
Abstract
Objectives
The objective of this article is to determine the relationship between headache frequency and socio-demographic data, personal characteristics, habits, daily activities, daily loss of ability, depression and anxiety in the headache subtypes in the pediatric population.
Patients and methods
Our sample group was composed of approximately 5355 children aged between 9 and 18 years. An eight-stage questionnaire was administered to the children. In the second stage of the study, headache subtypes were created according to the ICHD-II criteria. The resulting data were compared according to the results of the headache subtypes.
Results
In school-age children, the prevalence of recurrent headaches was 39.4%, and the prevalence of migraine was 10.3%. The subjects with migraine mostly preferred sedentary activities in their leisure time, and preferred less exercise than the subjects with the other headache types. The PedMIDAS score of the children who preferred to play sports was significantly lower than those who did not prefer to play sports. In the group that preferred reading books, an opposite relationship was found. In overweight and obese migraine sufferers, other types of headache were found to be significantly higher.
Conclusions
In the management of treating childhood headaches, the association of psychiatric comorbidities should be considered. To minimize disability, children should be directed to more useful physical activities.
Introduction
Epidemiological studies examining primary headaches in childhood are increasing. In the literature, the rate of childhood headache ranges from 5.9% to 82% (1–4). This rate varies for tension-type headaches (TTH) (4–7) and migraines (2,7–11) from 0.9% to 72.8% and 2.97% to 28%, respectively. This wide distribution depends on many things, such as methodological and geographical differences as well as socio-cultural and ethnic factors. Ankara is the capital of the Republic of Turkey with a population of 4,466,756 (2007 Turkey Statistical Institute (TSI) data). Because it is located in the middle of Anatolia, it receives immigrants from all parts of Turkey. Surprisingly, its population has increased over the past seven years by 40% (3,203,362 in 2000, TSI data).
In the last 30 years, the prevalence of migraine and the frequency of headaches have increased considerably. This increase in incidence is alarming. Changes in the lifestyles of children have been suggested as probable causes for this increase (12). A limited number of studies conducted show the relationship between headache and children’s lifestyle, diet, and habits (13–16). The number of studies that show the relationship between psychiatric comorbidities and headaches is low (17–19). Depression, anxiety, disability, and individual