
Abstract
Background
The combination of vertigo, dizziness and balance disturbance with migraine is called vestibular migraine. Although it is estimated that up to 1% of the population suffers from this disease, it is still widely unknown and often underdiagnosed. Recently, the International Headache Society and the Báràny Society published the first joint document with mutually accepted diagnostic criteria for vestibular migraine.
Method
This review summarizes current knowledge on vestibular migraine with regard to epidemiology, clinical presentation, pathophysiology, differential diagnosis and therapeutic options.
Results
Approximately 30–50% of patients with migraine report vertigo, dizziness or balance disturbances with at least one migraine attack. Vestibular migraine often appears in a temporal delay to the first onset of migraine headache. In some patients the symptom of sudden onset disequilibrium was the main complaint and more worrisome than the accompanying migraine headache. The duration of attacks varies from a few seconds up to few days. The underlying pathophysiology of vestibular migraine is still widely unknown. As an important differential diagnosis, Ménière’s disease has to be considered and excluded.
Conclusion
As randomized controlled treatment trials are still missing in vestibular migraine, the therapeutic recommendations for vestibular migraine are currently based on the guidelines of migraine.
Introduction
Vertigo and headache are frequently reported symptoms in clinical neurology (1,2). About 30–50% of all patients with migraine describe vertigo or dizziness associated with their migraine at least occasionally (3,4). The link between migraine and vertigo was described for the first time by Aretaeus of Cappadocia in 131 BC, but systematic research of this association only started at the end of the 19th century (5). In 1873 Edward Liveing, a Victorian physician, described a link between migraine and dizziness in some of his patients (6). Since that time this phenomenon has been described with varying terminology in the literature, and has recently come more into the focus of clinical and scientific interest. Since 1990 the number of articles published on vertigo and headache in PubMed has doubled approximately every 5 years. The most common terms to describe the combination of both (migraine and vestibular symptoms) are vestibular migraine (7), migranous vertigo, migraine-associated vertigo, vertiginous migraine, migraine-associated balance disturbance and benign paroxysmal vertigo. The diversity of the nomenclature indicates that clear diagnostic criteria for vestibular migraine were lacking for a long time and diagnosis was complicated by the complexity and abundance of associated symptoms.
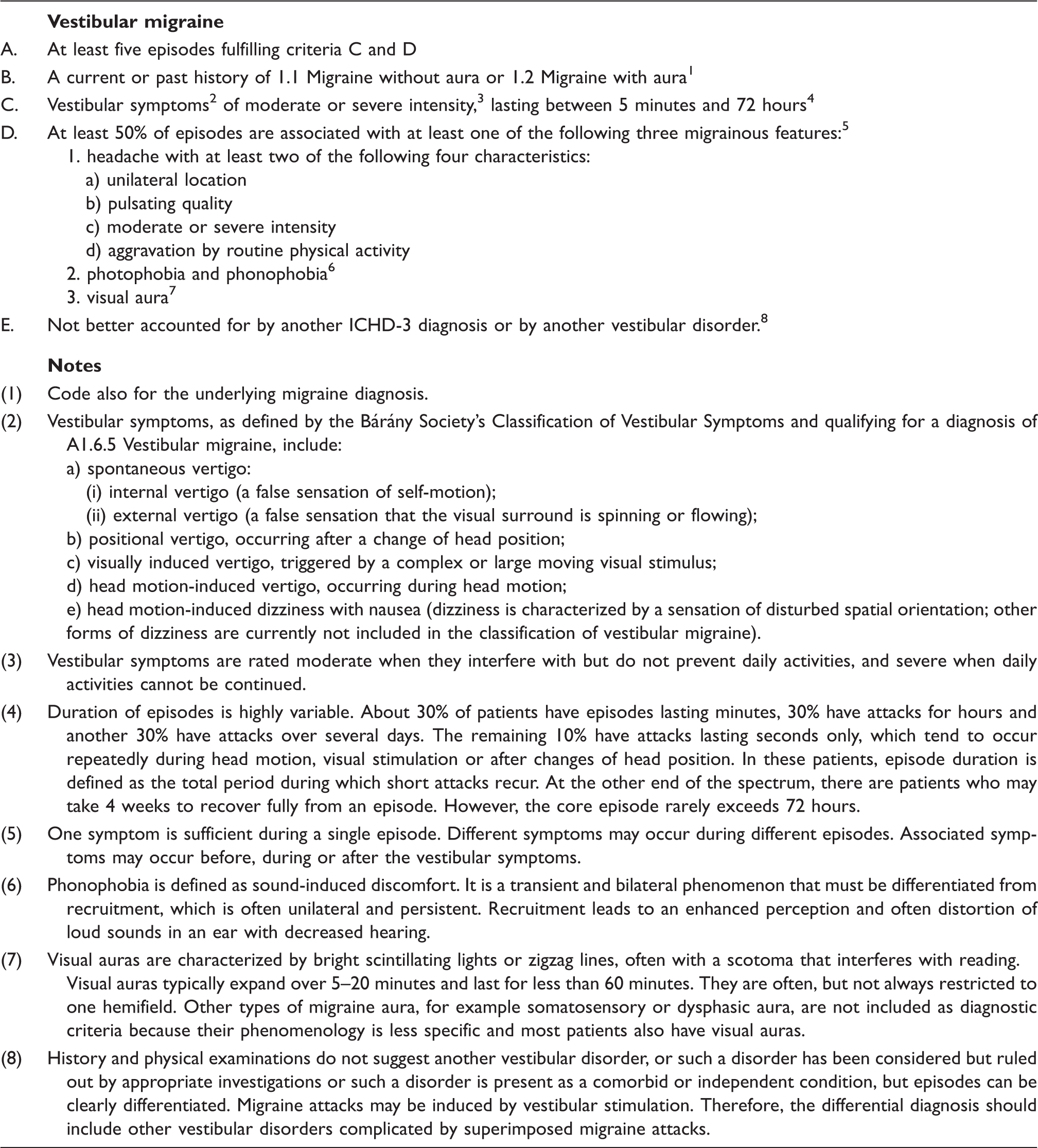
