
Abstract
Objective: To estimate the lifetime prevalence of trigeminal neuralgia (TN) and persistent idiopathic facial pain (PIFP) in a population-based sample in Germany.
Methods: A total of 3336 responders of 6000 contacted inhabitants of the city of Essen in Germany were screened using a self-assessment questionnaire. 327 individuals, who reported recurrent facial pain and randomly selected 150 (5% of 3009) screening negative subjects, received a phone interview by one of six neurologists and if necessary a face-to-face examination. Those with suspected TN or PIFP following the phone interview underwent neurological examination by two neurologists who were unaware of the presumed diagnosis. A random group of 25 (10% of 247) phone interview negative subjects was examined face-to-face. All suspected cases of PIFP received otorhinolaryngological examination and diagnostic cranial magnetic resonance imaging (MRI). In TN patients the number of vessel-nerve contacts was determined by thin-slice cranial MRI.
Results: Lifetime prevalence of TN was estimated to be 0.3% [10 of 3336; 95% CI 0.1–0.5%], of PIFP 0.03% [1 of 3336; 95% CI < 0.08%]. Thin-slice cranial MRI detected five vessel-nerve contacts and no symptomatic lesions in the 10 TN patients.
Conclusions: This large population-based study revealed that TN and PIFP are rare facial pain disorders.
Keywords
Introduction
Trigeminal neuralgia (TN) is a unilateral painful disorder characterized by brief electric shock-like pains, abrupt in onset and termination, and limited to the distribution of one or more divisions of the trigeminal nerve. The International Headache Society (IHS) differentiates between classical trigeminal neuralgia, often caused by microvascular compression at the trigeminal root entry zone of the brainstem, and symptomatic trigeminal neuralgia, caused by a structural lesion other than vascular compression (1).
Persistent idiopathic facial pain (PIFP), previously termed atypical facial pain, is a persistent, dull, poorly localizable, facial pain without sensory or other neurological deficits, which cannot be attributed to a different disorder. Therefore investigations such as x-ray of face and jaws, cranial computer tomography (CT) or magnetic resonance imaging (MRI) are necessary to exclude any relevant abnormality (1).
The true prevalence of TN and PIFP is unknown, since both disorders are infrequent and therefore very rarely studied in population based studies. The present study aimed to estimate the life time prevalence of TN and PIFP and was embedded into the epidemiological survey of the German Headache Consortium (GHC study), which is a large population based survey on the prevalence of primary headache disorders in Germany.
Methods
The study was approved by the local ethics committee of the University of Duisburg-Essen. Informed written consent was obtained from all patients participating in the study.
Study sample and screening procedure
The initial GHC study sample included 18.000 people in three regions (city of Essen, a typical urban area, city of Muenster, a middle size town and the rural area of Sigmaringen) in Germany. Inclusion criteria during random sampling in 2001–2002 were: age 18–65 years and German citizenship (to ensure proper knowledge of the German language). The screening questionnaire asked for headache, facial pain and back pain (2,3). In 2003–2004, all study participants received the questionnaire via postal mail and, in case of non-response, a reminder 2 weeks later. Subjects, who did not respond were called and asked for a telephone interview performed by trained medical students. After eight unsuccessful calls, subjects were considered non-responders. Individuals who refused the interview either by postal response or by phone were also considered non-responders. Results on the prevalence of migraine, tension-type headache and medication overuse headache will be reported separately. In this study, we restricted the study sample to the city of Essen, as we had no opportunity to investigate people in Muenster and Sigmaringen personally.
Screening for TN and PIFP
The sample subset in the city of Essen (N = 6000) was screened for possible TN and PIFP using two screening questions: 1) “Have you ever had recurrent facial pain?” and 2) “Have you had facial pain last year?” In 2008–2009, all participants who answered “yes” to one of the two questions were called for a second detailed semi-structured interview which was performed by one of six neurologists who were trained for two to four years in the field of headache at the Department of Neurology, University of Duisburg-Essen (DM, MSY, MO, FP, MS, NH). All subjects with suspicion of TN or PIFP were invited for a face-to-face interview.
