
Abstract
Introduction
Persistent idiopathic facial pain (PIFP) is a poorly understood chronic orofacial pain disorder and a differential diagnosis to trigeminal neuralgia. To address the lack of systematic studies in PIFP we here report clinical characteristics and neuroimaging findings in PIFP.
Methods
Data collection was prospective and standardized in consecutive PIFP patients. All patients underwent 3.0 MRI.
Results
In a cohort of 53 PIFP patients, the average age of onset was 44.1 years. PIFP was found in more women 40 (75%) than men 13 (25%), p < 0.001. There was a high prevalence of bilateral pain 7 (13%), hypoesthesia 23 (48%), depression 16 (30%) and other chronic pain conditions 17 (32%) and a low prevalence of stabbing pain 21 (40%), touch-evoked pain 14 (26%) and remission periods 10 (19%). The odds ratio between neurovascular contact and the painful side was 1.4 (95% Cl 0.4–4.4, p = 0.565) and the odds ratio between neurovascular contact with displacement of the trigeminal nerve and the painful side was 0.2 (95% Cl 0.0–2.1, p = 0.195).
Conclusion
PIFP is separated from trigeminal neuralgia both with respect to the clinical characteristics and neuroimaging findings, as NVC was not associated to PIFP.
Keywords
Introduction
Persistent idiopathic facial pain (PIFP), formerly termed atypical facial pain (1), is a diagnostic entity that describes chronic facial pain without evidence of structural or other specific causes of pain (2). The population prevalence of PIFP is estimated to be 0.03% (3) and it is more common in women (4). The pain is aching or dull and poorly localized (1).
The taxonomy of PIFP and related disorders such as trigeminal neuralgia, temporomandibular joint disorder, burning mouth syndrome and atypical odontalgia has been much debated due to lack of knowledge of the etiological and pathophysiological mechanisms (5–7). Several authors have indicated that PIFP is closely associated with psychiatric disorders (7–9). Burchiel proposed that the term atypical facial pain should be reserved only for patients with evidence of a somatoform pain disorder, and in facial pain patients without evidence of a somatoform pain disorder the diagnosis of classical trigeminal neuralgia (TN) should be considered instead (9,10). In his proposed classification system, TN was divided into “Type 1” with more than 50% paroxysmal pain and “Type 2 TN “with more than 50% constant pain. With this proposed classification system the proportion of patients with idiopathic constant facial pain and no psychiatric or psychological illness, which would most likely be classified as PIFP according to ICHD-2 and −3 beta, would have to be classified as “Type 2 TN”. The current study challenges such proposed classification of PIFP.
Several studies have documented that a severe neurovascular contact (NVC), with displacement or atrophy of the trigeminal nerve due to a blood vessel, is important to TN etiology (11,12). There is, however, a scarcity of neuroimaging studies of PIFP. An association with NVC would favor that a proportion of PIFP patients actually have “Type 2 TN”. Currently, invasive neurosurgical procedures such as microvascular decompression (MVD), which carries a risk of stroke and cranial nerve damage, are widely offered to patients classified as having “Type 2 TN” and the long term outcome is worse compared to “Type 1 TN” (13–15). If TN and PIFP have different etiological and pathophysiological mechanisms, MVD should generally not be offered to PIFP patients, and the two disorders should not be classified according to evidence of a somatoform pain disorder or not.
What the current paper contributes to current literature
This is the first prospective systematic study using 3.0 Tesla MRI reporting the clinical characteristics and neuroanatomical findings in PIFP. We demonstrate that PIFP is a distinct diagnostic category, which is separated from TN both with respect to the clinical characteristics and neuroanatomical abnormalities.
Methods
The methodology of the data collection and the MRI protocol was similar to that used for our TN patients and has previously been described in detail (12,16). We included all patients seen at the Danish Headache Centre (DHC) with a diagnosis of PIFP from April 2012 to December 2014. Exclusion criteria were communication barriers. The number of patients in the inclusion period determined the sample size.
DHC is a tertiary neurological treatment centre for headache and facial pain that receives patients from all parts of Denmark. Patients suspected of having PIFP can be referred directly from general practitioners, other neurologists or hospital departments. Diagnosis in the clinic was based on the International Criteria of Headache Disorders (ICHD-2) (17) (Supplementary Appendix A). For the purpose of the current study we used a modified version of the ICHD-2 to allow for sensory abnormalities in line with our proposed TN diagnostic criteria (18). This was allowed as previous psychophysical studies (19) reported sensory abnormalities in PIFP patients at quantitative sensory testing. In case of sensory abnormalities at clinical examination, we diagnosed PIFP if the other diagnostic criteria were fulfilled and clinical history, physical and neurological examination and a 3.0 Tesla MRI did not raise suspicion of another cause of pain.
