
Abstract
Introduction
We aimed to field-test the beta version of the third edition of the International Classification of Headache Disorders (ICHD-3 beta) diagnostic criteria for classical trigeminal neuralgia (TN). The proposed beta draft of the 11th version of the International Classification of Diseases (ICD-11 beta) is almost exclusively based on the ICHD-3 beta classification structure although slightly abbreviated. We compared sensitivity and specificity to ICHD-2 criteria, and evaluated the needs for revision.
Methods
Clinical characteristics were systematically and prospectively collected from 206 consecutive TN patients and from 37 consecutive patients with persistent idiopathic facial pain in a cross-sectional study design.
Results: The specificity of ICHD-3 beta was similar to ICHD-2 (97.3% vs. 89.2%, p = 0.248) and the sensitivity was unchanged (76.2% vs. 74.3%, p = 0.134). The majority of false-negative diagnoses in TN patients were due to sensory abnormalities at clinical examination. With a proposed modified version of ICHD-3 beta it was possible to increase sensitivity to 96.1% (p < 0.001 compared to ICHD-3 beta) while maintaining specificity at 83.8% (p = 0.074 compared to ICHD-3 beta).
Conclusion
ICHD-3 beta was not significantly different from ICHD-2 and both lacked sensitivity. A modification of the criteria improved the sensitivity greatly and is proposed for inclusion in the forthcoming ICHD-3.
Keywords
Introduction
In the summer of 2013 the International Headache Society (IHS) published the beta version of the third International Classification of Headache Disorders (ICHD-3 beta) (1). Its criteria were based on the opinion of experts including IHS representatives as well as leading experts from outside the headache field, most often representatives from the International Association for the Study of Pain (IASP). The proposed beta draft of the 11th version of the International Classification of Diseases (ICD-11 beta) of the World Health Organization (WHO) is so far based on the ICHD-3 beta criteria in a slightly adapted form and will in the following be referred to only as the ICHD-3 beta criteria. IHS and WHO strongly encourage field-testing of the new diagnostic criteria. This is best performed in a clinical setting with a large and representative cohort of patients.
The Danish Headache Center (DHC) is a neurological center for headache and facial pain. It receives patients from all over Denmark. We have a large volume of classical trigeminal neuralgia (TN) patients from the full spectrum of the disease as patients suspected to have TN can be referred directly from general practitioners, private neurologists and other hospital departments. Those patients referred to the Department of Neurosurgery at The National Hospital of Denmark, are referred by the neurosurgeon to DHC for pre-surgical evaluation. We therefore considered our cohort of TN patients to be representative and suitable for field-testing of the diagnostic criteria and the specialist evaluation of diagnosis performed by experienced neurologists to represent the “gold standard” as the diagnosis of TN is primarily based on history.
Patients suffering from persistent idiopathic facial pain are useful as a control group because they pose one of the most challenging differential diagnoses (2,3). Patients suspected to suffer from persistent idiopathic facial pain can be referred to DHC only by other neurologists. All patients with TN or facial pain were examined by 3.0 Tesla magnetic resonance imaging (MRI) with a special protocol focusing on the facial structures, brain, the trigeminal nerve and neurovascular contact.
Second version and third beta version of the diagnostic criteria for classical trigeminal neuralgia of the International Classification of Headache Disorders (ICHD).

Methods
We consecutively included all patients seen at the DHC at the Department of Neurology, Glostrup Hospital, Denmark, with a diagnosis of TN or persistent idiopathic facial pain from April 2012 to November 2013. Exclusion criteria were communication barriers, painful posttraumatic trigeminal neuropathy and symptomatic TN. The number of patients in the inclusion period determined the sample size. In previous papers we reported the clinical characteristics in TN (submitted) and compared TN patients with and without concomitant persistent facial pain (5) using the same method of data collection.
