
Abstract
Importance and Objective
Headache is the most common symptom in spontaneous CSF leaks, frequently associated with additional manifestations. Herein, attention is drawn to movement disorder as a notable manifestation of spontaneous CSF leaks.
Design
Four women and one man (ages 51–78 years) with spontaneous CSF leaks and movement disorders were evaluated clinically and by pertinent neuroimaging studies with follow-up of one to seven years (mean 3.2 years).
Results
The movement disorder consisted of choreiform movements in two patients, torticollis in one, mixed tremor in one, and parkinsonism in one. All except the last patient had headaches (orthostatic in one, Valsalva maneuver-induced in one, both orthostatic and Valsalva-induced in two, lingering low-grade headache in one). Diffuse pachymeningeal enhancement and sinking of the brain was noted in all. CT-myelography showed definite CSF leak in three and equivocal leak in one, while no leak could be located in the fifth patient. Two patients improved over time with complete resolution of the movement disorder. One responded to epidural blood patch with complete resolution of his choreiform movements. Two patients required surgery and epidural blood patches. Results were drastic but nondurable in one, while complete recovery was achieved in the other.
Conclusion
Movement disorders are uncommon in spontaneous CSF leaks but occasionally can be one of the major components of the clinical presentation.
Introduction
Headaches in cerebrospinal fluid (CSF) leaks.
Clinical manifestations, other than headache, in cerebrospinal fluid (CSF) leaks.

The purpose of this communication is to draw attention to the occurrence of various movement disorders resulting from spontaneous CSF leaks. Five patients with spontaneous CSF leaks are reported in whom a movement disorder was one of the major components of the clinical presentation. The movement disorder was chorea in two, focal dystonia (torticollis) in one, a mixed orthostatic tremor in one, and finally parkinsonism in one patient. One of the patients with choreiform movements has been previously reported and is only briefly described, but with additional follow-up (4).
Patient No. 1
A 59-year-old, tall, slender man was seen with orthostatic and exertional headaches, nausea, cognitive difficulties, choreiform movements, abnormal gait, dysarthria, and dysphagia. Evaluation in another institution included head magnetic resonance imaging (MRI) with findings suggestive of intracranial hypotension computed tomography (CT)-myelography revealing a possible leaking meningeal diverticulum at T9–10. Surgery to repair the meningeal diverticulum resulted in good improvement, but for only one week. At the time of evaluation at our institution, there was hyperkinetic dysarthria, choreiform movements of face and limbs, and cognitive difficulties including trouble with attention, concentration, learning, and memory. Diffuse pachymeningeal enhancement, descent of cerebellar tonsils below the foramen magnum, and crowding of the posterior fossa were noted on head MRI. CT-myelography showed a CSF leak at the cervicothoracic level. He was treated with a low cervical epidural blood patch (EBP). Within several days, he showed substantial improvement and within weeks was entirely asymptomatic. Choreiform movements had completely resolved. He returned five years later with recurrence of the leak clinically manifested by orthostatic headache only. He was treated with an EBP with very good but not permanently durable response.
Patient No. 2
A 51-year-old woman presented with orthostatic wooziness, exertional-Valsalva headaches, positional vertigo, head tremor, and spasmodic torticollis. There was history of an unspecified meningitis 10 years earlier leading to hospitalization with excellent recovery. Five years earlier she had been evaluated in another institution for exertional-Valsalva headaches. Head MRI had revealed “meningeal thickening” and low-lying cerebellar tonsils. The former was attributed to the past meningitis and the latter to a Chiari malformation. Two years later, she underwent suboccipital craniectomy and C1 laminectomy to treat the presumed Chiari. Symptoms persisted. She was later evaluated at our institution. Head MRI showed diffuse pachymeningeal enhancement, substantial descent of the cerebellar tonsils, flattening of the anterior pons (Figure 1) as well as the postoperative changes of the previous surgery. CT-myelography showed 1–2 mm thick ventral epidural CSF collection extending from C4 to T8–9. She received three cervical EBPs with only partial benefit. She decided to avoid provoking factors as much as possible and to carry on with her routine. Approximately 18 months later she began to note side-to-side head tremors and involuntary pulling of her head to the right. After another five months she was again seen in our institution with positional vertigo, Valsalva maneuver-induced transient headaches in addition to her head tremor and cervical dystonia. On examination there were phasic dystonic movements of the head to the right and mild right neck dystonic deviation. The rest of the neurologic exam was normal. Head MRI continued to show diffuse pachymeningeal enhancement and evidence of brain sag. Patient did not wish to undergo invasive studies or subject herself to possible surgery. She continued avoiding provoking factors. On a follow-up five years later, patient was completely asymptomatic and reported gradual resolution of headaches and dizziness in tandem with gradual resolution of her cervical dystonia without any medications or other interventions. As she had become asymptomatic, follow-up imaging could not be justified.