Vestibular migraine: diagnostic criteria.
Epidemiology
In population-based studies the lifetime prevalences of migraine and vertigo in the general population of Germany as a representative of the Western industrial nations were approximately 16% and 7%, respectively (1,11). In the general population the lifetime prevalence of vestibular migraine was 1%, with a 1-year prevalence of 0.9% (12). A large epidemiological study showed the concurrent presence of both symptoms in 3.2% of all patients (1). A different survey described the presence of dizziness or vertigo in 47.5% of patients with migraine during a severe migraine attack with pain intensity of 7 or more on a visual analogue scale (VAS 0 = no pain, 10 = worst imaginable pain) (13).
Vestibular migraine can occur in any period of life (7,14,15). Women are affected more frequently than men with a gender ratio between 1.5 and 5 (7,15–17). A familial clustering as well as an autosomal-dominant inheritance with a lower penetrance in males was described (18). In most patients vestibular migraine appears in an advanced period of life, and often with a temporal delay to the first onset of migraine (7,17). The association of vestibular symptoms with migraine with aura is controversial, as some studies found this connection (7,17,19–22), whereas others discovered that patients with migraine without aura have vestibular symptoms more often or at least equally often as migraine with aura patients (7,16). In elderly patients, especially postmenopausal women, the typical migraine attacks are sometimes replaced by isolated episodes of vertigo, dizziness or a transient feeling of disequilibrium (23).
Clinical presentation
A common problem in taking the patient’s history is the imprecise description of the type of vertigo. Rotational and positional vertigo are often not well distinguished from dizziness and gait disturbances. This is primarily a problem related to the multiformity of the symptom vertigo that many patients find hard to describe. In vestibular migraine rotational or nonrotational vertigo can occur spontaneously or in association with a change of position (12). In a large population-based survey, the most frequent vertigo symptoms were a spontaneous rotatory vertigo in 67% followed by positional vertigo in 24% of patients with vestibular migraine (12). Interestingly, during a migraine attack the initial spontaneous rotatory vertigo can turn into positional or illusion of movement-type vertigo with gait disturbances (24,25). An increased sensitivity to motion, particularly to movements of the head, was also reported (15,26). These symptoms can be similar to those of motion sickness (e.g. balance disturbance, illusion of motion and nausea). Sometimes vertigo is enhanced by looking at fast-moving visual objects and resembles visual vertigo (27,28).