In the ICHD-3 beta diagnostic criteria it is stated that “a continuum seems to exist from PIFP induced by insignificant trauma to painful posttraumatic trigeminal neuropathy caused obviously by significant insult to the peripheral nerve” (1). We agree with these considerations and find that evaluation of whether the preceding trauma actually caused painful posttraumatic trigeminal neuropathy or not is difficult. Therefore, in order to obtain a cohort as homogenous as possible, we excluded patients with any kind of trauma, including invasive dental treatment such as root canal treatment or tooth extraction, relevant to the painful region preceding the onset of pain by six months or less. Thus, the current cohort consists of patients with purely idiopathic facial pain.
Several categorical and quantitative variables were systematically collected using a purpose-built semi-structured clinical interview (Supplementary Appendix B), which was filled out by trained medical doctors working at DHC. We distinguished between two types of pain: Paroxysmal pain lasting from a split second to two minutes and described by patients as superficial, stabbing, or electrical lightning; and dull, nagging, aching pain lasting more than two minutes up to being constantly present. To assess pain intensity, we used the verbal numerical rating scale (VNRS) which ranges from 0, “no pain at all” to 10, “worst possible pain”. The location of pain was described according to the trigeminal branch involved. In patients where the facial pain was not restricted to the trigeminal territory, i.e. it crossed the midline of the face, or also involved the posterior part of the scalp, the angle of the jaw or the neck, the pain location was defined as “not anatomically distributed”.
Remission periods were defined as pain free periods lasting at least a month without medication or with very low dosage of medication defined as carbamazepine 100 mg daily or corresponding doses of other drugs. It was regarded as a response to medication if a patient had experienced pain relief to some extent after taking a specific medication. The patients were interviewed about past or current comorbidities. Depression and anxiety were defined as whether the patient had in the past or was currently diagnosed with depression or anxiety by a medical doctor.
The clinical examination of sensory function consisted of routine neurological examination for touch with a cotton swab and pinprick with a pin in the three trigeminal branches. Patients with previous TN surgery were excluded from the analyses of sensory function, as MVD and percutaneous procedures for TN can cause sensory disturbances.
To explore the hypothesis that PIFP represents a distinct diagnostic category separate from TN, we compared PIFP patients with episodes of stabbing pain to PIFP patients with only constant pain with respect to classical features of TN; unilateral pain strictly in the trigeminal territory, touch-evoked pain, remission periods, response to sodium channel blockers and severe NVC. This approach was chosen because, presumably, patients with some element of stabbing pain are more likely to have been misdiagnosed with PIFP, even though they actually have TN with an atypical presentation.
MRI protocol and definitions
All patients underwent an MRI scan within two months after the semi-structured interview was obtained. All data were acquired on a 3.0 Tesla Philips Achieva imager (Philips Medical Systems, Best, the Netherlands) equipped with a 32 channel head coil with Multi Transmit parallel radiofrequency transmission. The following sequences were used: A sagittal T2 weighted Turbo Spin Echo sequence covering the whole brain; an axial thin section T2 weighted GRASE sequence encompassing the brainstem and posterior fossa; an axial thin section T2 weighted Turbo Spin Echo sequence covering the face; a 3D time of flight MR angiography (s3DI MC HR); and a 3D, high spatial resolution heavily T2-weighted sequence (3D Balanced Fast Field Echo), with multiplanar reconstructions of the cisternal part of the trigeminal nerve strongly parallel to the nerve in the axial and sagittal planes and perpendicular to the trigeminal nerve in the coronal plane.
The MRI scans were evaluated by the same experienced neuroradiologist (FW). NVC was defined as contact between a blood vessel and the trigeminal nerve without visible cerebrospinal fluid between the two structures. If the neuroradiologist was uncertain about whether there was a contact, it was considered as no NVC in the data analysis. NVC was evaluated for 1) degree of contact, 2) localisation and 3) type of blood vessel. The degree of contact was graded on a three-point scale as simple contact, displacement or atrophy. Displacement was defined as displacement or distortion of the trigeminal nerve at the site of an NVC. Atrophy was defined as reduced volume of the trigeminal nerve at the site of an NVC. “Severe NVC” was defined as an NVC with displacement or atrophy. NVC was classified as either at the root entry zone or peripheral. The root entry zone, i.e. the zone where peripheral myelination transitions to central myelination, was defined as the area from the site of entry of the trigeminal nerve into the pons to 7 mm peripherally along the nerve. “Peripheral NVC” was defined as NVC more than 7 mm from the site of entry of the trigeminal nerve into the pons. The NVC was also evaluated according to whether it involved one or more arteries or veins, or both. If there was more than one NVC, the one with the highest degree of contact was graded. If there were two NVCs with an equal degree of contact on the same side, we favored the one in the root entry zone.
