
Abstract
Aim
This study examined the change over 20 months in 178 participants with frequent episodic migraine under adequate treatment as usual, who had completed online behavioural training (oBT) in migraine self-management either directly (group 1, n = 120) or after 10 months of watchful waiting (group 2, n = 58).
Methods
Participants completed questionnaires and an online headache diary and migraine monitor following the International Classification of Headache Disorders at T0 (baseline), T1 (post-training), T2 (6-month follow-up; extended baseline in group 2), T3 (post-training, group 2 only) and T4 (group 1: 16-month follow-up; group 2: 6-month follow-up). Statistical analyses were conducted on the observed data without imputation of missing observations.
Results
Both groups were highly comparable. The data over time revealed benefits in response to oBT, with significant between-group differences in the change achieved in the training episodes T2–T0 (group 1) and T4–T2 (group 2). Improved attack frequency (M = –23%) was higher in participants with more (i.e. 4–6) attacks per month at baseline, and the effects of oBT were durable over 16 months of follow-up.
Conclusions
oBT is beneficial in frequent episodic migraine, which deserves special efforts in care. Self-management variants such as oBT reach patients easily and supplement these efforts with durable results.
Keywords
Introduction
In Europe, migraine is the most costly neurological disease (1), accounting for 64% of all headache-related expenses (2,3). Migraine impedes work performance and impairs family and social life due to attacks of pounding and debilitating headache (4). Abortive pharmacological treatment is well established (5,6), but preventative treatment is relatively confined (7). Behavioural training (BT), advocated for by neurological guidelines as a supplementary preventative treatment (8), has a longer time to benefit, but fewer side effects than drugs, and its effects seem to be more durable due to improved self-efficacy (9). BT aims at proactive migraine management, which requires the recognition of premonitory symptoms of attacks in progression. The notion that this could be trained (10) gained support from electronic diary studies showing that, within 12 hours of migraine headache onset, premonitory deviations from interictal functioning are distinctly evident (11) and attacks are predicted relatively well (12). BT includes strategies for the identification of premonitory warnings and the acquisition of self-regulation skills through relaxation training and cognitive–behavioural intervention (13), and it can reduce attack occurrence by 35–55% when delivered individually in a clinical setting (13,14). This type of service is scarcely available, however. Since BT outreach could be beneficial through its extension to the open population with home-based applications (15) while promoting patient self-management (16), we tested its benefit when offered at home by trained patient trainers (17,18) or via the Internet (19,20). Both studies yielded strong psychological changes that are central to self-management and there was a 23% improvement in attack frequency six months after the end of the training, but the latter approach was uncontrolled (18) or not significantly superior to waitlist control (WLC) (20). However, the durability of effects over an average of 3 years was recently shown for home-based BT delivered by patient trainers (21).
The study in online BT (oBT) was extended for over 20 months. In the first 10 months, a randomised controlled trial (RCT) was conducted in oBT and WLC groups, with measurements taken post-training (T1) and at the 6-month follow-up (T2) (19,20); in the next 10 months, delayed training (oBT-d) was offered to the WLC group and also followed by measurements post-training (T3) and 6 months later (T4). At T4, the former oBT condition was assessed again, which yielded a 16-month follow-up for this group. This allowed us to examine changes over time in both groups and to follow oBT benefits up for 6 months in the training completers. Consistent with the RCT, we distinguish between primary (attack frequency and indicators of self-management) and secondary outcomes (headache top intensity, use of rescue medications, migraine-specific quality of life and disability).
The present paper focuses on the following research issues: (1) determine the change over 20 months in oBT completers who underwent training subsequent to randomisation (n = 120) or did so 10 months later (n = 58); and (2) establish the effects of oBT post-training and 6 months later in these treated cases. Explorative analyses concern the clarification of: (3a) treatment responder rates for clinically significant changes in attack frequency (17–20); (3b) potential differences in outcome between participants with high versus low attack frequencies at baseline (18); and (3c) potential moderators of the effects of oBT on migraine attack frequency at the 6-month follow-up (18). For the latter purpose, baseline characteristics, as well as satisfaction with and benefits of oBT as assessed post-training, were employed as effect predictors.