Extensive psychophysical data by Maier et al. (6) and clinical experience demonstrated that some TN patients have sensory abnormalities and that in some patients this is detectable at a bedside neurological examination. We therefore used a modified version of the ICHD-2 diagnostic criteria as inclusion criteria in the current study allowing sensory abnormalities detected at clinical neurological examination in TN as well as in persistent idiopathic facial pain. However, such patients were diagnosed and included only if the other diagnostic criteria were fulfilled and if complete clinical history, neurological and physical examination and a 3.0 Tesla MRI did not raise any suspicion of another causative disease such as painful posttraumatic trigeminal neuropathy or symptomatic TN.
Several categorical and quantitative variables were systematically collected using semi-structured clinical interviews. The semi-structured interviews were performed by senior neurologists working at DHC and carefully trained in headache diagnosis. The interview is shown as supplementary material. The methodology has been described in more detail previously (submitted).
Definitions of specific terms
We distinguished between two types of pain: paroxysmal pain lasting from a split second to two minutes and described by patients as superficial, intense, lancinating, stabbing, ice pick-like or electrical lightning. We use the term “paroxysmal pain” for this type of pain. The other category of pain ranged from two minutes up to being constantly present and was described by patients as deep, toothache-like, aching, nagging, boring or dull. This type of pain is termed “concomitant persistent pain” according to the terminology of ICHD-3 beta.
If the paroxysmal pain did not only involve the innervation area of the trigeminal nerve, but also affected the scalp or neck, this was characterized as “not anatomically confined to V1–V3.”
Sensory abnormalities were recorded by a bedside clinical neurological examination. We defined that potential neurological deficits should be disregarded in patients who had undergone prior surgery because sensory abnormalities on the one hand could be a complication of surgical intervention and on the other hand could possibly be normalized as a result of surgery (7).
Definitions of specific subcriteria
“Paroxysms lasting from a fraction of a second up to two minutes” (1,4) was defined as pain paroxysms lasting less than two minutes but occurrence of longer lasting paroxysms was allowed. “(…) [A]ffecting one or more divisions of the trigeminal nerve” (4) was defined as pain that must involve one or more divisions of the trigeminal nerve but in addition to that may radiate beyond the innervation area of the trigeminal nerve. “(…) [U]nilateral facial pain” (1) was defined as pain affecting only one side of the face. In cases of bilateral symptoms affecting alternating sides it was required that the pain in an individual attack did not cross the midline. “(…) [N]o radiation beyond the trigeminal distribution” (1) was defined as strictly no radiation beyond the trigeminal distribution. “Intense” (4) and “severe intensity” (1) were defined as pain intensity ≥7 measured by the Verbal Numerical Rating Scale (VNRS).” Electric shock-like, shooting, stabbing or sharp in quality” (1) and “superficial” (4) were considered as a whole under the category of stabbing pain. “Precipitated from trigger areas or by trigger factors” (4) was defined as “Precipitated by innocuous stimuli to the affected side of the face” (1). “Attacks are stereotyped in the individual patient” (4) was defined as unilateral pain affecting only one side of the face. In cases of bilateral symptoms affecting alternating sides it was required that the pain in an individual attack did not cross the midline. “No clinically evident neurological deficit” (1,4) was defined as strictly no neurological abnormalities at bedside neurological examination, especially no clinically evident sensory abnormalities. “Not attributed to another disorder” (4) was defined as “not better accounted for by another ICHD3 diagnosis” (1).
Testing diagnostic criteria
To test the sensitivity of ICHD-2 and -3 beta, we looked at the extent to which the clinical characteristics in our more broadly defined TN patients satisfied the diagnostic criteria. Specificity was evaluated by the accuracy of the diagnostic criteria in excluding patients with persistent idiopathic facial pain. When field-testing the diagnostic criteria for TN, we considered the patients diagnosed with TN at our center as the “true positives” and patients diagnosed with persistent idiopathic facial pain as “true negatives.”