Screening negative cases
In 2009-2010, a randomly selected 5% of those study participants, who responded “no” to both screening questions, were interviewed by phone and if necessary invited for a face-to-face examination. In addition, a random sample of 10% of those study participants, who screened negative following the phone interview, was invited for a face-to-face examination as well.
Clinical examination and imaging
Neurological examination was standardized to minimize the between-examiner variability. Each subject was explored by two neurologists blindly to the suspected diagnosis and independent from one another. In case of discordance subjects were finally diagnosed by the most experienced neurologist (ZK). TN and PIFP were diagnosed according to the ICHD-2 criteria (1). In order to detect a vessel-nerve-contact or possible symptomatic focus, all cases diagnosed as TN underwent cranial MRI scans using the following sequences: time of flight angiography (TOF), fluid-attenuated inversion recovery (FLAIR), gradient echo (T2*), thin slice (2 mm) T2, and magnetization prepared rapid acquired gradient echo (MP-RAGE). Study participants with suspicion of PIFP received maxillofacial and otorhinolaryngological examination to identify symptomatic causes of the facial pain.
Statistics
All analyses were performed using SPSS 16.0 (SPSS Inc. Chicago, IL, USA). Crude prevalences of TN and PIFP were calculated in percentages (prevalence = screening positive cases/ all screened respondents x 100%), with 95% confidence intervals (CI) estimated as suggested previously (4):

Results
Study sample
In total, 3336 respondents in the city of Essen (mean age 45.0 ± 12.8 years, 53.7% women) were screened for facial pain. Of those, 327 people reported recurrent or persistent daily facial pain and 270 (82.6%) individuals were willing to further participate in the study (Figure 1).
Flow chart illustrating the screening procedure to detect possible individuals with trigeminal neuralgia (TN) and persistent idiopathic facial pain (PIFP).
Suspected TN and PIFP cases
Of 270 candidates for TN or PIFP, 16 were classified as possible TN and 7 as possible PIFP following the telephone interview.
Confirmed TN and PIFP cases
The diagnosis of TN was confirmed in ten cases, the diagnosis of PIFP in one case (Figure 1). Estimated life time prevalence of TN in the population-based sample was 0.3% (10 of 3336; 95% CI [0.1-0.5%]), the life time prevalence of PIFP was 0.03% (1 of 3336; 95% CI [<0.08%]). The concordance between the two neurologists who attended face-to-face the patients was 91.3%.
Clinical features of the trigeminal neuralgia patients
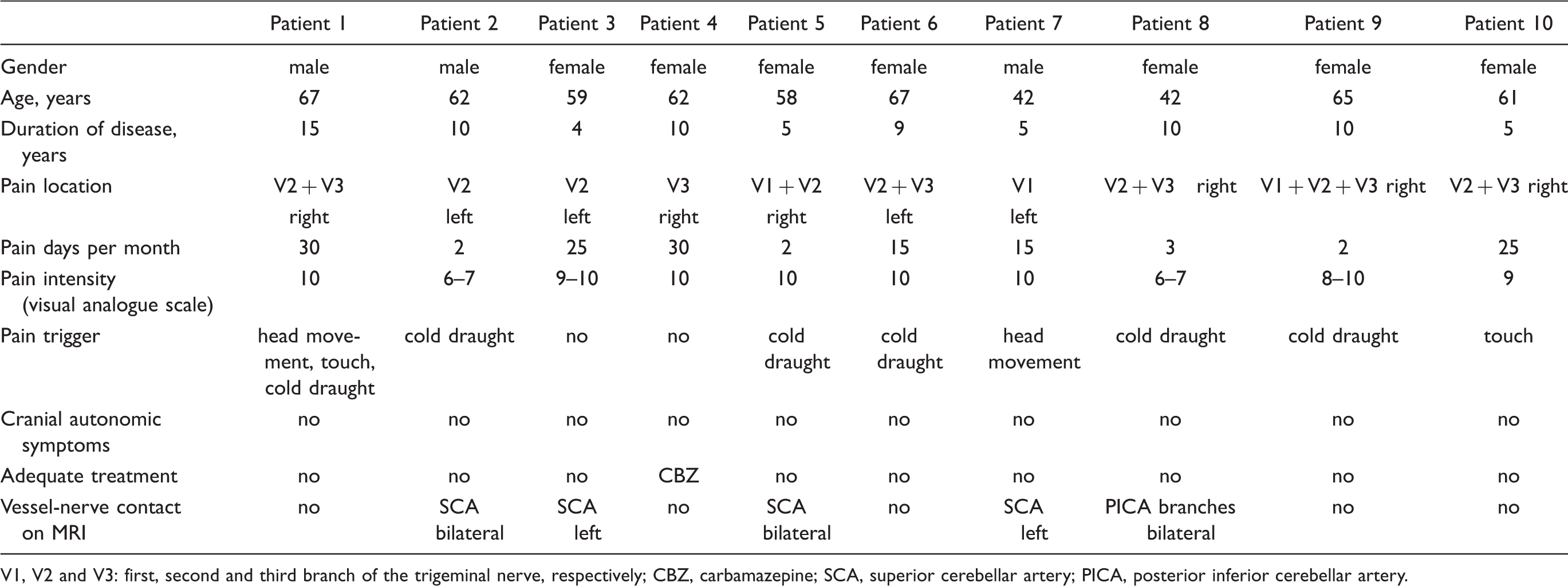