Patient No. 3
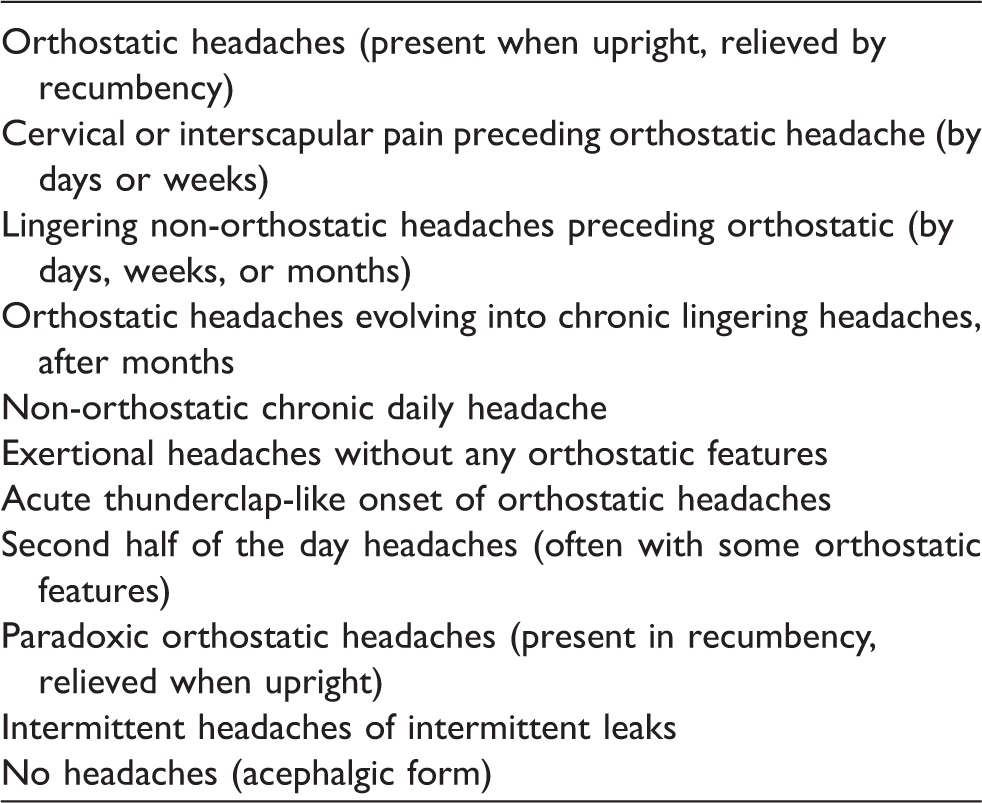
A 60-year-old woman presented with one-year history of bifrontal head pressure sensation and vague headaches, mild gait unsteadiness, abnormal movements of the face, and memory difficulties. Her examination revealed mild cognitive difficulties but substantial deficits in recall, and choreiform movements of face, trunk, and limbs. Gait was normal except for mild difficulty with tandem gait and alterations in connection with the movement disorder. There was a large congenital hemangioma involving the buttock, and anterior and lateral thigh on the left, partially resected as a child. The left leg was chronically swollen. Head MRI showed diffuse pachymeningeal enhancement, pituitary enlargement, imaging evidence of sinking of the brain with descent of the cerebellar tonsils below the foramen magnum, and obliteration of the perichiasmatic cistern (Figure 2). On CT-myelography, nerve root sleeves were dilated at the L1–L2 and left S1 with strong suggestion of CSF leak at former. This was confirmed at surgery and was repaired. The patient made an impressive recovery within a month. Gait and cognitive function improved and the choreiform movements markedly decreased. She could now use the curling iron to fix her hair and started to play her piano again. The very bothersome head pressure sensation essentially resolved. After two months, symptoms began to return and increase again. When she was rechecked four months postoperatively, she displayed essentially the same preoperative manifestation although to a milder degree. Head MRI again demonstrated diffuse pachymeningeal enhancement and imaging evidence of sinking of the brain. She was treated with a low lumbar EBP finally with complete resolution of all of her symptoms within several months.