Patients, regardless of diagnosis, who had both paroxysmal pain and concomitant persistent pain were evaluated only according to the paroxysmal pain. Did the paroxysmal pain for example last less than two minutes, was it intense and possible to trigger, etc.? In patients with no current paroxysmal pain we evaluated the criteria for the characteristics of the concomitant persistent pain (i.e. either TN patients with previous paroxysmal pain or patients with persistent idiopathic facial pain).
Proportion of patients with the clinical characteristic listed in the diagnostic criteria of ICHD-2 and ICHD-3 beta and sensitivity and specificity of the individual criteria.

Values represent numbers of patients (%) unless otherwise indicated. N = 206 in classical trigeminal neuralgia (TN) and n = 37 in persistent idiopathic facial pain. ICHD-2 and - beta3: second version and third beta version of the International Classification of Headache Disorders; CI: confidence interval for the mean; NA: not applicable.
All TN patients had experienced paroxysms lasting less than two minutes but 14 (7%) patients had in addition experienced longer-lasting paroxysms.
Patients who had undergone prior TN surgery are not included in this analysis. N = 160 in TN and n = 34 in idiopathic persistent facial pain.
One out of two: intense, sharp, superficial or stabbing and/or precipitated from trigger areas or by trigger factors.
Three out of four: recurring paroxysmal attacks lasting from a fraction of a second to two minutes and/or severe intensity and/or electric shocklike, shooting, stabbing or sharp in quality and/or precipitated by innocuous stimuli to the affected side of the face.
No available data.
Statistics
Continuous data such as age and ranked data such as pain score by VNRS were summarized by descriptive statistics. The two-sample t-test was used for comparing independent groups. Categorical variables are presented with frequency distributions (N, %) and with exact confidence limits and no decimals. The chi square test and Fisher’s test were used as appropriate to assess associations of categorical variables. If more than 5% of the data for an individual patient were missing, the patient was excluded from the analyses. Missing data from included patients were considered missing at random. Sensitivity was calculated as the true-positive rate divided by the true-positive rate plus the false-negative rate. Specificity was calculated as the true-negative rate divided by the true-negative rate plus the false-positive rate. Sensitivity and specificity are reported with one decimal. The positive likelihood ratio (LR+) was calculated as (sensitivity/(1-specificity)) and the negative likelihood ratio (LR−) was calculated as (1-sensitivity)/specificity)). We calculated the kappa-values of agreement between the diagnostic criteria. P values for a significant difference between sensitivities and specificities were analyzed by McNemars test for paired proportions (8). All p values are reported as two tailed with a level of significance of 5%. Analyses were carried out using SAS 9.3 (SAS Institute Inc, Cary, NC, USA) except McNemars test, which was analyzed using GraphPad (GraphPad Software Inc, La Jolla, CA, USA).
Results
A total of 3869 patients were seen at DHC in the inclusion period. Of these 249 patients had TN or possible TN. Thirty-six TN patients were excluded from the current study because of missing data in the semi-structured interviews and two patients were excluded for communication problems (autism and dementia). Five patients were excluded because of a diagnosis of “possible TN” that could not be clarified at the end of the inclusion period. Finally, 206 TN patients were included in the current study. In previous papers we have reported the clinical characteristics of a subset of the included patients (5) (submitted).
Eighty-nine patients had facial pain other than TN at initial referral. Seventeen patients were excluded because of missing data and three patients were excluded for “possible atypical facial pain” that could not be further clarified at the end of the inclusion period. Patients with painful posttraumatic neuropathic trigeminal pain were excluded (n = 23). After careful specialist consideration, nine patients were excluded as their diagnosis was changed to cluster headache (n = 1), odontogenic pain (n = 2), migraine (n = 1) and diagnostically unresolved headache (n = 5), leaving 37 patients diagnosed with persistent idiopathic facial pain to be included. Figure 1 outlines the flow of the patients in the DHC in the inclusion period.