V1, V2 and V3: first, second and third branch of the trigeminal nerve, respectively; CBZ, carbamazepine; SCA, superior cerebellar artery; PICA, posterior inferior cerebellar artery.
MRI evaluation did not reveal causative lesions for TN in any of the studied patients. Vessel nerve contact was found in five of ten patients. In four patients the superior cerebellar artery (SCA) showed a contact to the trigeminal nerve root entry zone, in two of these patients on both sides, in two patients only on the symptomatic side. In one patient we found a contact of branches of the posterior inferior cerebellar artery (PICA) to the trigeminal nerve root entry zone on both, the symptomatic and the asymptomatic, side. In five patients, no vessel-nerve contact was found (Table 1).
One patient, a 65 year old woman was diagnosed with trigeminal neuropathy. The pain started 17 years ago. Currently she complained of stinging pain slowly rising from the cheek, radiating to the ear. The pain attacks occurred at approximately 20 days per month for about 3-5 hours and were triggered by mastication sometimes. Clinical examination revealed hypoesthesia and hypoalgesia in the second branch of the trigeminal nerve. Treatment with different anticonvulsants (e.g. carbamazepine, gabapentin, pregabalin) did not improve the pain. Currently, she uses opioids without significant pain relief, however. The patient was not willing to undergo cranial MRI and therefore was excluded from the prevalence analysis.
We identified one man with PIFP, who was 68 years old with disease duration of 10 years. He was misdiagnosed as chronic sinusitis and underwent functional endoscopic sinus surgery several times in the past years without clinical improvement. The facial pain occurred daily, and persisted for most of the day. It was confined to a limited area of the right jaw at onset and spread to the lower half of the face subsequently. He had no personal or family history of migraine. The neurological exam did not reveal any sensory deficits. X-ray of face and jaws as well as cranial MRI did not demonstrate any relevant abnormalities.
Unconfirmed cases
Out of the 270 individuals, who reported recurrent facial pain and agreed to participate in the study, 247 were rejected following the telephone interview, during which we recognized that the vast majority reported pain in the face meaning hemicranial pain, most prominent in the forehead. Based on the phone interview, probable diagnosis in 188 individuals was migraine, 39 had tension-type headache and 20 probably had both. Please note that these probable cases remained unconfirmed.
Six of 16 cases with suspected TN following the telephone interview were rejected after the clinical examination: five were diagnosed with migraine with concomitant facial pain and one with trigeminal neuropathy as described above.
