
Abstract
The goal of this study was to collect and analyse information on the prevalence of childhood migraine and disability due to migraine in primary school children of 4th to 8th grades (ages ranging from 9 to 17 years) in the Aydin urban area. A cross-sectional school-based study was conducted between March and June 2004. There were 76 333 children of 4th to 8th grades in primary schools in Aydin. Nearly 10% of this population (7721 out of 76 333) was evaluated by a multistage clustered sampling procedure. Four questionnaire forms were applied to each child by a study neurologist during class time. Questionnaire A consisted of a single question, ‘Have you ever had a headache?’. To those who responded ‘yes’, questionnaire B was applied as a second step, which consisted of eight questions. Diagnosis of migraine headache was made according to International Classification of Headache Disorders 2004. Migraine disability was measured with questionnaire C, which was originally the Pediatric Migraine Disability Assessment (PedMIDAS). Migraine history, previous migraine diagnosis and pain intensity were measured with questionnaire D. According to questionnaire A, 79.6% of boys and 87.1% of girls suffered from headaches. The prevalence of migraine was 9.7% (7.8% in boys, 11.7% in girls) according to questionnaire B. The male:female ratio was 1:1.5. Total PedMIDAS score was 9.94 ± 8.41 days in boys and 11.50 ± 12.28 days in girls. Only 1.9% of the children had previously been diagnosed with migraine. The average migraine headache history was 2.48 ± 1.18 years in girls and 2.57 ± 1.18 years in boys. Although migraine is a common health problem among school children in Aydin, it is mostly still under-recognized.
Introduction
The clinical features of childhood migraine usually resemble those of adult migraine. Many of the criteria used to diagnose migraine in childhood are same as those for adults, namely uni/bilateral pain location, pulsatile quality of pain, nausea and vomiting, photophobia and phonophobia, prodromal symptoms and aura, aggravation by routine daily activities and relief after rest or sleep, except for the duration of pain (1–9). Childhood migraine headache attacks usually have shorter duration and sometimes a bilateral location. Adult migraine lasts for 4–72 h, whereas childhood migraine usually ends in 1–4 h (10–14). On the other hand, International Headache Disorders (IHD)-2004 criteria accept a shorter duration of headache than the International Headache Society (IHS)-1988 criteria (5, 9). Many authors have proposed reducing the lower limit to 1 h and others have proposed a further reduction to 30 min (11–13). Migraine duration has caused difficulties for clinicians in the treatment of children with migraine, as well as for researchers in providing consistency in their studies and results. Some researchers consider full recovery and complete resolution of symptoms as the end-point of headache attacks, whereas for others the duration implies solely the duration of headache (10, 14). In order to provide consistency, IHD-2004 criteria were developed and our study was designed based on these rules.
The age-specific prevalence of migraine headache from childhood to adulthood represents a steadily increasing trend (15). In epidemiological studies designed according to IHS-1988 criteria, migraine prevalence was between 2.4% and 28%, respectively (16, 17). It is important to find a solution to the problem of migraine headache because of its impact on children's school, home and social life.
Materials and methods
This cross-sectional, school-based study was conducted between March 2004 and June 2004 in Aydın, which is located near the Aegean coast of Turkey and has a population of 1 million. Primary school children of 4–8th grades residing in the Aydın urban area were enrolled. Statistical data and official permission were acquired from the governor of Aydın.
Data collection
We divided the Aydın urban area into four different geographical areas. Six schools were selected randomly in each area. A screening questionnaire was distributed during class time to all students who were between the 4th and 8th grades. The population of students between the 4th and 8th grades in Aydın during the 2003–2004 education year was 76 333, and 7721 students (nearly 10% of the total population of these grades) were enrolled. Standard questionnaire forms were distributed to all students (Table 1). Students were grouped into 10–15 cases in each class and a detailed explanation of each question was made by a study neurologist in each class before answers were given. This amounted to face-to-face conversation. Students who could not read at that time, who could not understand the questions or who had communication problems or a history of a systemic disease or a head trauma were excluded.