habits in children were studied in a limited number of studies separately (13–19), but have not been studied in a comprehensive manner. A study that showed the relationship between the children’s leisure time and headaches was not performed comprehensively. The study herein will show the prevalence of migraine and headaches in Turkish children. In particular, the scope of our work was to conduct a prevalence study to underscore the relationship between childhood headaches and leisure time preferences, depression, anxiety, daily disability and eating habits.
Methods
Study population
This cross-sectional study was conducted on school-age children by the Departments of Child Neurology and Child Psychiatry of Ankara University between November 2011 and May 2012. The study was performed on students in the fourth through 12 th grades with ages ranging between 9 and 18 years.
The distribution of all the students according to their schools.
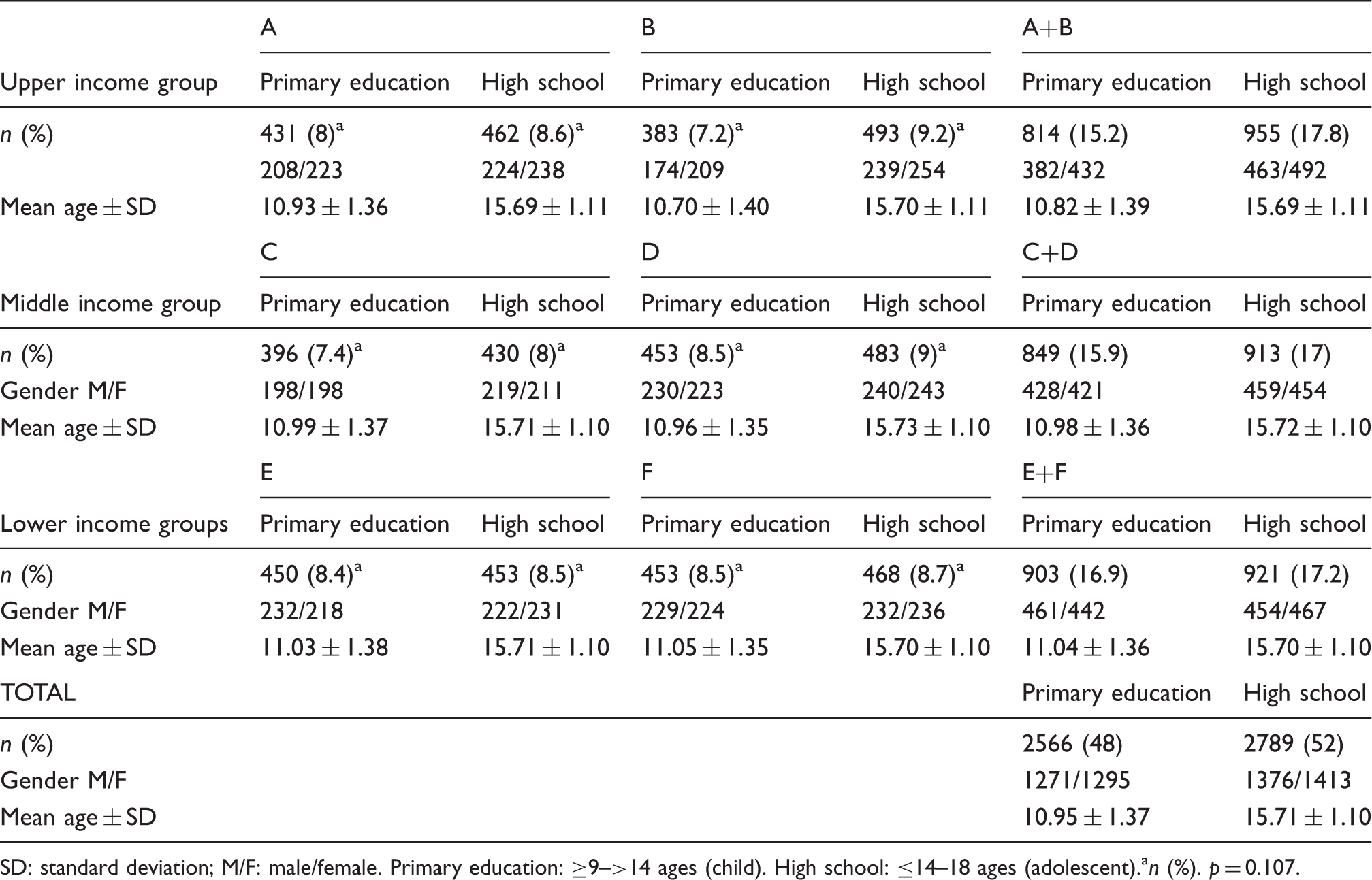
SD: standard deviation; M/F: male/female. Primary education: ≥9–>14 ages (child). High school: ≤14–18 ages (adolescent).an (%). p=0.107.
Study design
At each school, the study was conducted by a team of six people including a child psychiatrist and a child neurologist. The study was performed in two stages. The first stage consisted of a questionnaire of eight distinct sections. These forms were administered to multiple study groups of 25–30 people.
First stage
The first four parts of the survey asked for the participant’s general information (without stating names), childhood depression scale, the Beck Anxiety Inventory (BAI) (23), and eating habits. These surveys were completed by all the students participating in the study. In the fifth part of the survey, the individuals were asked if they had recurrent headaches. A recurrent headache was defined as a headache (of at least two occurrences during life) in the absence of an underlying cause (infection, trauma, etc.). The remaining two sections were completed by students who gave a positive answer to this question. Questionnaire 6 consisted of questions that were designed according to Department of International Classification of Headache Disorders, second edition (ICHD-II). This questionnaire consisted of eight questions about the headache episodes: frequency, location, duration, pulsating quality, intensity (moderate or severe), the occurrence of nausea, vomiting, photophobia and phonophobia, and aggravation by routine physical activity. Part 7 focused on pain history, pain intensity (on a 10-point pain scale), and whether he or she had been previously diagnosed with migraine. In part 8, the pediatric Migraine Disability Assessment Scale (PedMIDAS) was applied. All the forms that were applied are included in Appendix 1.