Patient No. 4
A 52-year-old right-handed woman developed orthostatic headaches, headaches provoked by Valsalva-type maneuvers, and subsequently also orthostatic mixed static and movement tremor of the upper limbs, especially hands and fingers predominantly on the right side, in addition to tinnitus, altered hearing, vertigo, and gait unsteadiness. She had history of right eye retinal detachment in her forties and her sister had joint hypermobility. Head MRI obtained one year after the onset of first symptom revealed findings pointing to intracranial hypotension (Figure 3). CSF opening pressure was 70 mm H2O. A subsequent EBP caused marked improvement in the headaches and complete resolution of her other symptoms but for only two weeks. She had been subsequently treated with EBPs every six weeks or intravenous (IV) saline infusions every three weeks.

Two years after the onset of the symptoms, the patient was seen at our institution. There was gait unsteadiness and substantial difficulty with tandem gait. Muscle stretch reflexes were exaggerated in the lower limbs but plantar responses were flexor. There was inferior temporal visual field defect of the right eye related to the previous retinal detachment, and there was mixed static-action tremor of the hand and fingers, more on the right in the upright position that would resolve with recumbency within about 30 minutes.
On head MRI, there was diffuse pachymeningeal enhancement, descent of the cerebellar tonsils below the foramen magnum, flattened anterior pons, enlarged pituitary, flattened optic chiasm, and obliteration of the perichiasmatic cistern. Indium-111 cisternography showed a paucity of radioactivity over the cerebral convexities at 24 hours. CT-myelography showed numerous bilateral nerve root sleeve diverticula without evidence of CSF-contrast extravasation except for a possible leak at the left S1 nerve root level. She received two EBPs at S1, each giving two weeks of relief. Two months later she underwent S1, S2, and partial L5 hemilaminectomies with exploration of common dorsal sac and S1 and S2 nerve roots. No definite site of the leak was identified. The area was packed with Gelfoam and fibrin glue. Postoperatively there was six weeks of relief from symptoms. Follow-up head MRI showed decreased but still persistent pachymeningeal enhancement. CT-myelography showed no evidence of a leak. Patient was reluctant to receive another EBP and preferred to continue with IV saline infusions every three weeks.
Patient No. 5
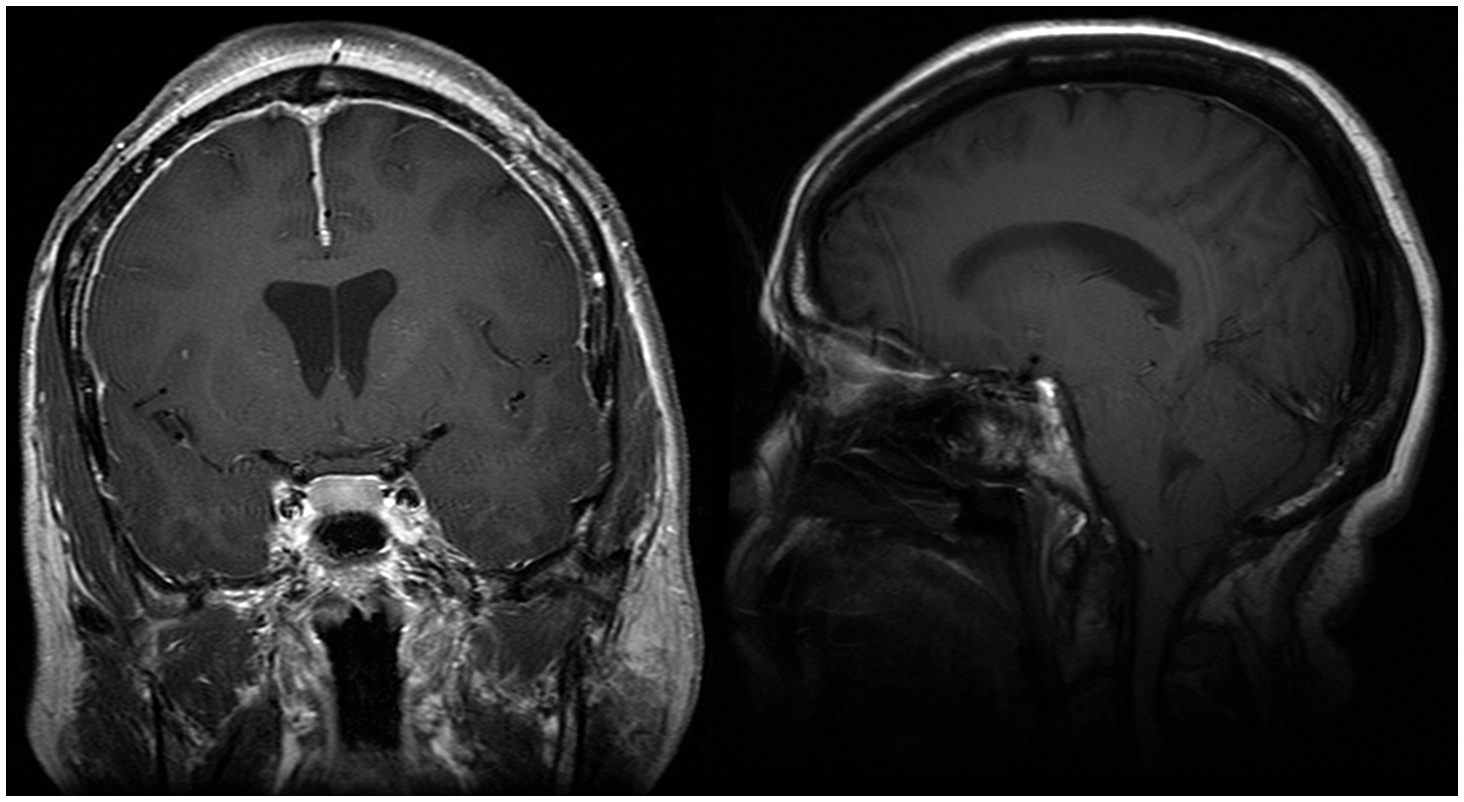