Methods
Design
Details of the RCT of oBT and WLC are described elsewhere (19,20). The concluding measure point of this trial (T2) served as the pre-training assessment for oBT-d, directly followed by oBT offered to the former WLC group with measurements post-training (T3) and 6 months later (T4). The original oBT group was assessed again at T4. On average, the study extended over 20.3 months in oBT (SD = 0.4) and 20.2 months in WLC/oBT-d (SD = 1.3).
Participants
Participants were recruited through Dutch Headache Centers (26%) and the Dutch Society of Headache Patients (21%) or enlisted mostly in response to flyers in general practitioner (GP) offices. The inclusion criteria were: (1) being aged 18–65 years; (2) meeting the criteria for migraine with or without aura of the International Classification of Headache Disorders, second edition (ICHD-II) (22); and (3) an attack frequency of two to six attacks in the 30 days prior to randomisation. Exclusion criteria were: (1) headache occurring on more than 15 days in the 30 days before randomisation; (2) medication overuse (≥10 triptans – or analgesics on ≥15 days – in the 30 days before randomisation); (3) a score of 178 or higher on the Symptom Checklist (SCL-90R) screening instrument for psychopathology; (4) experiencing migraine symptoms for less than 1 year; and (5) current or planned pregnancy. WLC participants not meeting the inclusion criteria at T2 were excluded from the analyses (see Figure 1).
Participant flow through the study over 20 months.
Procedure
A prospective headache diary that was designed to conform to the trial guidelines (23,24) and the Identification of Migraine screener (ID migraine), SCL-90R, and a demographic and health inventory were filled out in the study’s protected web portal (www.mymigraine.nl) for the purposes of eligibility. According to the inventory, almost all participants had sought medical advice (GP: 93%; neurologist: 63%) (19,20) and used rescue medications (triptans: 80%; analgesics 69%) for their migraine (20). A recent physical examination was not obligatory. When our assessments pointed towards complications or the need for medical action, the patients at issue were informed that this hampered inclusion and were advised to consult their physician or received contact information of a nearby headache centre if desired. Unrestricted randomisation based on a computerised scheme assigned eligible participants to either the oBT or WLC condition. Participants were asked not to change their medication while in the trial, and although this was not mandatory, participants complied to a large extent and only marginally extended their medication use for migraine in the first 10 months of the study (20). The Medical Ethics Committee of the University Medical Centre Utrecht approved the study (no. 10-304) and entrusted a medical board with the independent handling of any complaints, inconveniences or complications as stated by participants, but no such issues arose during the trial.
Intervention
oBT incorporates training in relaxation and cognitive–behavioural techniques that are ranked as gradeA for non-pharmacological migraine prophylaxis (25). It was closely adopted from the manual for patient trainers (17,18) and includes 70% of the established behavioural change techniques that are advocated for use in web-based interventions (26). oBT consists of eight lessons with homework offered, including audio files, videos, interactive exercises and email support (27). Each lesson pursues two steps under the catchphrases ‘face your migraine’ (focused on the early detection of prodromal signs well before start of the headache phase of the migraine attack) and ‘ease your migraine’ (subsuming techniques for physical relaxation and cognitive–behavioural self-regulation, including advice regarding body posture, a healthy lifestyle and pain management during an attack). Completion of assignments was obligatory in order to enter the next lesson. On average, the support took 1.5 hours for most participants, and 2 hours for the 15% who preferred weekly contacts; it comprised weekly reminders, encouragement and tips (≤5 minutes) or assistance, motivational support and concluding comments upon completion of the lessons (10–15 minutes). On average, the training took 3.6 months (SD = 1.4) to be completed (19).
Measurements
Measurements were taken per measure point at T0 to T4 (in the original oBT group, T3 was omitted). Migraine was assessed prospectively with the online headache diagnostic diary for 30 days. Migraine attacks were defined according to the ICHD-II (22,28) as follows: the headache had at least: (1) two migraine characteristics (unilateral location, pulsating quality, moderate or severe pain intensity and aggravation by physical activity); and (2) one associated symptom (nausea and vomiting as well as photo- and phono-phobia). Attack frequency was counted, considering that recurrence within 48 hours of attack onset or within 24 hours of the end of an attack represented a single attack. For headache top intensity, we counted the number of ratings >7.0 of the visual analogue scale (range: 0.0 to 10.0) for pain intensity. Medications were classified as triptans, analgesics and prophylactic agents. Use of rescue medication was calculated separately for triptans and analgesics by counting the number of headache days on which each agent was taken (29).