The duration of attacks can vary from a few seconds (10% of patients) to some minutes (30% of patients), some hours (30% of patients) and even up to a few days (30% of patients) (7,14,16,19). In this regard, the distinction between an active migraine attack and the postdromal phase with slowly remitting vestibular symptoms can be challenging (Figure 1) (29). In contrast to the former understanding of the condition, only 10–30% of patients report a typical vestibular aura with a duration between 5 and 60 minutes (7,17). Vertigo or dizziness can precede the migraine attack, but can also occur during or after the headache (14,16,17). In less than one-quarter of the patients, each headache episode is accompanied by dizziness or vertigo (12). Sometimes the vertigo even occurs as the major symptom, to the extent that these patients only report a slight feeling of pressure in the head, without necessarily describing this symptom as a typical migrainous headache. Approximately 30% of all vestibular migraine attacks are not accompanied by headache. In some patients vertigo and headache never appear at the same time (14,16,17). In these cases, the typical migraine-associated symptoms like phono-/photophobia, osmophobia, nausea and vomiting, aggravation by movement or the need to rest are the crucial symptoms for diagnosis (30). Aura-phenomena such as visual (fortifications, positive and negative scotomas, visual field deficits) or somatosensory (hypoesthesia, paraesthesias) symptoms can underline the diagnosis. Vestibular migraine has the same triggers as typical migraine, for example menstruation, sleep restriction, stress, nutrition (certain sorts of cheese, red wine and glutamate) and possibly change of weather, among others. Furthermore, caloric examination or stimulation of the vestibular system can provoke a migraine attack (31). However, in these cases the development of a vestibular migraine attack is not obligatory.
Distribution of vestibular symptoms during a migraine attack.
During an attack as well as in-between attacks, mild clinical signs of central-vestibular dysfunction were reported (7). Gaze-induced nystagmus, saccadic pursuit (especially vertically), central positional nystagmus and a slight horizontal or vertical spontaneous nystagmus can be observed, and might support the diagnosis. However, other central causes of central ocular abnormalities need to be ruled out (7). A more recent study reported that positional nystagmus is the most common symptom between two attacks of vestibular migraine, with a prevalence of 28%. Up to 41% of studied patients showed mild disturbances of ocular movement. Nevertheless, after an average of 9 years this symptom was only present in one of nine cases (32). This finding indicates that central impairments are transient and normalize between attacks. Vertigo, as well as headache, generally worsens during movement. In-between attacks patients are also more susceptible to kinetosis. They report a decreased tolerance of riding carrousels, boats or cars or even watching 3D movies (33).
Approximately two-thirds of patients visit a physician because of their symptoms, but vestibular migraine was diagnosed in only 20% of these patients (34). The various interpretation by different specialties regarding the combination of both symptoms – headache and vertigo – is quite interesting. A survey among neurologists and otologists reports that neurologists would diagnose a vestibular migraine in 82% of patients with vertigo and headache, whereas this opinion was shared only by 64.5% of ENT physicians. Surprisingly, in the context of this survey, 19% of ENT physicians and even 14.5% of neurologists declared never to have treated a patient with vestibular migraine before (34).
Pathophysiology
The exact pathophysiological mechanisms of vestibular migraine remain unclear. Most theories concerning the pathogenesis of vestibular migraine resemble those of migraine without offering a hypothesis explaining the complex processes to its full extent (35). The neuroanatomically evident tight interneural connections between the vestibular system and nociceptive brain stem areas, that is the dorsal raphe nuclei, the locus coeruleus and the lateral tegmentum, as well as the connections between inferior, medial and lateral vestibular nuclei and the caudal trigeminal nucleus, strongly indicate an interaction between the nociceptive and vestibular systems (36).