Institutional review board approval
The Danish National Committee on Health Research Ethics ID number H-1-2012-093 confirmed that the project did not need ethical approval or patients’ informed consent, as it was observational. The data collection was approved by the Danish Data Protection Agency.
Statistical analyses
Continuous data such as age were summarized by descriptive statistics, and the two sample t-test was used for comparing independent groups. Categorical variables are presented with frequency distributions (N, %) and exact confidence limits. McNemar’s test for paired proportions was used to assess associations of paired categorical variables, and the chi square test and Fisher’s test were used as appropriate to assess associations of un-paired categorical variables. Univariate conditional logistic regression was used to estimate the odds ratio (OR) between an NVC and the painful side. Patients with bilateral symptoms were excluded from the analyses of MRI data, as it is not possible to employ a case-control design in bilateral cases.
If more than 5% of the clinical data from the semi-structured interview form were missing, the patient was excluded from the analyses. Missing data were considered missing at random. P-values are reported as two-tailed with a level of significance of 5%. Analyses were carried out using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
During the inclusion period, 118 patients with facial pain other than TN attended DHC. Of these, 40 had facial pain diagnoses other than PIFP. PIFP was suspected in eight patients, but the diagnosis was not clarified as they were still in the work-up process being evaluated for odontogenic or infectious causes of pain. In 17 patients, more than 5% of the semi-structured interview was missing. Finally, 53 PIFP patients were included in the study. The flowchart of the inclusion process is outlined in Figure 1.
Flowchart of the inclusion from April 2012 to November 2014.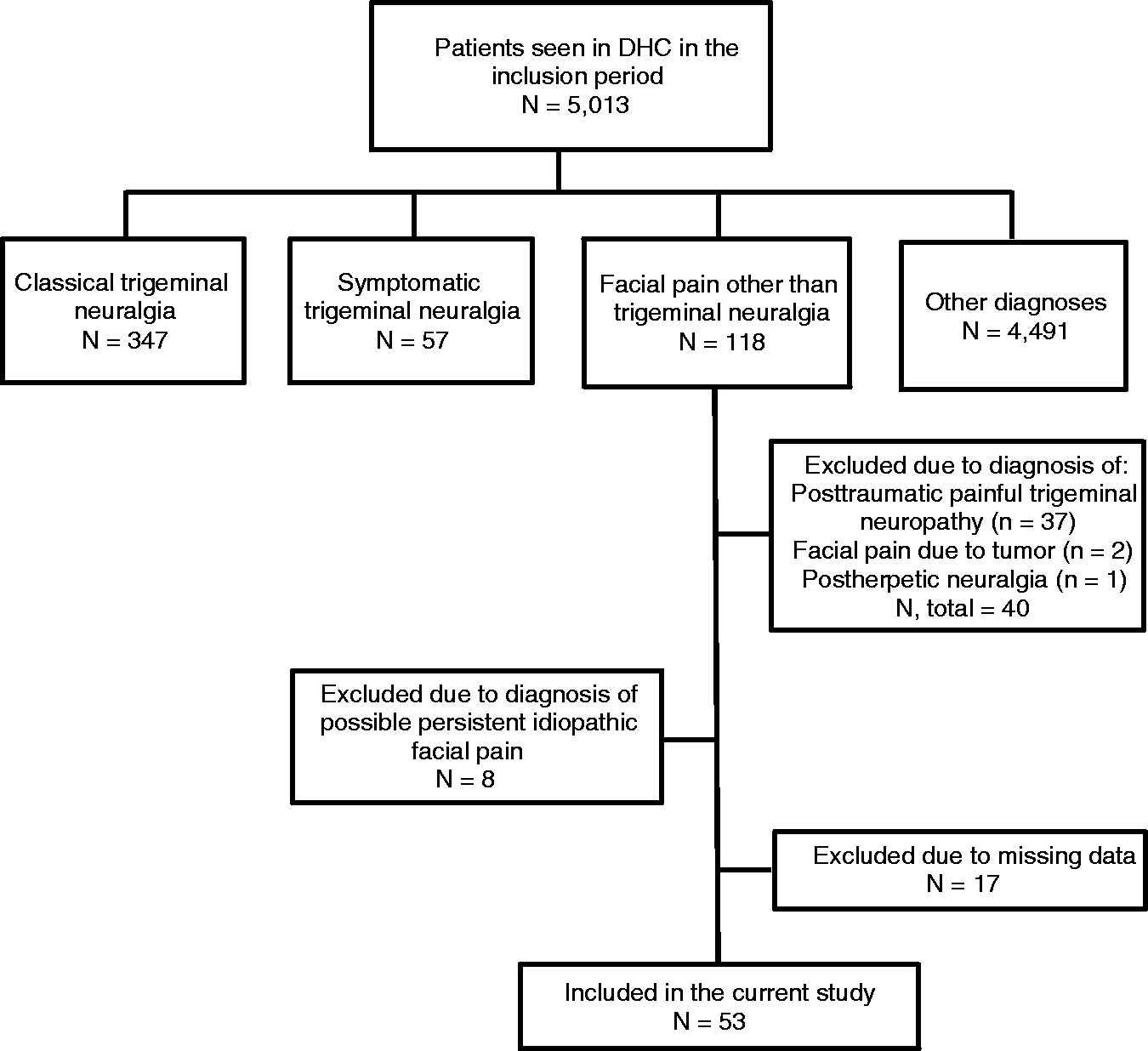
Clinical characteristics
Side and anatomical localisation of pain, stabbing pain, autonomic symptoms and sensory abnormalities. Values represent numbers of patients (%) unless otherwise indicated. N = 53.

Patients with previous TN surgery (n = 4) were excluded from the analyses of sensory abnormalities.
Of the 49 patients naïve to TN neurosurgery, 29 (59%) patients had sensory abnormalities, of which the most frequent finding was hypoesthesia (23 (48%)) (Table 1). In four of these patients, hypoesthesia was also found intraorally.