Other aspects were measured with four well-established questionnaires. We used the same Dutch versions throughout our research and refer to previous publications for the psychometric properties (17–20). Confidence in one’s behavioural skills for preventing and managing recurrent headaches (self-efficacy) and whether one views these headaches as being a matter of faith or under one’s own influence (perceived control) are regarded as important indicators of migraine self-management (30). Self-efficacy was assessed with the Dutch translation of the Headache Management Self-Efficacy questionnaire (31). Answers to the 25 items range from 1 (absolutely disagree) to 7 (absolutely agree). A higher score (range: 25–175) indicates stronger confidence in one’s behavioural skills for preventing and managing recurrent headaches. Perceived control over migraine was assessed with the Dutch translation of the Headache-Specific Locus of Control Scale (32), containing 22 items on a five-point scale (range: ‘strongly disagree’ to ‘strongly agree’) and reflecting the belief that the onset, course and severity of one’s migraine can be influenced by one’s own actions (internal locus of control; range: 11–55) or is due to fate/chance (external locus of control; range: 11–55). Higher scores indicate more control.
The secondary outcomes included two burdening consequences of living with migraine. Migraine-specific quality of life was measured with the Dutch version of the Migraine-Specific Quality of Life Questionnaire (33), consisting of 20 items with agreement scores ranging from 1 (‘very much’) to 4 (‘not at all’). A higher score reflects a better quality of life between attacks (range: 20–80). Migraine-related disability was assessed with the Dutch translation of the Migraine Disability Assessment Scale (34). For the past 3 months, the days lost – and those with ≥50% lost productivity – due to headache are assessed separately for paid work and housework, and for family, social and leisure activities. The days lost to headache are assessed as well. The score sums all of the missed days plus the days with less than 50% productivity at work or at home.
Satisfaction with and benefits of oBT were assessed post-training with 38 items of an online evaluative questionnaire, with answers ranging from 1 (‘not at all’) to 5 (‘very much’). These items were clustered, based on the agreement between two judges, into one scale for satisfaction with oBT and five scales for oBT benefits (see Online Supplementary Material 1). For the latter, ‘mastery of migraine self-management’ (with two scales for, respectively, ‘detection of prodromal signs (face your migraine)’ and ‘management of upcoming attacks (ease your migraine)’) was distinguished from ‘acquisition of self-management skills’ (with three scales for, respectively, ‘relaxation skills’, ‘cognitive skills’ and ‘self-care skills’).
Data analysis
All analyses were performed with SPSS version 20.0 (IBM Statistics) on the observed data without imputation of missing observations, since this study concerns the completers of the oBT training. We compared the outcomes of training completers to the data from all subjects allocated to oBT or oBT-d (see the results for research issue 2) in order to control for the impact of treatment drop-out or study attrition on the present results. The criterion for attrition was very stringent: failure to keep the online headache diary on ≥25 of 30 days per measure point (19,20). A significance level of p < 0.05 (two-tailed) was used throughout the study.
Improvement in outcome variables was tested using paired-sample t-tests within the oBT and oBT-d groups; the strength of the time effects was established per post-training measure point with Cohen’s d ((Mpre – Mpost)/SDpooled), providing an effect size (ES) that was negligible (d < 0.2), small (0.2 ≤ d < 0.5), medium (0.5 ≤ d < 0.8) or large (d ≥ 0.8) (35). Since the magnitude of improvement was presented in terms of ESs, it was considered reasonable not to adjust the significance values (p) of the within-group t-tests for multiplicity in order to avoid type II errors that leave effects undetected (36). In concordance with other studies (17,18,37–39), the treatment responder rate was defined as a reduction of ≥50% in migraine attack frequency; differences ranging between +49% and –49% were considered to represent no change, and an increase of ≥50% was deemed to be an adverse response.
