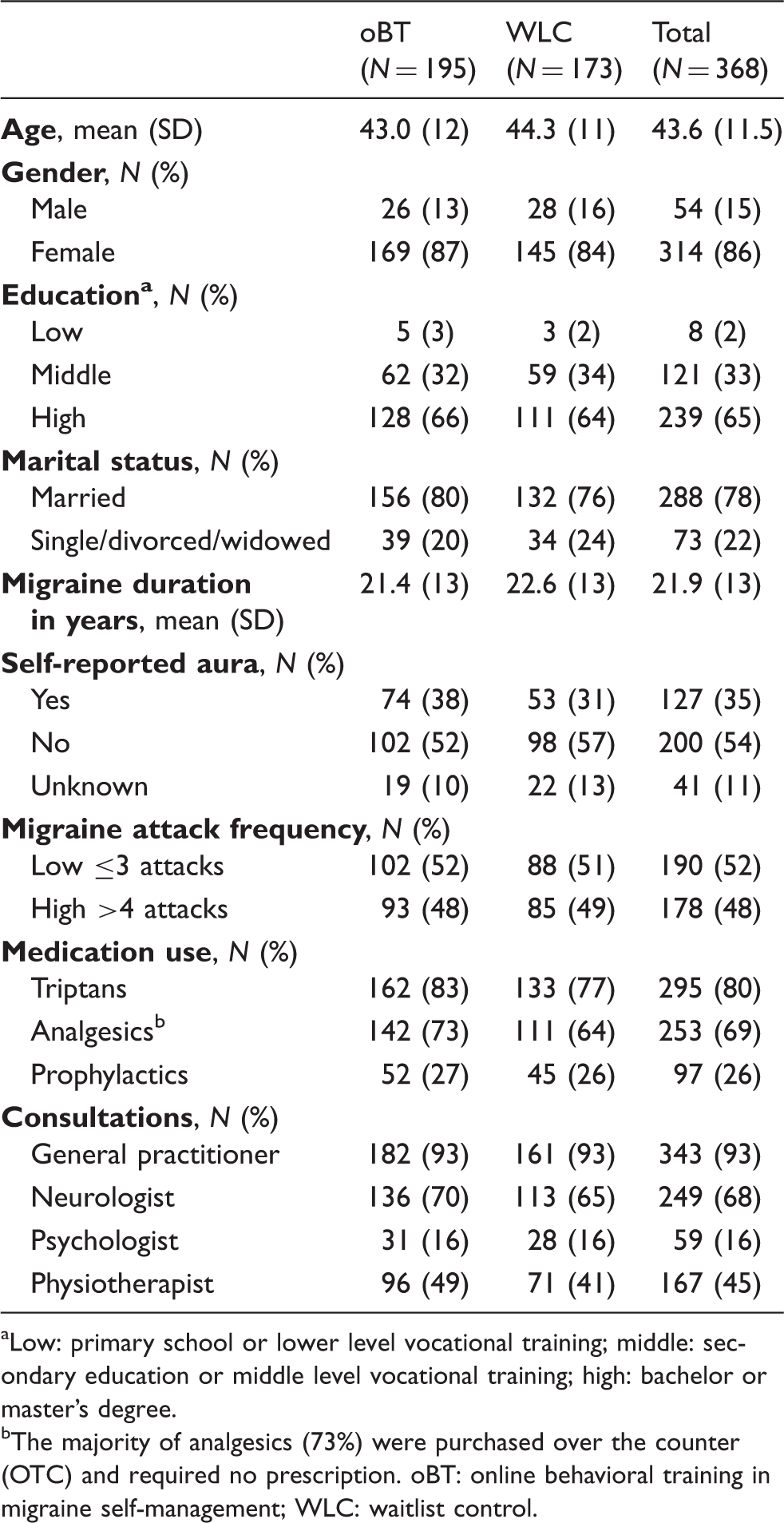
Low: primary school or lower level vocational training; middle: secondary education or middle level vocational training; high: bachelor or master’s degree. bThe majority of analgesics (73%) were purchased over the counter (OTC) and required no prescription. oBT: online behavioral training in migraine self-management; WLC: waitlist control.
Observed means (SD), effect sizes and results of the growth curve analysis for all outcome measures.

p < 0.05; bp < 0.01; cp < 0.001 (two-tailed testing). oBT: online behavioral training in migraine self-management; WLC: waitlist control; LOC: locus of control; CI: confidence interval.
Analyses of effectiveness
The results are organized by primary, secondary and exploratory outcomes. Table 2 presents the observed means at baseline (T0), post-treatment (T1), and six months later (T2), while testing was based on the imputed data (ITT). Figure 2 illustrates the change over time in all parameters (for all p values and models for individual growth see online Supplementary Material, part 2).