A few experimental studies observed a strong interconnection and increased signal transmission between the nociceptive and the vestibular systems in patients with vestibular migraine compared with healthy control subjects. Painful electric stimulation of the skin area of the trigeminal nerve in patients with vestibular migraine induced a nystagmus, whereas no nystagmus was observed in healthy control subjects (37). This finding was seen as a correlate of cortical hyperexcitability and central sensitization of the trigeminal system in migraine, with a specific effect on the vestibular system in patients with vestibular migraine (37). Many studies also suggested hyperexcitability of the vestibular system in these migraine patients (38–40). Murdin et al. (2010) observed a decreased suppression of otoacoustic emissions in patients with vestibular migraine in comparison with healthy controls (38). In patients with vestibular migraine the perceptual threshold of dynamic head movements was reduced compared with control subjects (39). A different study observed increased motion sensitivity ranging up to motion sickness in patients with migraine (33). The cause of this presumed cortical hyperexcitability and, in particular, the impairment of the vestibular system remains unclear. The theory of a ‘locus minoris resistentiae’, that is a susceptibility as a result of diseases affecting the vestibular system (e.g. vestibular neuritis) with a subsequent involvement of the vestibular system on the basis of a preexisting migraine, is conceivable but remains unproven.
As a result of the close relationship between migraine and episodic ataxia type 2 (EA2) with associated balance disturbances, the hypothesis of vestibular migraine as a channelopathy was suggested by some authors (41). Alterations of the voltage-dependent calcium channel gene CACNA1A were observed both in familial hemiplegic migraine (FHM) and episodic ataxia type 2 (EA2), and could establish a genetic connection between migraine and vestibular disorders (42). However, the proof of a genetic defect in this region in patients with vestibular migraine is still missing (41,43). The CACNA1A gene encodes the alpha-1-a subunit of neuronal calcium channels, which are predominantly expressed in the cerebellum. This fact was previously used to explain the frequently observed interictal central-vestibular signs such as gaze-evoked nystagmus, etc., in these migraine patients. Different authors described a dysfunction of calcium channels for migraine patients with aura not suffering from FHM, suggesting this as a generalized problem in patients with migraine (44).
‘Cortical spreading depression’ (CSD) in both multi-sensory vestibular areas of the cortex and brainstem was used as an explanation for ‘aura’-like dizziness/vertigo attacks with consecutive headache (14). However, an isolated CSD, which is limited to the brainstem without causing any other symptoms, is not very likely. The majority of symptoms described by patients remains unexplained. In the past, this fact has been used as a pathophysiological basis for distinguishing vestibular from basilar type migraine, which requires the headache to be accompanied by at least two brainstem symptoms (30).
Neurotransmitters such as calcitonin gene-related peptide (CGRP), serotonin, norepinephrine and dopamine modulate the neuronal activity of central as well as peripheral-vestibular neurons and might influence the pathogenesis of vestibular migraine (14–16,45). A unilateral release of these transmitters in a unilateral migraine attack might lead to a vestibular imbalance causing rotatory vertigo, whereas a bilateral release of transmitters might provoke a static imbalance leading to positional vertigo and gait disturbance. However, experimental proof in humans is still lacking.
Differential diagnoses
Differential diagnosis of vestibular migraine.

Episodic ataxia type 2 (EA2) typically presents with sudden onset dizziness or vertigo, with ataxia and occulomotor signs. This cannot be distinguished from vestibular migraine without headache clinically and underlines the close relationship of the two disorders with possibly common genetic origin in the CACNA1A gene and a shared pathophysiological pathway in some patients (54).