In accordance with our study in BT (18), we used stepwise linear regression analyses to identify moderators of the oBT effect at the 6-month follow-up on attack frequency (dependent measure), with backward elimination and increased adjusted R2 as criterion for eliminating variables. The analyses were adjusted for gender, education, age and attack frequency at baseline. The first step included the baseline values of the remaining outcome variables (for the oBT-d group, scores at T2 were used). In the second step, we entered the summed scores per scale for satisfaction with oBT and the five benefits of oBT as rated post-training.
Results
Patient flow through the study and participant characteristics
Figure 1 shows the flow of participants through the study consistent with the Consolidated Standards of Reporting Trials statement (40), covering the measure points T0 to T4 over 20 months for research issue 1. For research issues 2 and 3, however, the indicators ‘pre’, ‘post’ and ‘6-month follow-up’ were added (see Online Supplementary Material 2, with details on study attrition per measure point). Of the 877 patients who were assessed for eligibility, 32% did not meet the inclusion criteria and 26% declined. The previous oBT and WLC groups were randomised successfully; loss of interest up to T2 was lower in oBT (16%) than in WLC (41%), while the reverse was true for study attrition (WLC 29%; oBT 43%), and both groups adhered strongly to the online headache diary (19,20). At T2, 29% (n = 51) of the former WLC participants declined oBT-d, while 16% (n = 27) no longer met the inclusion criteria, mostly (89%) due to decreased attack frequency (their training results were excluded). Analysis in all 178 oBT completers confirmed high adherence to the relaxation exercises (19), but the oBT effects did not differ significantly in the extreme groups of those who practiced relaxation on ≥80% of the training days (n = 42) versus those who did so on ≤20% of the training days (n = 27).
Comparison of characteristics of participants who completed oBT or oBT-d and those allocated to oBT or oBT-d.

Low = primary school or lower-level vocational training; middle = secondary education or middle-level vocational training; high = Bachelor or Master’s degree.
oBT: online behavioural training; oBT-d: delayed online behavioural training.
Research issue 1: change over 20 months in oBT completers who underwent training directly or did so 10 months later
Effects over 20 months in participants who completed oBT or oBT-d.

p < 0.05; ** p < 0.01; *** p < 0.001 (two-tailed testing).
Numbers vary somewhat per measure: n = 120 (T0), n = 99–118 (T1), n = 98–111 (T2), N/A (T3), n = 60–83 (T4).
Numbers vary somewhat per measure: n = 58 (T0), n = 55–58 (T1), n = 58 (T2), n = 54–58 (T3), n = 45–56 (T4).
Effect sizes were computed in both groups taking T0 into account as the baseline. This reflects the significance of change over the course of 20 months.
Effect sizes computed only for oBT-d using T2 instead of T0 as the pre-training baseline.
LOC: locus of control; oBT: online behavioural training; oBT-d: delayed online behavioural training.

Effects over 20 months in participants who completed oBT or oBT-d.
According to Table 2, both groups achieved highly comparable training results (oBT: T2 vs. T0; oBT-d: T4 vs. T2), and Figure 2 illustrates that benefits ensued due to the training. Distinct training effects occurred in self-management (self-efficacy and perceived control over migraine) and triptan use, and benefits were also noted regarding improved attack frequency and headache top intensity. The negative impact of migraine on quality of life and disability was ameliorated, but these improvements took more time to materialise. Between-group differences in change scores for migraine attack frequency verified the differential effect of oBT for the primary outcome. The oBT group achieved more (p = 0.03) positive change in migraine frequency at T2 versus T0 (Mchange score = –0.80 (SD = 1.8), p < 0.001 against Mchange score = –0.16 (SD = 1.7), p = NS in oBT-d), while at T4 versus T2, the change was in favour (p = 0.04) of the oBT-d group (Mchange score = –0.69 (SD = 1.8), p < 0.001 against Mchange score = –0.03 (SD = 1.7), p = NS in oBT). Attack frequency did not change significantly, however, while the oBT-d group waited (T2–T0, Mchange score = –0.16), and it remained improved in oBT during the 10-month prolonged follow-up (T4–T2, Mchange score = –0.03).