Change over time in all outcome measures.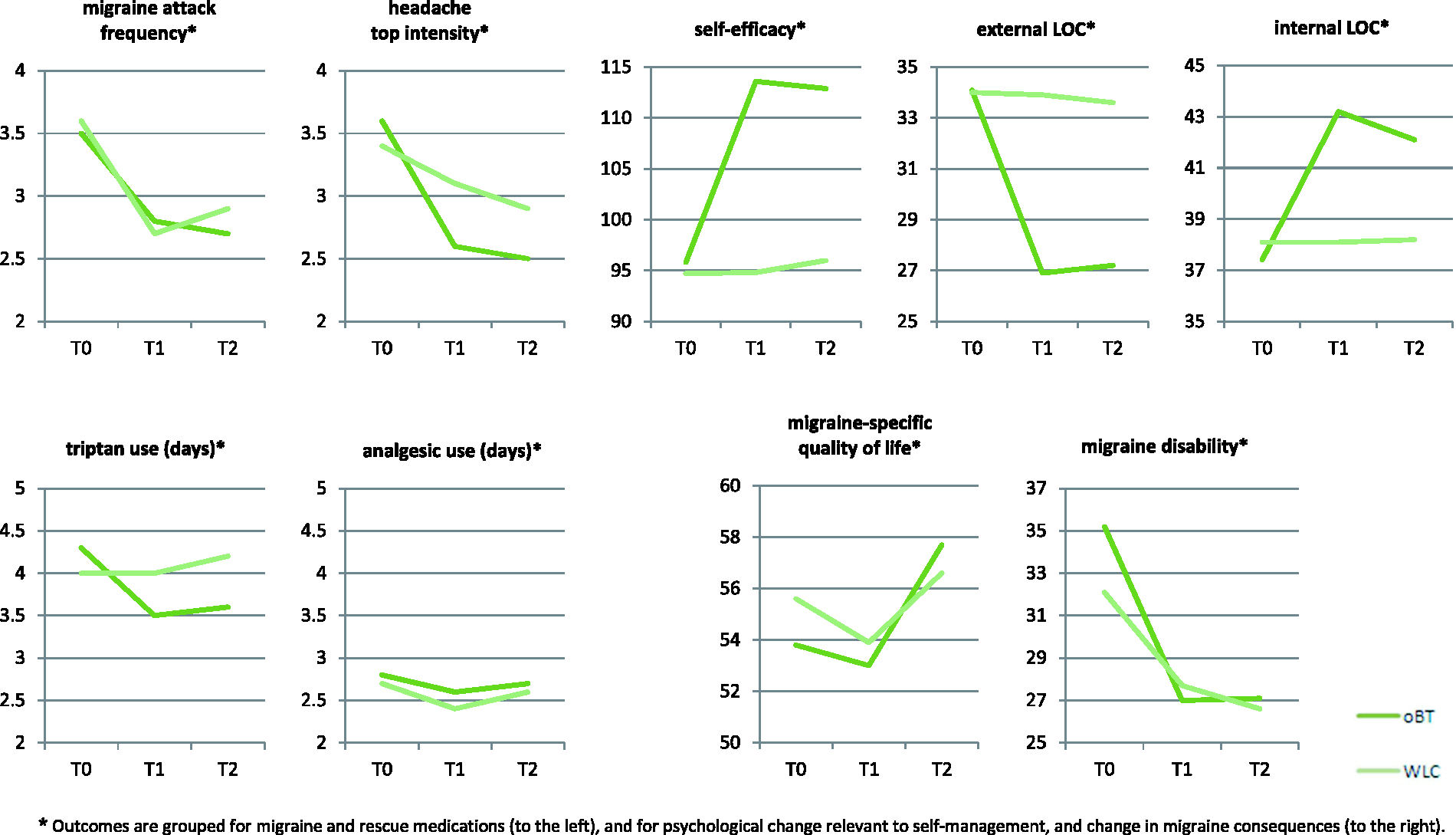
Outcomes are grouped for migraine and rescue medications (to the left), and for psychological change relevant to self-management, and change in migraine consequences (to the right).
oBT: online behavioral training in migraine self-management; WLC: waitlist control; LOC: locus of control.