Questionnaire forms
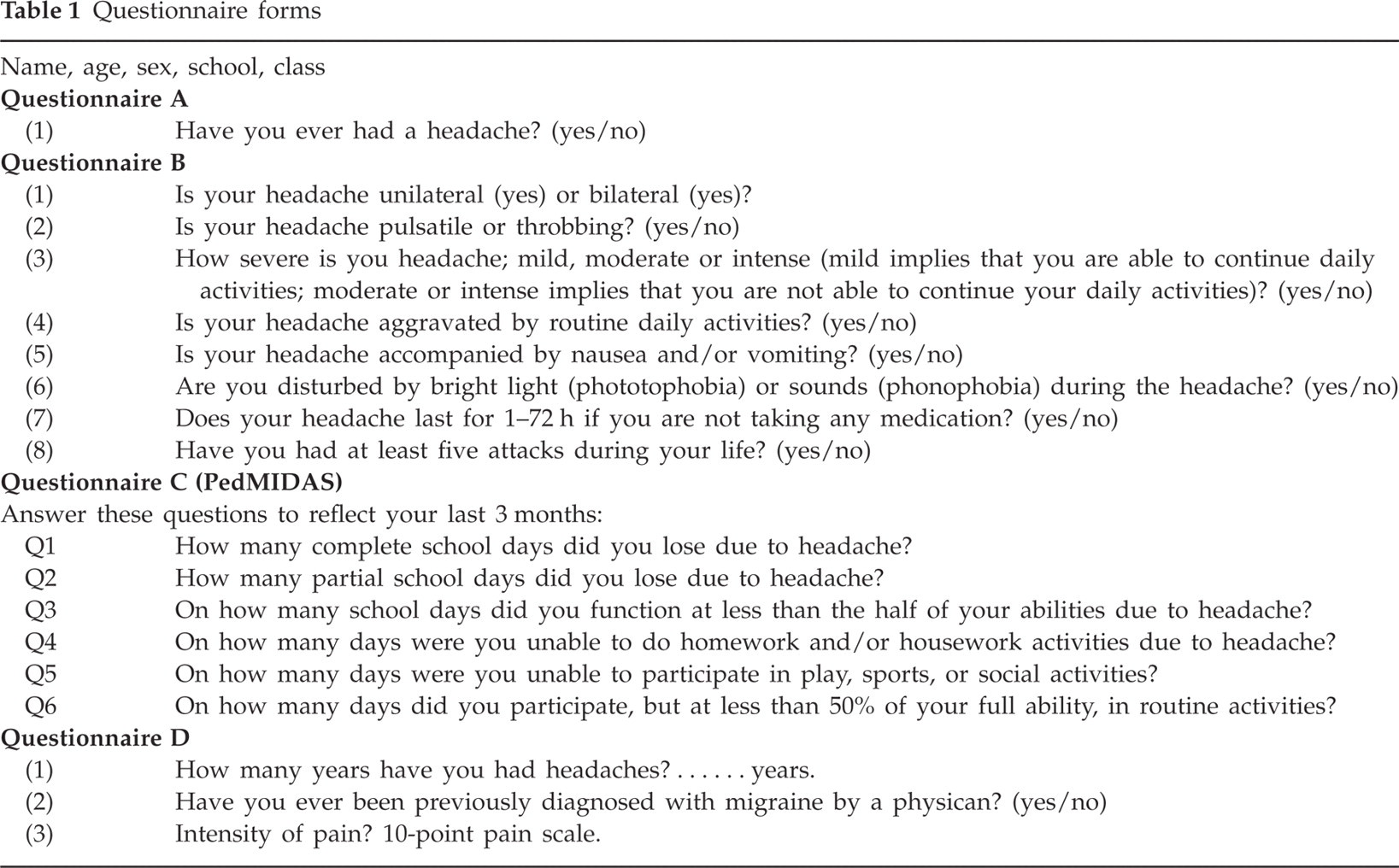
Design
Questionnaire A form consisted of a single question: ‘Have you ever had a headache?’. To those who responded ‘yes’, a self-administered questionnaire, the English version of which has been validated, designed according to IHD-2004, was given (questionnaire B) and answered under guidance as mentioned above in Data collection. The other students were discarded. Questionnaire B consisted of eight questions about the headache episodes: frequency, location, duration, pulsating quality, intensity (moderate or severe), aggravation by routine physical activity, and occurrence of nausea, vomiting, photophobia and phonophobia. If there were at least two ‘yes’ answers to the first four questions and at least one ‘yes’ answer to the next two questions, and a ‘yes’ answer to both of the last two questions, a diagnosis of migraine was made according to IHD criteria. Children then also completed the Pediatric Migraine Disability Assessment (PedMIDAS-questionnaire C) questionnaire, which asked for the children to record their lost time due to headache, such as in homework and/or non-work activities (family, social and leisure activities). Total PedMIDAS scores were calculated according to Hershey and colleagues (18). Finally, questionnaire D was applied, which consisted of three questions on pain intensity (on a 10-point pain scale), pain history and whether the student had previously been diagnosed with migraine (Table 1).