In these 10 months of extended follow-up, the oBT effects in 120 participants did not relapse, but rather strengthened somewhat instead. Noteworthy are the improvements in the burden of migraine, which reached medium ESs for migraine-specific disability (ES = 0.57) and quality of life (ES = 0.59).
Research issue 2: oBT effects post-training and at 6-month follow-up in all treated cases
Effects post training and at 6-month follow-up relative to pre-training baseline: comparison of participants who completed oBT or oBT-d and those allocated to oBT or oBT-d.

p < 0.05; ** p < 0.01; *** p < 0.001 (two-tailed testing).
Numbers vary somewhat per measure: N = 178 (pre), N = 167–178 (post), N = 162–170 (6-month follow-up).
Numbers vary somewhat per measure: N = 290 (pre), N = 183–207 (post), N = 165–172 (6-month follow-up).
LOC: locus of control; oBT: online behavioural training; oBT-d: delayed online behavioural training.
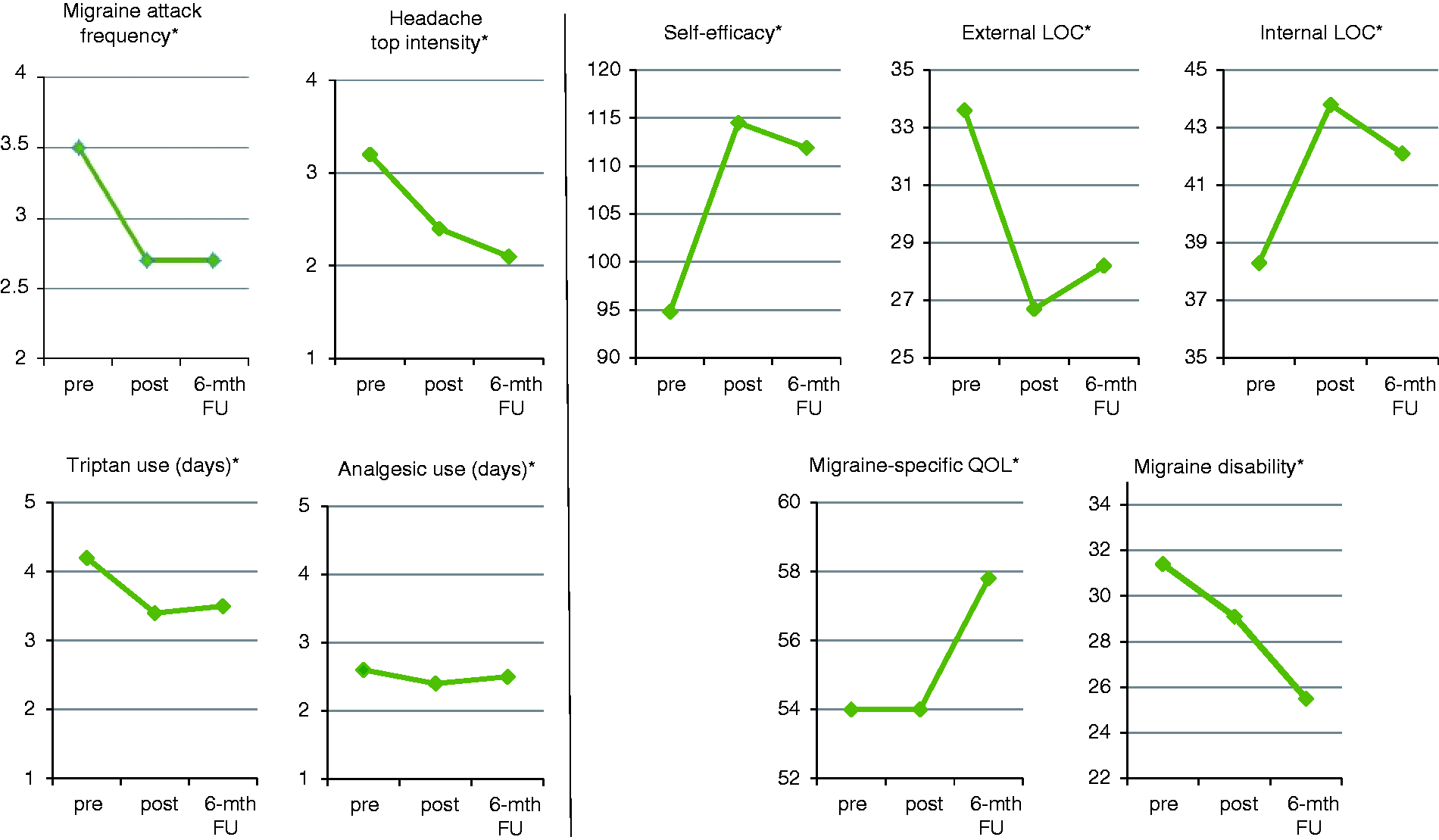
Effects post training and at 6-month follow-up in participants who completed oBT or oBT-d.