Flowchart of patients and diagnoses at Danish Headache Center (DHC) in the inclusion period.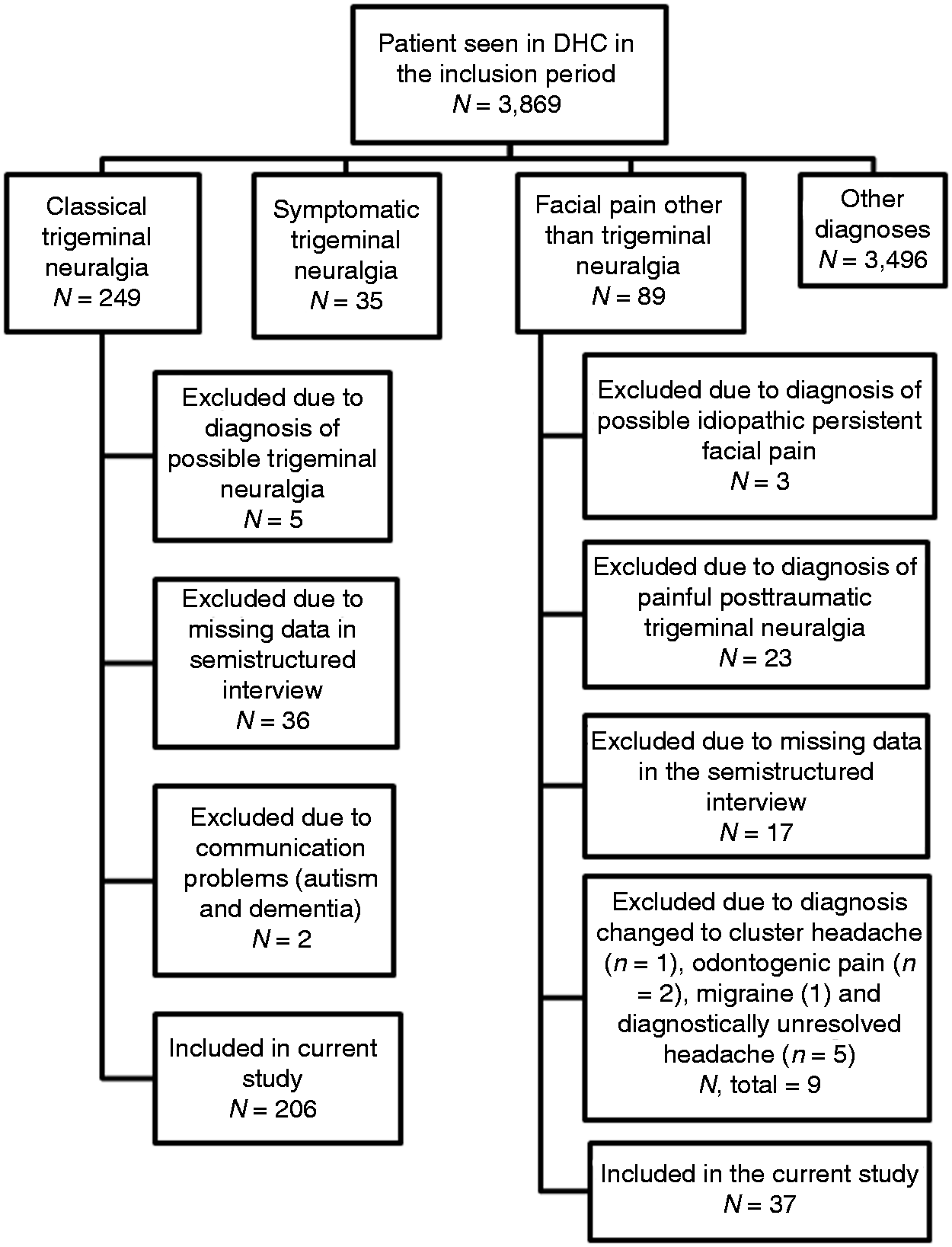
Demographics.

Values represent numbers of patients (%) unless otherwise indicated. N = 206 in trigeminal neuralgia (TN) neuralgia and n = 37 in persistent idiopathic facial pain. CI: confidence interval for the mean.
Sensitivity and specificity of diagnostic criteria.