Twenty-one (40%) patients had episodes of stabbing pain paroxysms (Table 1). Of these, four (19%) fulfilled the TN diagnostic criteria of ICHD3 beta (Supplementary Appendix A). An expert in headache and facial pain carefully reviewed the diagnosis of the four patients who fulfilled the TN diagnostic criteria of ICHD3 beta. The expert did not find that the patients did suffer from TN, and that the disorder was better accounted for by the PIFP diagnosis. The main reasons for this were that none of these four patients had touch-evoked pain, and in all patients the stabbing pain component was not the main complaint.
The median intensity of the stabbing pain was 8, ranging from 2 to 10. There was a higher prevalence of unilateral pain confined to the trigeminal territory in patients with stabbing pain (18; 86%) compared to patients without stabbing pain (20; 63%) (p = 0.067). In three (14%) of the 21 patients with stabbing pain, the stabbing pain could be triggered by sensory stimuli. These three patients did not fulfil the IHCD-3 beta TN diagnostic criteria as the stabbing pain lasted more than two minutes and the pain was not of severe intensity. There was a lower prevalence of remission periods in patients with stabbing pain (one (5%) compared to nine (28%) (p = 0.034) patients without). Out of the patients who had tried sodium channel blockers (n = 27), there was a higher response rate in patients with stabbing pain (seven (64%) compared to four (36%) (p = 0.252) patients without), but the difference was insignificant. There was no difference in the prevalence of severe NVC between patients with episodes of stabbing pain (one (8%) compared to no (0%) (p = 0.406) patients without).
Headache and psychiatric comorbidity
Family history, headache, psychiatric disorders, other chronic pain and employment status. Values represent numbers of patients (%) unless otherwise indicated. N = 53.

Treatments
Twenty-seven (51%) patients had been or were treated with a sodium channel blocker such as carbamazepine or oxcarbazepine, and of these 11 (41%) were responders. Seventeen (32%) patients had been or were treated with amitriptyline and of these nine (53%) were responders. Sixteen (30%) had undergone invasive dental procedures such as tooth extraction or root canal treatment and 10 (19%) had been treated with antibiotics for sinusitis prior to correct diagnosis but after onset of facial pain. As a result of the exclusion criteria, facial pain patients with a history of facial trauma prior to pain onset, e.g. invasive dental procedures, were not included in the study. Three (6%) patients had undergone MVD of the trigeminal nerve. MVD was not efficacious in any of these patients.