The results in treatment completers confirmed the strong oBT effects on self-efficacy and locus of control, indicating improved self-management. Migraine attack frequency decreased consistently (–23% at both measure points, p < 0.001), as did triptan use (post: –19%, 6-month follow-up: –17%, p < 0.001). Headache top intensity improved more strongly over time (post: –25%, 6-month follow-up: –34%, p < 0.001) independent of analgesic use, which did not change. Relief in the burden of migraine did not convincingly emerge post-training, but at the 6-month follow-up, migraine-specific quality of life had improved significantly (p < 0.001), as had migraine disability (–18%, p < 0.01).
Research issue 3: explorative analyses
The analyses pertain to: (a) responder rates in oBT completers; (b) differences post-training and 6 months later in participants with high versus low attack frequencies at baseline; and (c) potential moderators of the oBT effect on attack frequency at the 6-month follow-up.
Research issue 3a
Post-training, 36% of the oBT completers had improved to a clinically significant extent, 53% did not change and 11% responded adversely; at the 6-month follow-up, the rates were, respectively, 28, 58 and 14% (for a comparison with former findings, see Online Supplementary Material 3).
Research issue 3b
Attack improvements in participants with four to six attacks at baseline (high-frequency group, n = 99) were at rates of 28% post-training (ES = 0.91, p < 0.001) and 33% at 6 months later (ES = 1.21, p < 0.001), while those with fewer attacks (low-frequency group, n = 79) improved by 12% (ES = 0.24, p < 0.07) and 4% (ES = 0.08, p = NS), respectively, with highly significant between-group differences (p = 0.000) in averaged change scores.
Research issue 3c
The linear regression analyses showed that external locus of control (β = –0.14, p = 0.048), triptan use (β = 0.17, p = 0.021), migraine-specific quality of life (β = –0.27, p = 0.000) at baseline and ‘mastery of migraine self-management regarding upcoming attacks’ achieved during training (β = –0.20, p = 0.014) significantly predicted attack frequency at the 6-month follow-up. Attack frequency improved more strongly the more the participants at baseline had used fewer triptans, the more they tended towards external control and the more they exhibited a better migraine-specific quality of life. Through oBT, they had gained more mastery of successfully managing their upcoming attacks.
This model explained 48% of the variance in outcome; the four predictors were largely independent, except that better mastery gained through oBT was weakly associated with higher external control (r = –0.19, p < 0.05) and less triptan use (r = –0.17, p < 0.05) at baseline.
Discussion
To increase the outreach of BT and engage migraine patients to an optimal extent, we adapted an acknowledged protocol for psychological treatment to a self-management format offered by patient trainers (BT) (17,18,21) or online (oBT) (19,20,27). This paper extends a RCT over 10 months in oBT (19,20) with another 10 months, starting with delayed training offered to the former WLC group (oBT-d) and concluding with measurements 6 months later in all training completers. The data over time indicated that changes occurred not at random, but in response to the training; this was confirmed by significant between-group differences observed differentially in episodes T2–T0 (for oBT) and T4–T2 (for oBT-d). Both groups were highly comparable at the pre-, post- and 6-month follow-up, and the results of all treatment completers equalled those of the RCT (19,20). The effects of BT are known to develop gradually, but durably (9,21,41), and the present results confirm that the benefits of oBT were stable and did not deteriorate over 16 months of follow-up.