N = 206 in trigeminal neuralgia (TN) and n = 37 in persistent idiopathic facial pain.
ICHD-2 and -beta3: second version and third beta version of the International Classification of Headache Disorders.
If sensitivity is 100% the diagnostic test is positive in all subjects with the disease in question, e.g. all classical trigeminal neuralgia (TN) patients fulfil the TN diagnostic criteria. Specificity of 100% indicates that the diagnostic test is negative in all subjects without the disease in question, e.g. no patients with persistent idiopathic facial pain fulfil the TN diagnostic criteria. Positive and negative likelihood ratios (LR+ and LR−) indicate the overall performance of the diagnostic test as they are based both on sensitivity and specificity. LR+ of 5–10 indicates moderate increase and LR+ >10 indicates large and often conclusive increase in the likelihood of disease, e.g. if the test is positive, it is extremely likely that the disease is present. Conversely, LR− of 0.2–0.5 indicates a small decrease, 0.1–0.2 indicates a moderate decrease and <0.1 indicates a large and often conclusive decrease in the likelihood of disease in case of a negative test result, e.g. if the test is negative, it is extremely unlikely that the disease is present. (Source: Office of Medical Education Research and Development, University of Michigan).
Proposed modified ICHD-3 diagnostic criteria in trigeminal neuralgia.

In some patients there may be longer attacks present but for this criterion to be fulfilled the majority of the attacks should last less than two minutes. Some of the attacks may be perceived by the patient as longer attacks because of a series of attacks lasting a split second each.
Severe intensity is defined as ≥7 (0–10 visual analog scale (VAS) or verbal numerical rating scale (VNRS)) or described by the patient as severe.
A neurovascular contact in the prepontine segment of the trigeminal nerve is not considered a structural pathology. ICHD-3 beta: third beta version of the International Classification of Headache Disorders.
Table 2 outlines the prevalence of patients fulfilling each diagnostic criterion. Figure 2 outlines how many TN patients satisfied, respectively, the ICHD-2, ICHD-3 beta and the proposed modified version of ICHD-3 beta (Table 5). One hundred and fifty-three (74.3%) TN patients were correctly diagnosed by all three versions of the diagnostic criteria (Figure 2). The proposed modified ICHD-3 criteria further diagnosed 45 (21.8%) TN patients correctly. These patients did not satisfy criterion D of ICHD-2 and ICHD-3 beta because of presence of sensory abnormalities at clinical examination but did satisfy all other criteria of ICHD-2 and ICHD-3 beta. Forty of these patients had been or were currently treated with sodium channel blockers, of whom 39 (98%) had a positive response to treatment. For comparison, out of the 28 (75.7%) patients with persistent idiopathic facial pain who did not fulfill any of the TN diagnostic criteria, half (14) had tried sodium channel blockers but only two (14%) out of these 14 patients had a response.