Imaging
Prevalence and characteristics of neurovascular contacts. N = 32.

NA: not applicable.
Patients with bilateral symptoms (N = 7) were excluded from the analyses.
Root entry zone is defined as from the site of entry of the trigeminal nerve into the pons to maximum 7 mm peripherally along the nerve.
Either one or more arterial contacts or mixed contact with both arteries and veins.
Discussion
In a well-defined cohort of PIFP patients, we demonstrate that NVC is not involved in PIFP etiology and describe the clinical characteristics. These findings are important to the understanding of the etiological and pathophysiological mechanisms behind PIFP as well as for disease classification and clinical decision-making with respect to neurosurgical treatment options.
Clinical characteristics and comorbidities
We find a high prevalence of comorbid chronic pain and depression. This might be expected from a patient cohort recruited from a tertiary center. However, the estimates in out TN cohort for comorbid chronic pain (20%) and depression (15%) were much lower compared to the current PIFP cohort (16,20). Depression and comorbid pain suggest a predisposition to develop chronic orofacial pain, or may serve as aggravating factors for facial pain. Our data does not allow for further exploration into the causality between facial pain, other chronic pain and psychiatric illness, but supports that interdisciplinary treatment with both pain specialists and psychologists is relevant in PIFP.
Some of our findings are comparable to the findings of previous studies; others differ markedly. Comparison is hampered by the fact that all previous studies also included a proportion of patients (13–50%) where the pain was initiated by trauma (4,21–23), and only one series of papers describing the same cohort was prospective (23–25). In all previous PIFP studies, there is consistently a higher prevalence of women (68–89%) and the age of onset is also comparable to our findings (4,21,22,24,26). Remission periods lasting more than a month were reported in 10–23% (4,21,23). The prevalence of autonomic symptoms (0–30%) and of psychiatric disorders (6–79%) in PIFP vary greatly in previous studies (21,22,24–26), which probably reflects the different clinical settings and the different professional backgrounds of the authors.
Autonomic symptoms
Autonomic symptoms may pose a diagnostic challenge in differentiating the trigeminal autonomic cephalalgias and the idiopathic facial pain syndromes such as PIFP and TN. In particular, TN and short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) or cranial autonomic features (SUNA) can pose a challenge as both are characterized by paroxysmal short-lasting pain that can be either triggered or spontaneous (27). The dominant quality of pain in PIFP is, however, continuous aching pain, and although a proportion of the PIFP patients in the current cohort had autonomic symptoms, only one patient had pronounced autonomic symptoms, which is a hallmark feature of SUNCT/SUNA and other trigeminal autonomic cephalalgias (28).
Sensory disturbances
We report a high prevalence of hypoesthesia. Previous studies also reported and discussed sensory abnormalities in PIFP (19,22,25,29,30). One study using quantitative sensory testing did not find any sensory abnormalities in PIFP patients (31). Rather than actual nervous damage, our findings may reflect functional changes in the nervous system of central or peripheral adaptation to pain in the somatosensory system. Hence, loss of function (i.e. hypoesthesia) in PIFP could be due to functional downregulation of sensory input due to pain (32,33) as we have recently demonstrated in TN (34). Loss of function could also be caused by peripheral or central damage to the trigeminal sensory system.
Diagnosis
We report a high prevalence of episodes of stabbing pain in PIFP. Paroxysmal sharp pain in PIFP has also been recognized by others (1,2). In one study, 40% of patients assigned the pain quality descriptor “stabbing” to their pain (4), but in other studies stabbing pain was very rare (21,23). Stabbing pain is a hallmark feature of TN, but our results comparing PIFP patients with and without stabbing pain indicate that PIFP patients with and without stabbing pain do not represent distinct subgroups. Field-testing of the PIFP diagnostic criteria is beyond the scope of the current paper, but the findings are in line with a previous paper from our group with field-testing of the TN diagnostic criteria using PIFP patients as a control group, which showed a high specificity of the diagnostic criteria in TN in discriminating PIFP patients. Other studies using cluster analysis of the clinical characteristics and the McGill Pain Questionnaire also identified PIFP as clearly separate from TN (6,35).
In summary, we find several important clinical differences between PIFP and TN, as in PIFP there is a younger age of onset, an even greater preponderance of women, lack of side differences of pain, more frequent bilateral pain, less frequent remission periods, touch-evoked pain and response to sodium channel blockers, and more frequently comorbid pain, depression and sensory abnormalities (Figure 2).