Second stage
The answers to part 6 were evaluated according to the criteria in the ICHD-II. In the second stage of the study, the students who were assumed to have headaches and migraine were evaluated by a child neurologist, and a headache classification was made. The headaches were classified as migraine, probable migraine, TTH and other headaches. The PedMIDAS was calculated. Students with chronic illnesses, trauma history, those who did not want to participate in the study, and those who had communication problems or did not understand the questions were excluded from the study.
Consents received for work
In accordance with the Ministry of Education of the Republic of Turkey, no student names, last names or other identifying information were included. The questionnaires that were distributed to the students were numbered; therefore, the numbers were used for identification instead of names and surnames. For the study to be conducted, a written consent was obtained from the Ministry of Education of the Republic of Turkey. The questionnaires, which were sealed by the Ministry, were duplicated and used. Consent was obtained from the local ethics committee of Ankara University and from the academic board of the Department of Child Health and Diseases, Faculty of Medicine, Ankara University. Written informed consent for the Turkish version of the questionnaires used in the study was received from the individuals and institutions that own the copyright.
Scoring of depression, anxiety and PedMIDAS scales that were used
For rating depression, a childhood depression scale compiled by the Association of Turkish Child Psychiatry, whose validity and reliability had been previously proven, was used (Appendix 1). The children with a depression score of 19 and above were considered depressive. The Turkish version of Beck anxiety scores, whose validity and reliability had been previously proven, was used (Appendix 1). Scores of 21 and above were considered positive. These diagnoses were also confirmed by a child psychiatrist in the second stage. For the PedMIDAS scoring, its verbatim Turkish version, whose validity and reliability had been proven, was used (Appendix 1).
The extent of disability was divided into four grades based on the total score on the PedMIDAS. Grade I had scores ranging from 0 to 10, indicating little to no disability. Grade II had scores ranging from 11 to 30, indicating mild disability. Grade III had scores ranging from 31 to 50, indicating moderate disability. Grade IV had scores >50, which indicated severe disability.
Statistical evaluation of the study
The statistical evaluation of this study was conducted blindly by the members of the Department of Statistics, Faculty of Medicine, Ankara University.
Statistical analyses were performed using the statistical software for Windows (version 15 SPSS Inc, Chicago, IL, USA). All variables, reported as mean and standard deviation or as median, were analyzed by the Kolmogorov-Smirnov test according to the distribution of the variables. Normally distributed data were subjected to parametric statistical methods (student t-test, one-way analysis of variance (ANOVA)). The Kruskal-Wallis and the Mann-Whitney U nonparametric tests were also used to correlate the data, while the chi-square test was used to determine proportions. Following a gender and age adjustment, a multivariate logistic regression analysis was used to determine the associations between headache groups and others parameters (income levels, mother’s and father’s education level, obesity, anxiety, depression, habits, grade point averages, and PedMIDAS scores). A 95% CI was determined using an odds ratio (OR). A p value ≤0.05 was considered statistically significant for this study.
The null hypothesis:
HO: Childhood headaches are not triggered by sedentary activities, anxiety, depression, and dietary intake. The alternative hypothesis HA was defined as HA: Childhood headaches are triggered by sedentary activities, anxiety, depression, and dietary intake.
Results
Overall evaluation results
The study was conducted with 2566 (48%) primary school students and 2789 (58%) high school students. Of the 5355 subjects who participated in the study, 2647 (49.4%) were male, and 2708 (50.6%) were female. Elementary student enrollment consisted of 1271 (49.5%) male and 1295 (50.5%) female students. Of the high school students enrolled in the study, 1376 (49.3%) participants were male and 1413 (50.7%) were female. The mean age was 13.4 ± 2.68, and the range was 9–18. When the schools were divided among themselves and according to income levels, there was no significant difference in the average age and gender distribution (p > 0.05) (Table 1).
Evaluation of the results in terms of prevalence
The demographic data of the study group according to the headache classes, and comparisons of obesity, parental education levels and grade point averages.

Obese: >95 pounds. Overweight: 85–95 pounds by age.ap < 0.05. SD: standard deviation. M/F: male/female. The first data show percentages in the groups, the second data show overall distribution. The first p (P1) shows the statistical difference in the headache groups; the second p (P2) shows the statistical difference in overall distribution children (including non-headache).