Data analysis
SPSS for Windows version 10.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses and P < 0.05 was considered to be statistically significant. χ2 tests, Student's t-tests and Mann–Whitney U-tests were used for calculations and statistical analyses.
Results
There were 7721 students [3875 boys (50.2%) and 3846 girls (49.8%)] in this study. The mean age was 13.08 ± 1.92 years (± SD) (range 9–17 years). A total of 6431 (83.3%) responded ‘yes’ in questionnaire A (response rate 79.6% in boys and 87.1% in girls).
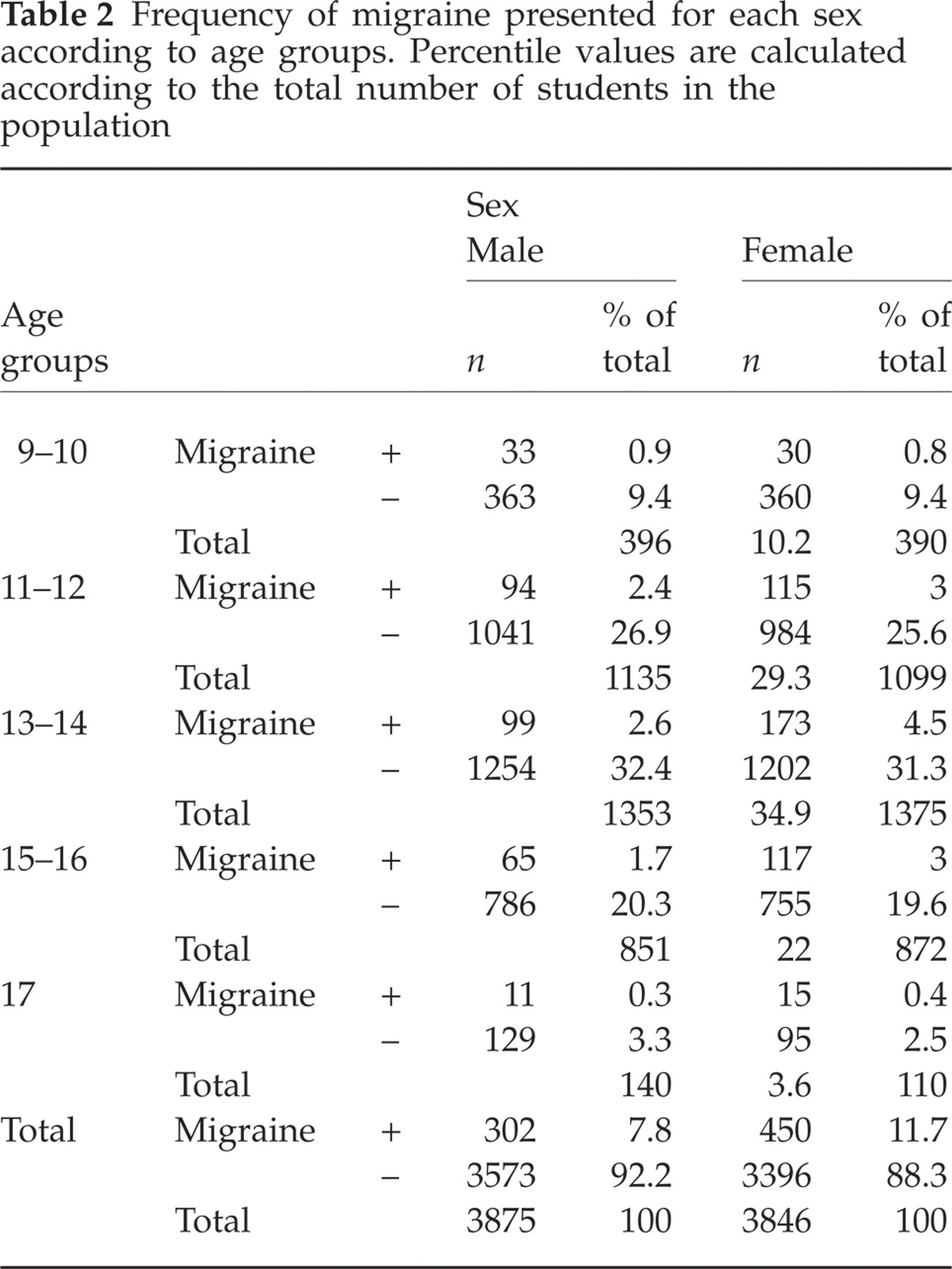
Migraine was diagnosed in 752 children (9.7%) according to questionnaire B; 450 girls (11.7%) and 302 boys (7.8%). The female:male ratio is 1.5 : 1. Migraine was significantly more frequent in girls than in boys (P < 0.001). The frequency of migraine was similar between 9 and 11 years of age in both sexes; however, it was more common in girls between 12 and 17 years old. Among girls, the highest prevalence occurred at the age of 13 years (Table 2). Migraine prevalence increased gradually with age in both sexes (P < 0.05).