Benign paroxysmal positional vertigo (BPPV) is the most common cause for relapsing attacks of vertigo (55). BPPV has to be considered in the differential diagnosis of vestibular migraine in patients with positional vertigo and accompanying headache (56). During an acute episode of vertigo, performance of diagnostic maneuvers might be the only way to distinguish both disorders clinically. In the case of vestibular migraine, the nystagmus also depends on the patient’s position, but is generally not persistent or paroxysmal and does not match a specific semicircular canal. Furthermore, frequency and timing of attacks are clearly distinct. Regarding vestibular migraine, positional vertigo occurs several times per year or month with a duration of some hours up to few days, whereas BPPV leads to episodes of short lasting vertigo generally with a duration of a few weeks or months. If reappearing at all, it reappears only after several months or even years (56,57). This aspect can also help in distinguishing BPPV from vestibular paroxysmia, which is a disease based on a neurovascular conflict with compression of the 8th cranial nerve and absence of the typical positional vertigo usually seen in BPPV. In the context of BPPV and migraine, an increased rate of coexistence of both diseases is described. Patients with idiopathic BPPV suffer from migraine three times as often as patients with symptomatic BPPV (following trauma or operation). Moreover, patients with idiopathic BPPV suffer from migraine twice as frequently compared with an age- and gender-matched comparison group (58,59).
Transient disorders of the vertebrobasilar circulation are additional and crucial differential diagnoses of vestibular migraine. This is especially true in patients with vestibular migraine suffering from only a few attacks or, in the case of the first attack, suffering from pronounced vertigo or balance disturbances. In these cases mild central-vestibular symptoms associated with a vestibular migraine attack can further complicate the clear clinical differentiation (see above).
Psychogenic dizziness is frequent in patients with anxiety disorders or depression. On the other hand, patients with vestibular migraine are prone to develop secondary somatoform dizziness (60). Under these circumstances, the distinction of both diseases can be difficult. More than 50% of patients suffering from vestibular migraine are supposed to have a comorbid psychiatric disorder (61). In this context the association seems to be bidirectional, as depression as well as anxiety disorders are risk factors for migraine, especially for developing a chronic migraine (62). Because of the close connection of psychological factors with dizziness and migraine, some authors suggested the definition of a distinct syndrome called ‘migraine-anxiety related dizziness’ (MARD) (63). However, a reasonable biological basis as well as plausible pathophysiological models justifying such a disease entity are still lacking.
Syncope occurs in approximately 5% of 500 studied patients with migraine (64). A population-based study showed an increased frequency of syncopes (46% vs. 31%) and enhanced orthostatic sensitivity (32% vs. 12%) in patients with migraine compared with controls (65). In this context the observation of inducing an orthostatic hypotension in patients with migraine by low-dose dopamine agonists and normalizing this by dopamine antagonists is particularly interesting (66). This finding was interpreted as a proof of hypersensitivity to dopamine in migraine and might be responsible for some of the observed dizziness symptoms in patients with vestibular migraine.
Basilar-type migraine
Basilar-type migraine, in contrast to vestibular migraine, already has been defined in the ICHD-2 classification and can be distinguished clearly from vestibular migraine in most cases (30). In the revised ICHD-3 beta classification it is termed migraine with brainstem aura (10). Less than 10% of patients with vestibular migraine meet the diagnostic criteria for basilar-type migraine (16,17). By definition, basilar-type migraine requires at least two aura symptoms, which are assignable to the vertebrobasilar territory, which last between 5 and 60 minutes and which are followed by a typical migraine headache (30). The extent to which both kinds of migraine can be distinguished and to what degree there are overlaps in some patients or disease constellations remains the subject of current research.
Therapy
The therapeutic recommendation for vestibular migraine is currently based on the guidelines of regular migraine. There is only one small, controlled and randomized clinical study on the particular treatment of vestibular migraine (67). This study suggested a benefit from zolmitriptan in 38% (three of eight episodes) of patients with vestibular migraine attacks, whereas in the placebo group a positive effect was observed in only 22% (two of nine episodes). Unfortunately, the validity of this study is limited because of the large confidence intervals and the small number of patients recruited (n = 10) with only 17 reported attacks (67).