Next, we compared pre-pubertal versus pubertal children for headache types. In this study, the age that defined the cutoff for pubertal children was set at 11 years of age, which is consistent with a previously published report on the pubertal age of Turkish children (24). Our study determined that 11.7% (442) of the pubertal children had a migraine, 10.4% (394) had a probable migraine, 17.7% (668) TTH, and 3.4% (128) had other headaches. However, pre-pubertal children had different ranges including 6.8% (108) migraine, 8.2% (129) probable migraine, 13.6% (215) TTH, and 1.8% (29) other headaches. A comparison of pre-pubertal versus pubertal children and the association with recurrent headaches is shown in Figure 1.
Comparison of pre-pubertal versus pubertal children and recurrent headaches according to their subtypes.
Evaluation of the results in terms of socio-economic aspects
When the headache subtypes were evaluated in terms of the income levels, they did not differ significantly (p > 0.05). Migraine diagnosis among patients had no observed statistical difference with the father’s education level, but a strong statistical significance with the mother’s education level. When the headache subtypes were evaluated in terms of the number of siblings, they did not differ significantly (Table 2) (p > 0.05).
Evaluation of the results in terms of school achievement and body mass index
When the headache subtypes were classified based on obesity, 8.7% of migraine sufferers, 6.9% of probable migraineurs, 5.1% of TTH, and 5.7% of the other headaches were observed to be obese. This difference was statistically significant (p ≤ 0.05). The average of body mass index was 4.20 ± 3.52 for migraineurs, 9.19 ± 3.00 for probable migraineurs, 9.19 ± 3.16 for TTH, and 1.20 ± 3.02 for other headaches. When a post-hoc analysis was performed, the grade point average of students suffering from migraine was significantly higher than students with probable migraine and TTH (p ≤ 0.05). Studies of school success and migraine association indicated that students with recurrent migraine had a grade point average of 71.1 ± 10.36, while probable migraineurs, TTH, and other headache groups were 73.2 ± 11.96, 73.8 ± 13.82, and 74.4 ± 11.73, respectively. Strikingly, a post-hoc analysis showed that the grade point average of children with migraine was significantly lower than all other headaches (p ≤ 0.05).
Evaluation of the results related to nutrition and habits
Of 550 students with migraine, 252 (45.8%) stated that the attacks were triggered by food. One hundred and eight students (19.6%) stated that cola and coffee were foods that triggered the attacks, 50 students (9.1%) indicated a fried food reaction, 17 students (3.1%) stated spicy food, 16 students (2.9%) stated chocolate, 15 students (2.7%) stated canned products, 13 students (2.4%) stated tea, 13 students (2.4%) stated peanuts, 12 students (2.2%) stated cheese, and eight students (1.5%) stated other foods (sausages, salami, fish, fruit) as foods that triggered their attacks.
Of the individuals, 36.5% of migraine sufferers (201), 32.7% of probable migraineurs (171), 28.8% of the children with TTH (228), and 22.3% of the other headaches (35) stated that they did not have regular sleep habits. This difference was statistically significant (p=0.001). Of the migraine sufferers, 51.8% of migraine sufferers (285) expressed that they went to school without breakfast. Of the other headache types, 50.7% of the probable migraineurs (265), 46.1% of the children with TTH (407), and 42% of the other headaches (66) stated that they went to school without breakfast (p=0.044).
Comparison of headache classes in terms of daily activities, eating habits and habits.

According to the post-hoc analysis, migraineurs have significantly higher cola consumption than the other headache groups.
According to a post-hoc analysis, in coffee consumption, migraineurs have significantly higher coffee consumption than those with TTH and other headaches.
According to a post-hoc analysis, migraineurs have significantly higher tea consumption than possible migraineurs.
According to the post-hoc analysis, migraineurs have significantly higher cola consumption than the other headache groups.
Cola in cans (330 ml–100 ml/13 mg caffeine), coffee in cups (200 ml–100 ml/60 mg caffeine), tea in glasses (150 ml–100 ml/28 mg caffeine).
The first p (p1) shows the statistical difference in the headache groups. The second p (p2) shows the statistical difference in overall distribution children (including non-headache).