Frequency of migraine presented for each sex according to age groups. Percentile values are calculated according to the total number of students in the population
According to questionnaire B, 76.5% had unilateral migraine headaches and the rest bilateral. Migraine headache was scored as moderate or severe in 77.7%; a pulsating quality was recorded in 76.9%, photophobia and phonophobia in 75.8%, associated nausea and/or vomiting in 69.8% and aggravation by routine physical activity in 59.6% (Table 3).
Answers to Questionnaire B presented for each sex in students with migraine. Percentile values are calculated for each question

The answers to Questionnaire C (PedMIDAS) are presented in Table 4. Total PedMIDAS scores were found to be 9.94 ± 8.41 days in boys and 11.50 ± 12.28 days in girls per 3 months. There were no statistically significant differences between the sexes with respect to PedMIDAS disability scores (P > 0.05, Mann–Whitney U-test).
Answers to Questionnaire C (PedMIDAS) presented for each sex in students with migraine

According to questionnaire D, headache history was 2.48 ± 1.18 years in girls and 2.57 ± 1.18 years in boys. There was no significant difference between the two groups (P > 0.05).
Among the respondents only 125 of 6431 (1.9%) reported that they had been previously diagnosed with migraine by a physician.
The mean headache intensity was 6.01 ± 2.17 in boys and 6.33 ± 2.24 in girls on a 10-point pain scale. The pain intensity was significantly higher in girls than in boys (P < 0.029, Mann–Whitney U-test).
Discussion
Headache is one of the most common neurological problems in children, although it may be under-recognized. In children with significant school absenteeism, possible psychosocial stressors such as school, family or relationship problems should be investigated. Migraine occurs especially in children who report feelings of unhappiness, fear of school failure or fear of a teacher (19). At the same time, frequent school absenteeism is a significant stressor which results in a decrease in academic performance, social interactions with peers and self-esteem. These factors also often aggravate pain perception (20). It is obvious that school is important not only for the intellectual development of children but also for their emotional and social development.
Although clinical evaluation is the gold standard in the diagnosis of migraine headache, a self-administered questionnaire form might help to diagnose migraine more accurately (18, 21–27).
Headache prevalence in the paediatric age group is reported in the literature to be 57–82% among 7–15-year-olds (2, 28). In our population, we found headache prevalence to be 83.3% (79.6% in boys and 87.1% in girls), which is slightly higher than in the literature.
In epidemiological studies migraine prevalence in childhood and adolescence has been reported to range between 2.4% and 19% (16, 17). We found the prevalence of childhood migraine in the Aydın urban area to be 9.7%. Our result is higher than in studies in Sweden (3.9% aged 7–15 years), Canada (2.4% aged 12–14 years and 5.0% aged 15–19 years), Finland (5.7%, age 7 years), Saudi Arabia (6.2% aged 6–15 years), Hong Kong (0.5% migraine and 0.7% probable migraine aged 6–13 years), the USA (2.1% in boys and 2.3% in girls aged 6–17 years), Greece (6.2% aged 4–15 years), Poland (8.42% aged 6–19 years) and Chennai, India (4% aged 7–15 years); similar to childhood population studies in Scotland (10.6% aged 5–15 years), Brazil (9.9% aged 10–18 years), Denizli, Turkey (8.8% aged 11–18 years), the USA (3.2–10.6% < 15 years old); and lower than in childhood population studies in Jaipur, India (9% in boys and 14% in girls aged 11–15 years) and another study in Sweden (11% aged 7–15 years) (2, 16, 17, 29–40). It is clear from the above that migraine prevalence may vary in different parts of the same country.