Prevalence of neurovascular contact (NVC) in two facial pain disorders. For a graphical illustration of the differences in the prevalence of simple NVC and severe NVC (with displacement or atrophy), the data from the current paper on PIFP patients (n = 32) on the symptomatic (a) and asymptomatic side (b) are presented, with prospective data collected using a similar MRI protocol as in the current study and previously published (12) from patients with classical trigeminal neuralgia (n = 135) on the symptomatic (c) and asymptomatic (d) side.
Etiology and treatment options
The MRI results presented in this paper clearly demonstrate that there is no association between NVC and the symptomatic side in PIFP. This is in accordance with a previous 1.5 Tesla MRI study (36). The final proof that NVC is not the cause of PIFP would be that there was no efficacy from MVD. However, based on the poor outcome reported in PIFP patients who have undergone MVD (37), which is in accordance with our clinical experience, it would be unethical to conduct such a study. We therefore conclude that NVC is not important to PIFP etiology. Findings are comparable to previous studies of healthy subjects that also reported a high prevalence of NVC in general (88%), while a severe NVC was rare (38). Our finding of any type of contact in 78% of PIFP patients is also in line with our previously reported findings of 78% on the asymptomatic side in TN patients using the same methodology as in the present study (12). In contrast, in TN there is a strong association between the symptomatic side and a severe NVC (11,12), and we reported a prevalence of severe NVC in 53% of TN patients on the symptomatic side using the same methodology as in the present paper in contrast to the 3% found in PIFP patients in this study. Traditionally, invasive neurosurgery for TN such as MVD has not been proved effective or recommended for PIFP. However, some PIFP patients undergo the procedure anyway, as was the case in our cohort. Meanwhile, it is crucial that MVD is offered to the correct patients, as it involves a risk of complications such as death, brainstem hemorrhage and infarction (0.1% each), and damage to the trochlear, trigeminal, facial and vestibulocochlear nerves (0.9–1.6% each) (39). The results presented in this paper supports that MVD should not be offered to PIFP patients.
Strengths and limitations
The included patients represent a well-defined cohort, and were diagnosed by experts in headache and facial pain. In facial pain disorders there is rarely a definitive diagnostic test available, which is why diagnosis is based on expert evaluation and diagnostic criteria. This may pose a risk of circular reasoning. With respect to obtaining a history of previous or current psychiatric disorders, data was collected by the clinician asking the patient rather than by applying advanced validated diagnostic questionnaires. This pragmatic approach was applied as the study was based in daily clinical practice with limited time resources.
Data was collected systematically and prospectively. High quality MRI and an experienced evaluator are important in assessing the relations of the trigeminal nerve, but it is a limitation that the neuroradiologist was not blinded to diagnosis or to the symptomatic side. Presumably this would, however, increase the number of positive findings, which is why we had expected to find a higher prevalence of simple and severe NVC on the symptomatic side. The fact that our results tended to show the opposite indicates that observer bias was not a problem. The cohort is based in a tertiary medical centre. Thus, the findings may not be applicable to less affected patients who can be cared for in the primary sector. Finally, it is a single centre study and findings should be reproduced by other centres.
Conclusions
In this paper, we report the clinical characteristics in PIFP. Furthermore, we demonstrate that there is no association between NVC and PIFP. Findings support that PIFP is a clinically and etiologically separate entity from TN, and that MVD should not be a treatment option in PIFP.
Clinical implications
In persistent idiopathic facial pain (PIFP) there is a high prevalence of women. Contrary to trigeminal neuralgia, in PIFP there is a high prevalence of bilateral pain, hypoesthesia, depression and other chronic pain, and a low prevalence of stabbing pain, touch-evoked pain and remission periods. As opposed to trigeminal neuralgia, in PIFP there is no association between the painful side and the presence of or degree of compression from a neurovascular contact in the prepontine segment of the ipsilateral trigeminal nerve. As there is no association between PIFP and neurovascular contact, the procedure of microvascular decompression, traditionally offered to trigeminal neuralgia patients, should not be a treatment option in PIFP. Findings support that PIFP is a clinically and etiologically separate entity from trigeminal neuralgia.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: In 2010 the Capital Region of Denmark awarded the Global Excellence in Health prize to DHC, and a part of the prize has financed this study. The work was supported by the Lundbeck Foundation [grant number R118-A11531] and the Danish patient organization Trigeminus Foreningen. The funding sources had no role in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.