Out of seven cases with possible PIFP four subjects were diagnosed with chronic sinusitis and two had temporo-mandibular dysfunction.
Screening negative cases
A random sample of 150 subjects (5% of 3009 screening negative cases (3336 minus 327) who denied having facial pain were interviewed by phone. Of those, 27 people reported having headache. All of them were examined personally. Migraine was diagnosed in 15 cases and tension-type headache in 12 cases. One subject reported to have pulsating pain in the mandibular region in the previous year, which was diagnosed as pulpitis and treated accordingly. She explained that she did not report it during the first interview because this painful event occurred once and was not recurrent. In addition 30 individuals without any suspicion of having headache or facial pain agreed to undergo a face-to-face neurological examination. No headache or facial pain disorder was diagnosed.
Another random sample of 25 subjects (10% of 247), who were not suspicious of TN or PIFP in the phone interview, were additionally examined face-to-face. 19 subjects suffered from migraine, in six of them tension-type headache was diagnosed. These diagnoses were already suspected in the phone interview and confirmed in the face-to-face examination. No facial pain disorder was diagnosed.
Discussion
We investigated 3336 subjects and identified ten cases with TN and one case with PIFP, corresponding to the prevalence rates of 0.3% [95% CI 0.1-0.5%] for TN and 0.03% [95% CI < 0.08%] for PIFP.
The prevalence estimation for TN and PIFP is difficult due to the rarity of these disorders. Therefore, we embedded the screening questions into the large scaled epidemiological survey of the German Headache Consortium (GHC). Intention was to include all possible TN or PIFP cases and thus used screening questions with maximal sensitivity neglecting specificity. This however, led to a high number of false positive cases, who were then filtered out by the telephone interviews. The main reason for misleading reports was the fact, that many people suffering from migraine or tension-type headache reported having facial pain, when in fact they meant hemicranial pain including frontal head pain. Hemicrania continua was considered among unconfirmed cases, but we did not find a person with a permanent and strictly unilateral headache with at least one cranial autonomic feature.
We think that the typical features of TN made it easy for headache experienced neurologists to differentiate between the different pain syndromes. The interview with a person with PIFP is more challenging and in this case as well as a general rule we applied that unclear patients should be invited for a clinical investigation. The final clinical diagnosis of TN or PIFP should be made following clinical examination. Therefore, all suspected cases were invited for personal examination to the hospital. Here, the clinical and imaging studies diagnosed 10 cases of TN and one of PIFP.
Literature regarding the prevalence of TN is scarce. Lifetime prevalence estimate of TN in Britain was based on information obtained from general practices and the British National Hospital for Neurology and Neurosurgery with a subsequent clinical re-evaluation of the suspected cases (5). Surprisingly, this report of MacDonald provides a lower prevalence (0.07%) compared to our result, although it is a hospital-based and practice-based survey and commonly prevalence rates tend to be higher in hospital-based surveys compared to population-based studies. In addition there was no age limitation in the study population and still lifetime prevalence was calculated lower.
A genuine population based study on the prevalence of TN was conducted in Norway, which similar to ours was embedded into a large headache survey (6). The age group was similarly limited to 18-65 years. The prevalence of TN in that study was 0.1%, which is three times lower than in ours. This difference could reflect the differences between the two countries or could be a consequence of a higher response rate in the Norwegian study. Penman indirectly calculated prevalence rates of TN making use of the proved association between TN and disseminated sclerosis (7). He utilized prevalence data for disseminated sclerosis, prevalence data for TN among sufferers from disseminated sclerosis and prevalence data for disseminated sclerosis among sufferers from TN, which were previously collected in hospitals and outpatient clinics. The age distribution of the underlying surveys is diverging. He calculated the prevalence of TN applying the formula a x c/a x b/c = b, where a, b and c are the respective prevalences of disseminated sclerosis, TN and combined cases (c being included in a and in b). Of course this calculation is subject to several kinds of inaccuracy, a fact which may partially explain the difference between our prevalence and Penman's prevalence (0.01% for men and 0.02% for women).