TTH: tension-type headache; SD: standard deviation.
Evaluation of anxiety, depression and PedMIDAS scores
Comparison of headache classes according to anxiety, depression and PedMIDAS scores and their levels.
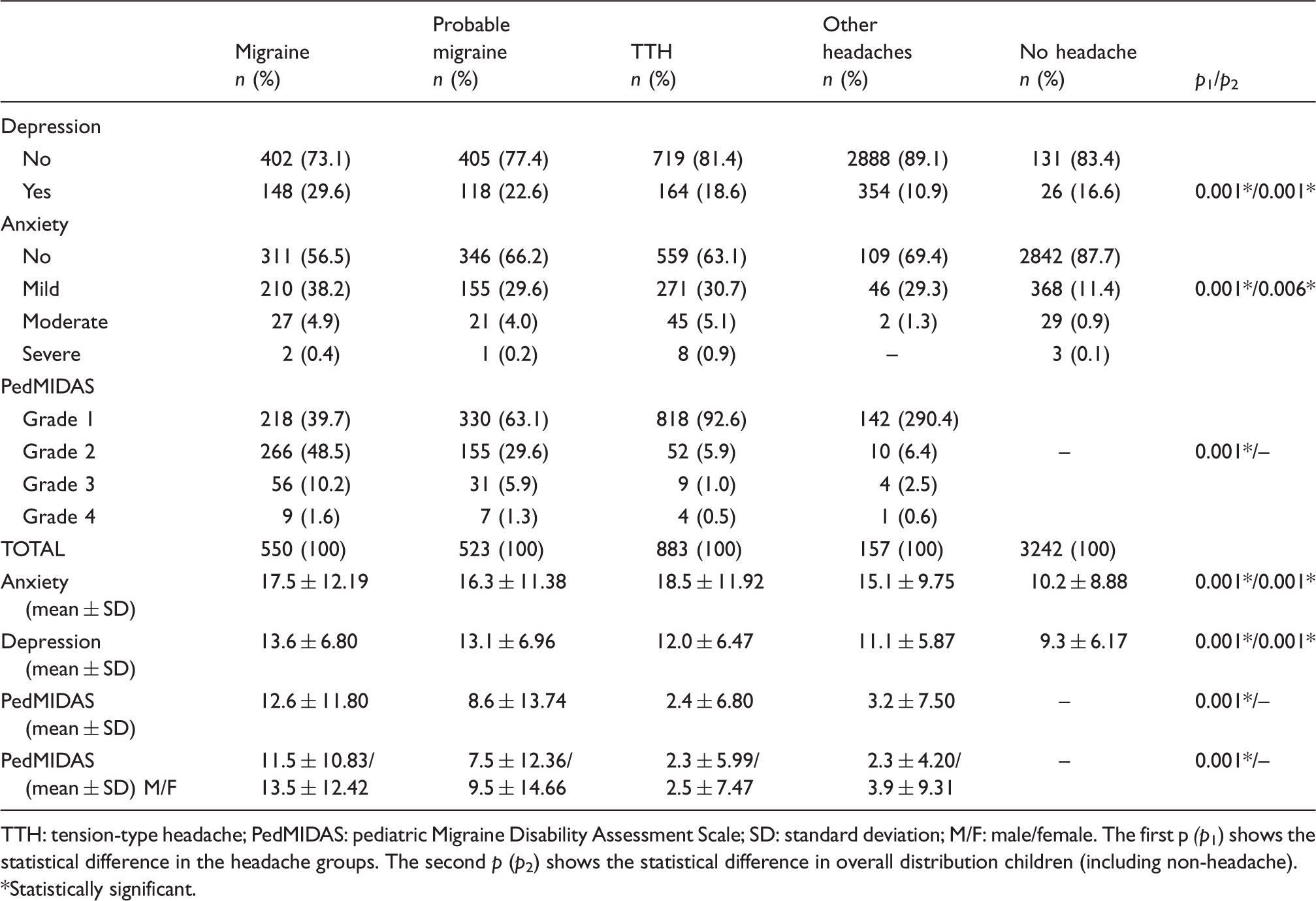
TTH: tension-type headache; PedMIDAS: pediatric Migraine Disability Assessment Scale; SD: standard deviation; M/F: male/female. The first p (p1) shows the statistical difference in the headache groups. The second p (p2) shows the statistical difference in overall distribution children (including non-headache). *Statistically significant.