The results of oBT are strikingly consistent with those of BT offered face to face. Attack frequency, the primary outcome measure, uniformly decreased –23% with medium ESs and a steady responder rate (M = 40%) (17–21). This improvement was stronger, particularly at the 6-month follow-up, in participants with four to six versus those with fewer attacks per month at baseline (oBT: –33%; BT: –37%) (18). Both modes of training yielded immediate, strong effects on indicators of self-management (confidence in one’s behavioural skills for preventing and managing attacks and perceived control over migraine). In addition, reduced attack occurrence at the 6-month follow-up was predicted by the belief at baseline that the onset, course and severity of one’s migraine are due to fate or chance (external control) in oBT and BT (18); in oBT, additional predictors were less triptan use and higher migraine-specific quality of life at baseline, as well as mastery achieved during training in the self-management of upcoming attacks. Importantly, triptan use decreased significantly with both training modes (18,20), and in oBT, this change was controlled at up to 6 months post-training. At that time point, a sizable improvement in migraine-specific quality of life also consistently occurred (18,20). The burden of migraine in terms of migraine disability and quality of life diminished gradually with BT (21), which the current study confirmed for oBT, since the effects and ESs increased from the 6- to 16-month follow-ups (see Table 2). The use of analgesics did not change with both modes of training (18,20). However, headache top intensity, which was only assessed in oBT, nonetheless decreased (–26% post-training and –35% at the 6-month follow-up; see Table 3) and dropped further to –44% at the 16-month follow-up (see Table 3), which may also be regarded as a benefit of training.
Strengths and limitations
The predominant strength of this study is the prolonged measurement period, extending over 20 months, the first half of which covered a RCT up to the 6-month follow-up. Other major strengths include: (1) the large sample of participants with frequent episodic migraine of long duration that was medically well informed and under adequate treatment as usual (20); (2) a well-defined screening procedure based on an online diagnostic headache diary applying ICHD-II criteria and other validated measures, as well as an intervention based on an approved protocol that was developed specifically for migraine and following the guidelines for online treatment (17–19); and (3) reasonable and representative drop-out rates, notwithstanding the highly stringent criterion for attrition due to failure to keep the online headache diary on ≥25 of 30 days per measure point (20). The present sample fully delivered the post-training measurements, and 6 months later, exhibited less than 6% loss to follow-up (see Online Supplementary Material 2). In addition, the drop-out rate did not inflate the current results.
The major limitation of this study is the absence of a control condition for the data collected in months 10–20, and therefore interpretations of these findings should be cautious. Episodic migraine with six or fewer attacks per month has a relatively favourable prognosis over >10 years (42), and migraine tends to decrease with ageing (43); therefore, we could not rule out whether the effects established in oBT-d, and the evidence of effect maintenance for almost 1.5 years in oBT, are partly due to natural history or spontaneous recovery. In addition, a potential bias remained, which forms another limitation. The oBT completers closely resembled the group of allocated participants (see Tables 1 and 3), but differences in unmeasured characteristics could still persist, and these would then undermine the representativeness of the present results. A third limitation is that the number of days on which a certain agent was taken was used as the measure for rescue medications. We would have preferred to use the number of administrations per day, but this reporting had not been mandatory in the headache diary. We found no difference in outcome in cases that had also carefully registered the administration of their rescue medications, but this is inconclusive given the incomplete data for drug administration in the present study.