Primary outcomes
Table 2 shows that migraine attack frequency decreased significantly over time in oBT (−23%; ES = 0.66, p < 0.001), but this occurred without significant difference also in WLC. The change trajectories in both groups yielded decreased attack frequency over time (time: b = −5.2, p < 0.001) with a steeper decrease between T0 and T1 (time2: b = 5.6, p < 0.001). Positive change over time in migraine self-efficacy and LOC, however, occurred only in oBT with small to medium ES (range 0.37−0.61, p < 0.001) and with similar values for the differences between conditions (range 0.43−0.61, p < 0.001). The growth analysis confirmed differential trajectories (Table 2, right columns) in favor of oBT, where self-efficacy and internal control increased and external control decreased from T0 to T1 and then remained stable.
Secondary outcomes
Over time headache top intensity improved significantly only in oBT (−31%; ES = 0.24, p = 0.032), but the growth analyses did not confirm a significant decline over time. Triptan use, however, decreased exclusively in oBT (−16%; ES = 0.54, p < 0.001), and the growth analysis substantiated the significant between-group effect (b = −1.6, p = 0.001). Use of analgesics (73% of which were mild anesthetics purchased without medical prescription) remained unchanged. Improved migraine-specific quality of life reached a sizable effect only in oBT (T2: ES = 0.47, p < 0.001) approaching between-group significance (p = 0.051) but uncorroborated by the growth analysis. Migraine disability improved in oBT (−23%; ES = 0.28, p = 0.009), but again without between-group significance.
Explorative analyses
Exclusion of participants who used prophylactic medications as recommended for behavioral research (8) did not affect any of the outcomes. A reduction ≥50% in attack frequency was adopted as clinically significant change or treatment responder rate, in accordance with other studies (12,17,19,20,22). Differences ranging from +49% to −49% were considered no change, and an increase of ≥50% was deemed an adverse response. Clinically significant change remained stable. At T2 oBT had 39% responders, 41% of the participants with no change, and 20% with an adverse response (for WLC this was, respectively, 33%, 46% and 21%). In the WLC condition attack improvement between frequent (N = 54) and occasional (N = 48) users of the migraine monitor did not differ over time (p ≥ 0.31), nor was there evidence that this group consumed more health care prior to T2 regarding medical consultations of a GP (WLC: 34%, oBT: 30%) or neurologist (WLC: 7%, oBT: 8%), use of mental health care (WLC: 16%, oBT: 14%), paramedic and alternative services (WLC: 54%, oBT: 53%), and hospital treatments or admissions (WLC: 1%, oBT: 2%). A small proportion of participants extended their headache medications during the trial: 4% in oBT (T1: 2%, T2: 2%) and 7% in WLC (T1: 5%, T2: 2%).
Discussion
This study showed that positive effects of oBT on migraine self-efficacy and perceived control were sustained over 10 months compared to WLC. However, the improved self-management did not translate to improved attack frequency since attacks decreased in both groups (oBT: –23%, ES = 0.66; WLC: −19%, ES = 0.52). Of the secondary outcomes, triptan use decreased significantly in oBT (−16%, ES = 0.54), while it increased in WLC (+5%, ES = 0.15). Other between-group differences were not significant, but it remains noteworthy that only oBT yielded a sizable improvement in migraine-specific quality of life (ES = 0.47).
Attack frequency declined while in WLCs triptan use increased to some extent, which could partly explain attack improvement in this group. In oBT, however, reduced attacks (−23%) and parts of days with incapacitating headache (−31%) went along with decreased triptan use. A different process thus seemed to have occurred in both conditions. The oBT group could have acquired self-management to some extent – given their achievement of migraine self-efficacy and perceived control – as a new tool to handle their migraine supplementary to rescue medications.
Additional reasons must also be explored, however, because the present attack improvement in WLCs vastly exceeded the 4%–6% in waitlist groups of former (o)BT studies (12,17,19,44,45), as well as placebo effects of 9%–10% in BT (44) or migraine rescue medications (46,47). Our participants could have admitted at a time of temporary migraine aggravation that decreased over time, but our trial seemed equally prone to this phenomenon as prior trials in (o)BT. The current WLC improvement also is beyond what could be expected from methodological artifacts such as random measurement errors (48,49), and help seeking behavior was compared but did not differ between conditions. Episodic migraine with ≤6 attacks per month has a relatively favorable prognosis over >10 years (50), however; natural history could thus have contributed but is unlikely to fully account for a remission of 19% of the attacks over 10 months’ time (46,50).
We excluded the explanation of high monitor use between the end of T0 and start of T1 when diary keeping was optional, but access to the migraine monitor may still have been a factor. The MyMigraine portal, migraine monitor and training were very well received (30); therefore reinforcement through this monitor may account for the limited study attrition in WLCs (T1: 14%; T2: 29%). But monitoring per se is not assumed to have induced self-management, because the WLC group gained neither self-efficacy nor a sense of control in migraine management.