Percentage of patients included in the current study diagnosed with classical trigeminal neuralgia (TN) and persistent idiopathic facial pain (PIFP) who satisfy the TN diagnostic criteria of the International Classification of Headache Disorders, second edition (ICHD-2), third edition beta (ICHD-3 beta) and the proposed modified criteria. The majority of TN patients (74.3%) fulfilled all three versions of diagnostic criteria and the majority of PIFP patients (75.7%) did not fulfil any of the three versions of the diagnostic criteria. TN, n = 206 and PIFP, n = 37. “0” indicates neither TN nor PIFP patients. Cohen’s kappa-value of agreement between ICHD-2 and ICHD-3 beta was 0.93, between ICHD-2 and the modified version of ICHD-3 beta was 0.38 and between ICHD-3 beta and the modified version of ICHD-3 beta was 0.50.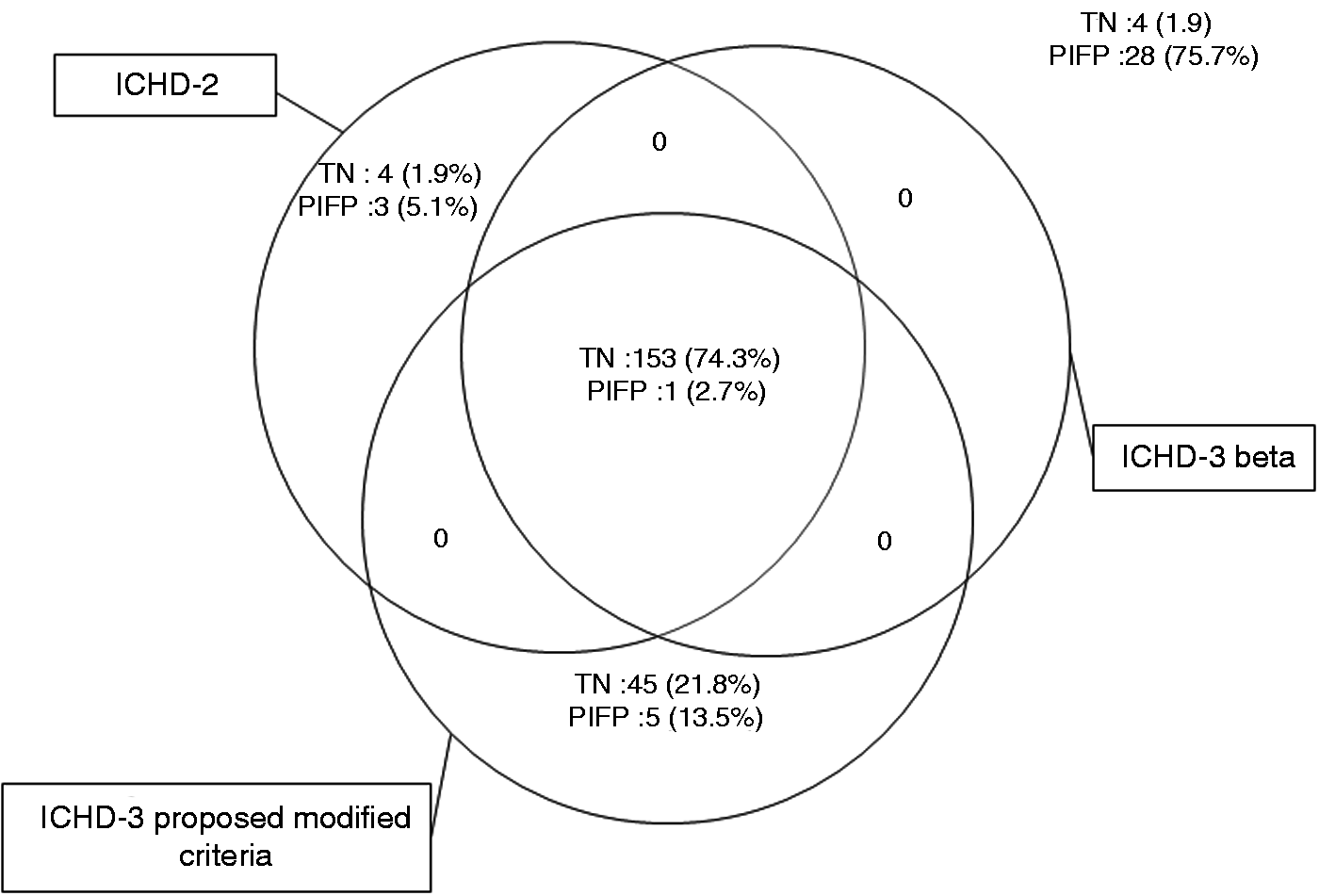
Four TN patients did not fulfill ICHD-3 beta or the modified version of ICHD-3 but did fulfill ICHD-2. The reason for non-fulfillment was in three patients pain radiating outside the trigeminal territory and in two there was neither intense nor triggered pain. Four other patients diagnosed with TN according to the inclusion criteria did not fulfill either ICHD-2, ICHD-3 beta or the modified version of ICHD-3 because one had neither intense nor triggered pain and three had radiating pain outside the distribution of the trigeminal nerve. The four patients all had sensory abnormalities at clinical examination.