Hypothetical process of change and proposed future research
From a theoretical view on self-management, self-efficacy seems to be the most relevant indicator, since the concept is proximal to the execution of specific self-management behaviours (30,44). Locus of control, on the other hand, reflects causal outcome expectancies that are more distal to direct action (30,44). Self-efficacy may be driven by control beliefs, and evidence of control loci that are health promoting is important in specific health areas such as migraine (44). We did not methodically design our present study around these theoretical issues, but our secondary findings substantiate the existing knowledge of cognitive–motivational drivers in migraine self-management. As part of a RCT (45) Seng and Holroyd studied the dynamics of change (30) in a BT program that closely matched our (o)BT, and in patients highly comparable to the samples of our studies (17–21). They found that only baseline external locus of control predicted the BT effect on migraine self-efficacy, which, compared to internal control, was more strongly related to baseline self-efficacy (r = –0.64 for external control; r = 0.29 for internal control) (30). The latter was confirmed by our secondary data (r = –0.66 vs. r = 0.46, respectively) and, over time, this association increased only for external control (post-training: r = –0.82; 6-month follow-up: r = –0.81). We also showed that baseline external control inversely predicted the treatment effect of oBT (current result) and BT (18) on migraine attack frequency at the 6-month follow-up and that the BT effect on migraine self-efficacy and external control persisted, while that on internal control faded away over 3 years of follow-up (21). Taken together, these data suggest that migraine self-management is not primarily governed by perceived internal control, as is frequently assumed on a theoretical basis (44), and that perceived external control does not compromise the effectiveness of (o)BT in migraine; instead, individuals who begin BT believing that their migraine is influenced primarily by chance/fate have the potential to show the greatest positive change in self-efficacy (30). As our study was not designed to promote this claim, we suggest that future research should examine whether loss of external control paves the way to self-efficacy – the confidence in one’s ability to behaviourally prevent and manage one’s own attacks of migraine – which in turn instigates the execution of self-management behaviours.
Our studies (17–21) also yielded preliminary findings pointing towards three steps in the process of change induced by (o)BT. The first emerging change pertains to indicators of self-management (30). This appears to support reduced triptan use for attack abortion, which may seem risky, since attacks could flare up with less pharmacological help, but according to our results, this was not the case. The second signs of change occur in headache. It is not as yet clear whether the training impacts on attack frequency and headache top intensity consecutively (and in which order) or simultaneously, but we assume that headache intensity is more easily influenced by self-management than is the all-or-nothing occurrence of the attack proper. Decreased pain intensity could be the first effect to reinforce self-management, bolstering the reliance on one’s own behaviour and staging incidents of mastery that then extend to experiences of attack prevention. The third step consists of much slower but steady improvements in the consequences or burden of migraine: migraine-specific quality of life and disability start to change at or beyond the point of the 6-month follow-up, but they improve and gain stability thereafter. Future research should substantiate these steps of change in BT and subsequently identify the elements of intervention that add specifically to each step of improvement.
Conclusions
This study followed up patients with frequent episodic migraine for 20 months with an online headache diary and migraine monitor according to the ICHD-II. The results lend support to the benefits of oBT in frequent episodic migraine. Delayed oBT induced stronger improvements compared to ‘watchful waiting’ by means of an online headache diary that carefully assessed migraine and medication use (20); these changes matched those in the group that had directly received oBT, and the effects were observed differentially in the training episodes of the respective groups. In addition, the effects of oBT were durable over 16 months of follow-up.
Frequent migraine deserves special attention and effort in care (41,46), given the risks of disease progression to highly debilitating (near-) daily headaches (47,48) and possible neurodegenerative changes in the brain (49). Self-management variants such as oBT fit in with multidisciplinary care (50) and reach these patients conveniently with the potential to durably reduce attacks by a quarter of their frequency.
Clinical implications
Training in behavioural self-management with a proactive focus on attack prevention is a useful supplementary aid in the treatment of frequent episodic migraine of long duration. Patients can be actively involved in this venture. Real-time prospective monitoring of migraine and medication use (and, preferably, gains during training) is an important element. It requires an engaging electronic diary that is highly user friendly with graphical output in order to reinforce daily entry, regardless of whether a headache occurred. Support and supervision remain necessary, but the contribution of professional psychologists can be tailored to far below the dose of regular individual psychotherapy.
Footnotes
Acknowledgements
We thank the Dutch Society of Headache Patients and the Society of Dutch Headache Centers for their cooperation, in particular neurologist JL van der Zwan, who, together with the last author, served as point of contact for study participants as instituted by the UMCU Medical Ethics Committee. We are also grateful to all participants for taking part in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by grant # 1871 of the Health Insurers Innovation Foundation (Innovatiefonds Zorgverzekeraars) and by substantial support from the Utrecht University Faculty of Social and Behavioural Sciences.