Migraine occurs with similar frequency in both sexes before the age of 10 but is more common in girls after the age of 11 years (41–45). Our female:male ratio was 1.5 : 1.0, which is similar to the US population (1.4 : 1.0) (17). Migraine frequency was similar in both sexes between 9 and 11 years of age but was more common in girls aged 12–17 years. This sex difference may reflect the influence of female hormones, and our results are consistent with the literature (2, 37, 44, 45). Among girls the highest prevalence is at 13 years old (menarche age in Turkey is 13.28 ± 1.09 years in Ankara (46) and 12.9 ± 1.0 in Denizli (37)). Migraine prevalence increases gradually with age in both sexes, consistent with the literature (10–13, 17, 28, 31, 36, 38, 47, 48).
Although primary school education is mandatory in Turkey, some families delay sending their children to school, especially girls. Some children begin school in a later age because their families have moved from other areas. For this reason, a number of students were older than their classmates.
In our study group 76.5% had unilateral migraine headache and the rest bilateral. Moderate or severe headache was noted in 77.7%, a pulsating quality in 76.9%, photophobia and phonophobia in 75.8%, associated nausea and/or vomiting in 69.8% and aggravation by routine physical activity in 59.6%. Intensity of pain, pulsating quality, nausea and vomiting, photophobia and phonophobia are the most important criteria, and aggravation of headache by physical activity the least important. Consistent with the literature, we found no significant difference between the sexes with respect to migraine symptoms (6, 14, 49).
A new concept in the new classification is ‘probable migraine’. Probable migraine is considered when all criteria but one are fulfilled in questionnaire B. Because we aimed to show the prevalence of definite migraine, we did not include this concept in the study.
School-related disability is one of the most important components of a child's quality of life. School is important for social, intellectual and emotional development in childhood. Migraine headache may cause lost school time or impact a student's school or homework performance. In one study, 44% reported that they stayed in bed during attacks and 26% stated that they were sometimes absent from school due to attacks (50). Many studies have found that migraine attacks brought significant disruption to family life, with an impact on spouses, children and friends (51–53). We evaluated this disability by means of questionnaire C (PedMIDAS). Total PedMIDAS scores were 9.94 ± 8.41 days in boys and 11.50 ± 12.28 days in girls for a period of 3 months, which is lower than in the literature (25 ± 36.3) (17). There was no statistically significant difference between the sexes. Loss of complete school days due to headache was 0.89 ± 1.67 days in boys and 0.72 ± 1.53 days in girls for a 3-month period. Partial school day loss due to headaches was 0.52 ± 1.24 days in boys and 0.45 ± 1 days in girls for a 3-month period. Our population's school day loss due to headache was lower than for US and UK children (17, 18).
According to questionnaire D, the mean age was 13.08 ± 1.92 years and headache history was 2.48 ± 1.18 years in girls and 2.57 ± 1.18 years in boys. There was no significant difference between the two sex groups. The average age of onset was significantly higher than in the US population (6.6%) (50).
Mean pain severity was 6.01 ± 2.17 in boys and 6.33 ± 2.24 in girls, on a 10-point pain scale, which is higher than in the literature (5.6 ± 2.3) (17).
Among the respondents only 1.9% reported that they had previously been diagnosed with migraine by a physician. This result is lower than in the literature (19.8%) (54).
This is the first epidemiological and prospective study evaluating the prevalence and characteristics of migraine in childhood based on IHD-2004 in the Aydın urban area. Because we used the new criteria, we hope the results will be a reference for future studies. In addition, this is the first study to reveal disabilities in childhood migraine in the Turkish child population. It shows that migraine in childhood is indeed a serious and under-recognized health problem in the Aydın urban area, deserving of attention to find a solution.
Acknowledgements
The authors thank Professor Dr Çiçek Wöber Bingöl for editing the manuscript, the governor of Aydın and the management of Astra Zeneca-Turkey for their support.