A comparison of the PedMIDAS scores of the subjects who had positive anxiety, depression, and obesity in the headache subtypes is shown in Figure 2. In Figure 3, a comparison of the PedMIDAS scores of migraine sufferers who prefer music, sports, television, computers, and books for leisure time activities and those who do not prefer these activities is given.
Comparison of the PedMIDAS scores of individuals who have anxiety, depression and obesity in the headache subtypes. Comparison of the PedMIDAS scores of migraine patients who prefer sports, music, books, computer and television to pass their leisure time and those who do not enjoy these activities.

After age and gender were adjusted, a multivariate logistic regression analysis was performed on all the variables between students with and without migraine. This analysis determined that the mother’s education level (OR: 1.63, 95% CI: 1.12–2.20, p=0.001), the presence of obesity (OR: 1.50, 95% CI: 1.11–2.01, p=0.007), a low grade point average (OR: 0.97, 95% CI: 0.96–0.98, p=0.001), the presence of anxiety (OR: 1.45, 95% CI: 1.16–1.82, p=0.001) and a high PedMIDAS score (OR: 7.68, 95% CI: 4.98–11.87, p=0.001) were related to migraine (not shown). While there was a positive correlation between migraine and body mass index, anxiety, depression, and PedMIDAS scores, there was a negative correlation with grade point average.
Discussion
In this study, we found that the prevalence of recurrent headaches was 39.4% and the prevalence of migraine was 10.3% in school-age children. Our rates were lower compared to another study conducted on Turkish children that found a 59% prevalence of recurrent headaches and a 14.5% of migraine (2). The main objective of our study was not to determine the prevalence. When we consider the size of our sample group, the age range, and migration rate to the province of Ankara from all over Turkey, we think our rates are important in terms of reflecting the averages in Turkey.
Changes in the emotional status during puberty are important, so it should be determined if the emotional problem/change is a comorbidity or the primary issue (12). Symptoms of depression, which include sadness, tearfulness, withdrawal from activities, and hopelessness, need to be checked (12). In studies that focused on migraine and were performed on adults, the rate of anxiety and depression was found to be 2 to 5.3 times higher in migraine patients. The presence of comorbid psychiatric diagnoses is thought to complicate treatment outcomes in headache (25,26). Some studies conducted on children showed that TTH had a relationship with anxiety and psychiatric comorbidities that included depression (27). Studies conducted on children and adolescents indicated that the general prevalence of anxiety disorders ranged between 2% and 24% (26,27). The prevalence of major depression ranged from 0.2% to 17% (27–31). When dysthymia and the prevalence of minor unclassified depression are added, this rate is higher. Our prevalence of anxiety in children without headaches was 22.8%, and the prevalence of depression was 16.6%, which were similar to previous studies. In our study, we found that the prevalence of anxiety, especially in migraineurs (43.5%), and the prevalence of depression (29.6%) were much higher than that of the general population and those with other types of headache. The PedMIDAS scores of migraineur children with depression and anxiety were significantly higher than the other types of headaches. These data may show us that, in the management of migraine treatment, psychiatric comorbidities should be considered as much as TTH.
Previous studies showed a lack of statistical significance between the family’s income level and migraine (10,32), however; other studies showed that migraine was more frequent in societies with low socio-economic levels (33). In our study, we did not find differences between migraine and family income level. Consistent with previous studies, we found that the migraine rates were significantly higher in female students. The education levels of the mothers were significantly higher in children who had migraine. We thought that this might be due to the prescriptive life that educated mothers imposed on their children and the stress that result in the children.