Strengths and limitations
A predominant strength of this study is the extended follow-up with two post-training measure-points, which also applied to a previous controlled oBT study in adults during which effects on migraine were not assessed, however (23). Other strengths include the use of a prospective diary to sample migraine attacks according to the ICHD-II, and a training protocol rated by the participants as intelligible, instructive, important and not too difficult to accomplish (30). Last, we carefully selected a large sample of patients who had sought former medical advice (GP: 93%; neurologist: 68%), used valid medications for migraine, and only marginally extended this use during the trial (oBT: 4%; WLC: 7%). This indicates that our sample was medically informed and represented migraine patients under adequate treatment as usual.
High attrition typically hampers Internet-based trials (51), particularly in early studies including those for headache (16,17,19). In the present study failure to keep the online headache diary on ≥25 of 30 days per measure-point counted as study attrition. Notwithstanding this stringent criterion our attrition rates were not excessive (T1: 24%, T2: 37%), matching those of oBT trials in headache with an extended follow-up (T1: 24%, 14%; T2: 38%, 33%) (21,23) and 27% mean post-treatment attrition of web-based trials in chronic pain (52); also multiple imputation techniques counteracted the potential bias due to missing data. Second, we would have preferred number of administrations per headache drug as the measure for rescue medications, but this rating was not mandatory in our headache diary (this will be adapted). We compared results for the number of days a certain agent was taken (reported) with those for the number of administrations used. But given the incomplete data for administrations, our finding that these results were highly comparable must be interpreted with caution. Third, we chose to interfere as little as possible with the waitlist group and thus did not assess their treatment expectation or responses to our portal and tools, but such assessments would have helped to understand the attack improvement in WLC. Likewise, measurements of continued self-management and usage of strategies for relapse prevention were not performed in the oBT group. Both types of assessments should be conducted in future research.
Outlook on longer-term gains and future research
BT effects are known to develop gradually but to be durable (15,25,53). In this study the oBT effects on migraine tended to increase from T1 to T2, also relative to WLC (see Figure 2), and this trend could continue over time. Whether oBT induced additional attack improvement in the present WLC group will appear from the results—not as yet available—of oBT offered to WLC after T2, again with two follow-up measurements. The perspective on durable oBT gains is supported by the similarity in participant characteristics, training protocol, and training effects in the current and the previous study (see online Supplementary Material, part 3), effects of which were maintained for three years (15).
Our WLC assessment showed that longitudinal, prospective monitoring is feasible in migraine with limited attrition. This is important in its own right, because not much is known about fluctuations in migraine attack frequency over time. Future research should comprise such prospective assessments, in order to disseminate the impact of natural course, medication change, and behavioral or contextual factors on migraine attack occurrence.
Last, efforts to decrease attrition rates are of utmost importance. One oBT study in headache (22) stood out with lower rates (of 12% and 20% according to our calculation) at, respectively, three and six months after the start of training. The authors underscored two important reasons: (1) a compulsory headache diary that allowed a new entry only when data for the previous day were available, and (2) thorough face-to-face contact with all participants at the time of inclusion. The effect of both of these arrangements should be clarified in future research.
Conclusions
This study could not corroborate that the improvement in migraine attack frequency over 10 months’ time was due to oBT, as the WLC group progressed too. However, only oBT had sustained effects on migraine self-efficacy and perceived control, which indicate better migraine self-management. Whether oBT adds to the prevention of migraine attacks still has to be established. This deserves further study because BT has fewer side effects compared to medications (25), and because the online provision of BT can increase BT outreach as well as improve its cost-effectiveness.
Clinical implications
Behavioral training (BT), based on techniques of cognitive-behavioral therapy including relaxation training, can contribute to attack prevention in migraine. Online provision of this training (oBT) can increase BT outreach and improve the cost-effectiveness of BT. This study showed that attack improvement after oBT was not superior to waitlist controls of patients under treatment as usual who were followed with an online diary with visual feedback. However, significant indications of improved self-management and decreased triptan use occurred only when oBT was offered. BT outreach can be improved via patient trainers, the Internet, and – potentially – a combination of both settings.
Footnotes
Funding
This study was supported by grant # 1871 of the Health Insurers Innovation Foundation (Innovatiefonds Zorgverzekeraars) and by substantial support from the Utrecht University Faculty of Social and Behavioural Sciences.
Conflict of interest
None declared.
Acknowledgments
We thank the Dutch Society of Headache Patients and the Society of Dutch Headache Centers for their cooperation, in particular the neurologists E.G