Several studies on the incidence of TN should be mentioned as well. Penman (1968) reported the incidence rates of 4.7/100,000/year (0.005%/year) in men and 7.1/100,000/year (0.007%/year) in women. Katusic et al. found an incidence of 4.3/100,000/year (0.004%/year) with 3.4/100,000/year (0.003%/year) for men and 5.9/100,000/year (0.006%/year) for women (8). Rozen reported an overall incidence of 2–5/100,000/year (0.002%-0.005%/year) for both genders (9).
The majority of the 10 TN patients in our study were women. The second branch (alone or together with the third) was most frequently affected as reported previously (8,10). In six patients, the right side was painful, in four patients the left side. This is in line with previous studies showing insignificant clustering on the right side probably due to raised stand of the right pyramid (11). In our cohort the patients were 58.8 ± 9.2 years old in average during actual examination with mean disease duration of 8.3 ± 3.5 years. None of them had cranial autonomic features like conjunctival injection or tearing, a fact that is important in the major differential diagnostic issue of short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache attacks with cranial autonomic features (SUNA) (12). The demographic features of our patients were comparable with previous reports (8,13). The one patient with PIFP described a typical continuous dull facial pain. As many other patients he also had a history of several otorhinolaryngological and dental surgery procedures.
Brain MRI scans were performed in all probable TN and PIFP cases and no symptomatic causes, e.g. a demyelinating lesion or a tumor, were detected. In TN patients, a vessel-nerve contact was found in five patients (50%) by thin-slice-MRI. In four patients the superior cerebellar artery and in one case branches of the posterior inferior cerebellar artery were the contacting vessels. In three patients a vessel-nerve contact was found on the asymptomatic side as well. These findings are in line with a previous study demonstrating aberrant vessel-nerve-contacts in approximately 27% of asymptomatic subjects (14). The symptomatic vessel-nerve contacts were found in 57% as in our study.
Some limitations of this study have to be discussed. The age of the screened population was limited to 18-65 years during initial random sampling in 2001-2002, so that the age range at the beginning of the screening for TN and PIFP in 2008 was 24-72 years. The overall response rate of the survey was 56%, which is comparable to other large scaled population based surveys in Western Europe and the US, but poses a possible selection bias. It is likely that young and old and disabled people do not respond. We cannot exclude an interest bias during the first screening phase that people with head or facial pain tend to participate more eagerly than healthy people. This could lead to overestimated prevalence of TN. A conservative calculation with the entire sample in the denominator (10 of 6000) would provide an estimate of 0.16%. We think therefore that the true prevalence of TN lies between 0.16% and 0.3%. It is of note, that the validity of the screening questionnaire was studied for headache and pain in general and for the three most frequent headache disorders, migraine, tension-type headache and cluster headache. Ideally the questionnaire should be tested for TN and PIFP as well, which is hardly possible, especially in a population based setting because of the rarity of these syndromes. We assumed that suffering from severe recurrent facial pain is a condition which can hardly be neglected, and therefore almost all individuals would recall this suffering. This hypothesis is supported by the fact that we did not find any false negative cases in the analysis of 5% of the subjects who screened negative in the mailed questionnaire and in the analysis of 10% of the subjects who screened negative in the telephone interview. Finally, it should be noticed that 57 individuals with facial pain were lost to follow-up before the neurological exam. In case any of them had TN or PIFP, the prevalence estimates might well be affected.
Several strengths of this study may account for the limitations. The studied population can be considered representative for the general population in Germany with reasonable approximation. The stepwise screening procedure including questionnaire, phone interview, clinical examination and imaging studies allowed precise diagnosis and adequate characterization of patients with TN and PIFP.
Consequently, we think that despite the above mentioned limitations, the presented study achieved its main goal to provide an estimate of TN and PIFP life-time prevalence in the general population in Germany.
Footnotes
Funding
This work was supported by the German Headache Consortium, the financial support was used for design and conduction of the study, especially for the data collection.