All other therapeutic approaches are based on case reports, retrospective cohort studies and open-label trials. In this context, a retrospective study with 111 patients indicated a positive effect of drugs primarily used to treat migraine in patients with vestibular migraine (68). In this regard, drugs intended for acute treatment such as sumatriptan, nonsteroidal anti-inflammatory drugs (NSAID) and ergots as well as preventive migraine medications such as beta blockers, tricyclic antidepressants, methysergide, flunarizine, topiramate and valproic acid were studied (69). Even less conventional drugs such as benzodiazepines, selective serotonin reuptake inhibitors (SSRI), pizotifen, dothiepin, lamotrigine, acetazolamide as well as behavioral modification such as special diets were reported to have a positive effect on vestibular migraine (69). However, it is difficult to extract a clear therapeutic recommendation for the particular treatment of vestibular migraine from these data. Furthermore, it must be kept in mind that inconsistent definitions of vestibular migraine were used in the context of these studies. As a result, the examined patient groups were quite heterogeneous. In future, this deficit should be eliminated by the new diagnostic criteria, hopefully leading to more comparable, high-quality studies.
Recommendations for treatment
The treatment recommendations for vestibular migraine are similar to those of migraine. Some of the following treatment recommendations are based on the authors’ experience. According to the available literature, zolmitriptan 5 mg (tablet, nasal spray, dissolvable tablet) should be the first choice in the acute vestibular migraine attack. Analogous to migraine, any other triptan may be just as effective (70). Patients with excessive nausea or vomiting may prefer non-oral applications (i.e. nasal spray, suppositories or subcutaneous injections) or intravenous options such as acetylsalicylacid 1000 mg with metoclopramide 10 mg or dimenhydrinat (62.5 mg). Prophylactic medications are not different from treatment of migraine with or without aura and include propranolol 80–240 mg, metoprolol 50–200 mg, bisoprolol 5–10 mg or flunarizine 5–10 mg per day in patients with over three attacks per month, very long lasting or disabling attacks, or failure to respond to acute treatment. Topiramate 25–100 mg and valproic acid 500–600 mg may be used as well. Combination of drugs belonging to the same class is probably not reasonable. Patients with frequent migraine attacks (>15 per month) or more than eight migraine days per month should receive either topiramate 25–100 mg or amitriptylin 50–150 mg. A trial of onabotulinumtoxin type A (155 MU), as used in the treatment of chronic migraine, may also be reasonable, but this option has not yet been proven to improve vestibular symptoms. Patients who predominantly complain of vertigo or dizziness with typical aura duration, but without frequent migraine headache might be successfully treated with lamotrigine 25–100 mg per day (71).
Clinical implications
This review is of major importance for neurologists as well as ENT physicians as vestibular migraine is an often misdiagnosed disease, which has recently gained attention because of the new diagnostic criteria published by the International Headache Society and the Báràny Society. These criteria are important for future research on the epidemiology, clinical symptoms and standardized therapy of vestibular migraine.
Footnotes
Acknowledgements
This review was in parts translated into English from its original German version. We specifically thank Michael Strupp, Andreas Straube, Stefanie Fördereuther and Zaza Katsarava, who co-authored the German version for their invaluable input and honored contribution.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
Dagny Holle has received a research grant from Grünenthal and Allergan. Hans-Christoph Diener has received honoraria for participation in clinical trials, contribution to advisory boards or lectures from Addex Pharma, Allergan, Almirall, AstraZeneca, Bayer Vital, Berlin Chemie, Coherex Medical, CoLucid, Böhringer Ingelheim, Bristol-Myers Squibb, GlaxoSmithKline, Grünenthal, Janssen-Cilag, Lilly, La Roche, 3 M Medica, Minster, MSD, Novartis, Johnson & Johnson, Pierre Fabre, Pfizer, Schaper and Brümmer, SanofiAventis, and Weber & Weber; received research support from Allergan, Almirall, AstraZeneca, Bayer, Glaxo-Smith-Kline, Janssen-Cilag, and Pfizer. Headache research at the Department of Neurology in Essen is supported by the German Research Council (DFG), the German Ministry of Education and Research (BMBF), and the European Union. Mark Obermann has received scientific grants by the German Federal Ministry of Education and Research BMBF 01EM 0513.