Diet, lifestyle, and habits are perceived as factors affecting headaches in children. Many studies conducted on adults investigated the effects of lifestyle and diet on headaches (34). A previous study showed that inadequate fluid intake, irregular meals, and diet-related factors such as high caffeine consumption increased the frequency and duration of attacks and triggered the attacks (35). It was shown that some other habits, including smoking and alcohol consumption, were related to headaches (36,37). In a small number of studies conducted on children, it was shown that caffeine consumption, irregular breakfasts, and a lack of regular sleep habits had a relation with headaches (13–16,35). In these studies, the sample groups were small, the age ranges were narrow, and the income status was not taken into consideration or the studies covered only certain types of headaches
In our study, it was found that a lack of regular sleep and irregular breakfast habits were significantly higher in children with headache than in those without headaches. These observations were significantly higher in migraineurs than in those with other headache types. It was observed that children with migraine mostly preferred to spend their leisure time reading books. They did not prefer photophobia sources such as television, the Internet, and phonophobia sources such as music. The relationship between reduced physical activity and migraine was previously shown. It was based on the hypothesis that patients avoided exercise because physical activity could trigger the attacks (36). In our study, we observed that migraineurs preferred sports in leisure time less often than the patients with other headache types. The PedMIDAS scores of the children who spent their free time playing sports were lower. This finding supports the studies that indicated that physical activity had a positive impact on the management of migraine treatment (13). Scores were higher in children who preferred reading books, watching TV, and using computers in their spare time (Figure 3). Collectively, this suggests that reduced physical activity is a risk factor for migraine sufferers and that these patients should be persuaded to perform more physical activity.
A limited amount of physical activity contributes to obesity and being overweight in patients with recurrent headaches. Recent data showed a relationship between obesity and migraine (38). The mechanisms that link obesity with the frequency of a migraine attack are uncertain, but they may be connected from a biochemical perspective (39). It is known that obesity is a proinflammatory and prothrombotic state, and neurovascular inflammation might be an important mechanism of migraine. It is thought that obesity triggers pain by releasing proinflammatory mediators such as calcitonin gene-related peptide and substance P, resulting in the stimulation of the trigeminal ganglion nociceptor (39).
In our study, the rate of headache activation through foods was found to be as high as 46.6% in migraineurs. Caffeinated beverages such as cola and coffee and fried foods were the primary triggers among the foods that caused attacks. Although cola, coffee and tea trigger migraine attacks, the rate of consumption was significantly higher in the migraineurs. In our study, migraineurs had higher levels of maternal education but a lower grade point average. Because there is a competitive examination system in our country, we think that pressure from educated parents contributes to the headaches. The pressure and stress could potentially be the root of increased consumption of caffeinated beverages and tea, which have a stimulating effect to increase study habits even though these beverages trigger attacks.
Our study has some limitations. Like many other cross-sectional studies, our study was performed using a specific time-point questionnaire and was not carried out in a time-dependent fashion. The headache classification was determined based on the valid ICHD-II criteria at the initiation of the study and not the newly drafted ICHD 3-beta criteria. In addition, the parents or guardians of the children were not interviewed for this study as advised by the Ministry of National Education. We were advised not to ask questions that pertained to menarche or alcohol consumption, since the children may not provide an honest answer.
In this comprehensive study, we broadly present the headache prevalence and the distribution of chronic headaches, the effects of diet, lifestyles and habits on headache, the relationship between anxiety, depression and headaches, and the loss of daily life activity in school children and different socio-economic groups. This study showed a relationship between recurrent headaches with caffeinated beverages, obesity, lack of regular sleep, irregular breakfast habits, parental education level, depression and anxiety. We believe that this comprehensive synoptic study will shed light on studies that will be conducted on pathophysiology and treatment in the future.
Clinical implications
We found that the prevalence of recurrent headaches was 39.4% and the prevalence of migraine was 10.3% in school-age children. The pediatric Migraine Disability Assessment Scale (PedMIDAS) scores of the children who spent their free time playing sports were lower. The score was higher in children who preferred reading books, watching TV, and using computers in their spare time. The mother’s education level, the presence of obesity, a low grade point average, the presence of anxiety, and a high PedMIDAS score were related to migraine.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgments
We would like to thank Dr Levent İnanc, Dr Ozan Akinci, Dr Idil Daloglu, Dr Ayş e Kartal, Dr Arzu Yımaz, Neva Bektaş, Assoc. Prof Dr Ersoy Civelek, Özge Tıraş, Dr Ali Rıza Yamur, Dr Betül, Dr Elif and Dr Şerife Bektaş and all the teachers who helped us.