Figure 2 outlines how many patients with persistent idiopathic facial pain satisfied the three sets of ICHD-criteria. There was only one (2.4%) patient with persistent idiopathic facial pain who was falsely diagnosed with TN by all three sets of diagnostic criteria. This patient did have short-lasting stabbing pain confined to V2 but the most dominant type of pain was the concomitant persistent pain that involved all three trigeminal branches and in addition radiated to the occipital area and was accompanied by burning paresthesias in the face. There were comorbidities of tension-type headache and depression. Five (13.5%) further patients with persistent idiopathic facial pain were falsely diagnosed with TN by the modified version of ICHD-3 beta. The five patients all had sensory abnormalities. All of these patients had experienced short-lasting stabbing pain but only to a minor degree while the concomitant persistent pain component was by far the most dominant type of pain. In three patients there were no trigger factors.
Discussion
The diagnostic criteria for classical TN in ICHD-3 beta are not significantly more or less sensitive or specific than ICHD-2 criteria. Both ICHD-2 and ICHD-3 beta have a relatively low sensitivity. A high sensitivity is important in clinical diagnosis (9). The authors therefore propose to allow for sensory abnormalities at clinical neurological examination if MRI and patient history do not demonstrate structural, systemic or traumatic causes of facial pain. This yielded a higher sensitivity than ICHD-2 and -3 beta and improvement of LR− (Table 4) indicating that when applying the proposed modified criteria to a group of patients presenting with facial pain, patients who do not fulfill the diagnostic criteria are much more likely not to suffer from TN. The proposed modified criteria only moderately reduced specificity. As the structure of ICHD-3 beta is also used in the International Classification of Diseases, 11th edition beta version (ICD 11 beta), our field testing and proposed criteria are also relevant to the forthcoming ICD 11.
Sensory abnormalities in TN
The monothetic criterion D of both ICHD-2 and -3 beta, which excludes all patients with sensory abnormalities at clinical neurological examination, was largely responsible for the low sensitivity of both sets of criteria because they exclude all patients with sensory abnormalities. A prior study reported high sensitivity of the diagnostic criteria of ICHD-2 in TN (10) but it did not report sensory abnormalities at clinical examination. The authors did, however, propose an amendment of “probable TN” for which the criterion of “no sensory abnormalities” was removed.
Several studies discussed sensory abnormalities in TN detected at bedside examination (10–13). Studies using quantitative sensory testing (QST) (6,7,14–16) reported a high prevalence of QST abnormalities in TN. We described the sensory abnormalities at clinical neurological examination in TN in detail in a previous paper (submitted). Patients with and without sensory abnormalities did not differ regarding classical characteristics of TN such as anatomical localization of pain, trigger factors, periods of remissions or response to sodium channel blockers. We concluded that, if the medical history and clinical and laboratory examinations do not raise suspicion of another diagnosis, the patient should not be excluded from the diagnosis of TN solely on the basis of sensory abnormalities. This would ensure that these patients are offered the correct and optimal pharmacological and surgical treatment.
Changes in the diagnostic criteria
In the recent ICHD-3 beta criteria there are major changes as the polythetic criterion B in ICHD-2 was expanded. According to our study, this change considerably improved specificity. Two monothetic criteria in ICHD-2 were abandoned; criterion A in ICHD-2 stating that the pain should last less than two minutes was incorporated into the polythetic criterion C in ICHD-3 beta. We defined criterion A in ICHD-2 as pain paroxysms usually lasting less than two minutes but occurrence of longer lasting paroxysms was allowed. This definition was in accordance with the comments in ICHD-3 beta (1). All of our patients had experienced pain lasting from a split second up to two minutes but some patients also had longer-lasting pain in addition. Thus longer-lasting pain should not mean failure to meet the criterion if the patient also had attacks lasting less than two minutes. This is added as a comment in the proposed modified criteria.
Criterion C from ICHD-2 stated that the pain must be stereotype. We consider this criterion poor because it is neither possible to measure reliably nor specific as it is not clarified whether “stereotype” refers to strictly unilateral pain, strictly the same intensity of attacks, strictly the same anatomical distribution of pain paroxysms or strictly always the same character of pain. We therefore support that this criterion was abandoned in ICHD-3 beta (1).
The new monothetic diagnostic criterion of “… no radiation beyond the trigeminal distribution” was added in ICHD-3 beta. Very few TN patients in our study had pain radiating outside the territory of the trigeminal nerve, but sensory nerves may exhibit considerable variation. Trigeminal branches may therefore in rare cases extend beyond their usual domains. As removing this criterion caused the overall specificity to drop considerably, we suggest keeping the criterion even though it did exclude a few true TN patients.
Using diagnostic criteria in low- and high-prevalence settings
The present authors propose modified criteria of ICHD-3 beta that are based on patient history and MRI and have been validated in an actual clinical setting rather than being based on expert opinion.
The proposed modified ICHD-3 criteria had a much higher sensitivity than ICHD-2 and -3 beta, ensuring that almost all patients diagnosed with TN by experts were correctly diagnosed by the diagnostic criteria, but the specificity was slightly lowered. A high sensitivity is, however, crucial (9) to the diagnostic criteria of TN as it is an extremely painful disease, which often can be effectively treated. Moreover, the purpose of the diagnostic criteria is to identify all patients suffering from TN in low- as well as high-prevalence clinical settings. Identifying TN patients will allow them to be referred from the primary sector to specialist evaluation. Specialist evaluation is not only based on the diagnostic criteria but is a complex diagnostic process in which data from the history and physical examination as well as clinical expertise, therapeutic trials and neuroimaging are assimilated to fortify the diagnosis.
Methodological and statistical considerations
The strengths of the current study are that the clinical characteristics were collected in a systematic, standardized and prospective way. Furthermore the diagnosis was made by neurologists specialized in headache and facial pain and symptomatic TN was excluded by high-resolution MRI.
The study population is as representative as possible although some less-affected patients are cared for by practicing neurologists. It is unlikely that such patients would alter the present results but it would be worthwhile to reproduce the present study in a practice setting. Furthermore, it is a limitation that patients were included from only one center.
Conclusion
ICHD-2 and ICHD-3 beta lack sensitivity. We propose modified criteria with a higher sensitivity for inclusion in ICHD-3 and ICD 11.
Clinical implications
Field-testing of the recent beta version of the third edition of the International Classification of Headache Disorders (ICHD-3 beta) diagnostic criteria for classical trigeminal neuralgia (TN) showed no significant difference in sensitivity or specificity compared to ICHD-2. A high prevalence of sensory abnormalities in TN accounted for a relatively low sensitivity of both sets of diagnostic criteria (74.3% and 76.2%). By applying a modified version of the ICHD-3 beta, it was possible to increase the sensitivity to 96.1% and maintaining a high specificity of 83.8%. A high sensitivity should be considered more important than specificity because it ensures that most patients get adequate treatment. The modified criteria are recommended for inclusion in the future ICHD-3 and International Classification of Diseases, 11th edition (ICD 11).
Ethics and institutional review board approval
It was confirmed by the Danish National Committee on Health Research Ethics ID number H-1-2012-093 that this project did not need ethical approval or patients’ informed consent, as it is observational, noninterventional and incorporated in the usual clinical daily work. The study protocol was not registered at ClinicalTrial.gov.
Footnotes
Funding
This work was supported in part by the 2010 Capital Region of Denmark Global Excellence in Health prize to DHC. The work was also supported by the Lundbeck Foundation (grant number R118-A11531) and the Danish patient society Trigeminus Foreningen. LB is principal investigator for Convergence study 1014802/202 and has received research grants from Convergence Pharmaceuticals. The funding sources had no role in the study.
Conflict of interest
None declared.