A 78-year-old nurse presented with a two-month history of gait unsteadiness, slowness of thinking and trouble with memory, and a two-week history of vertigo and nausea. A recent head MRI had shown diffuse pachymeningeal enhancement and bilateral subdural fluid collections. This resulted in her referral to our institution with concern about intracranial hypotension and CSF leak. She denied headaches. On neurological examination there was small stepped gait, mild rigidity, and resting tremor of the upper extremities, hyperactive muscle stretch reflexes, and trouble with abstraction and concentration. The examining neurologist did notice parkinsonism and suspected neurodegenerative disease vs. parkinsonism secondary to CSF leak. Review of the head MRI showed diffuse uninterrupted and non-nodular pachymeningeal enhancement and thin biconvexity subdural fluid collections. Cerebellar tonsils were not below the foramen magnum but iter was significantly below the incisural line (Figure 4). CT-myelography did not show a definite site of a CSF leak. There was severe spinal stenosis at L3–4 but the patient did not have any symptoms of pseudoclaudication. CSF opening pressure was 62 mm H2O. Clinically she was improving. When this author saw her in neurologic consultation four months later, her gait and speech had normalized and cognitive function had improved to above average. There was no parkinsonism whatsoever. She felt “100% improved.” Follow-up imaging, therefore, was not carried out.

Discussion
Many patients with spontaneous CSF leaks, in addition to headache, report one or more of a variety of manifestations listed in Table 2; and uncommonly some may report no headaches at all. The most commonly proposed mechanism of headache in spontaneous CSF leaks has been sinking of the brain and, therefore, traction on pain-sensitive suspending elements of the brain such as blood vessels. Another proposed mechanism has been engorgement of the intracranial vascular structures, especially venous sinuses and large veins (2). Vertical pressure on the tentorium and the floor of the posterior fossa or foramen magnum may also play a role or sometimes a combination of these factors may come to play. Nonetheless, the scope of variability in the headaches and MRI findings in CSF leaks is such that in some cases a convincing single theory cannot be presented. This becomes even more complex in acephalgic forms of spontaneous CSF leaks, where imaging abnormalities may exist but headache will be absent, such as the fifth patient reported in this communication. It is hoped that with further research more convincing explanations may emerge. Movement disorders of different types may occur as one of the “non-headache” manifestations of this disorder, although quite uncommonly. The case series reported here demonstrates occurrence of a variety of movement disorders plus additional manifestations. All but one patient also had headaches.
The pathophysiologic mechanisms of various “non-headache” clinical manifestations of CSF leaks have been typically attributed to such factors as sinking of the brain; pressure on various locations or lobes of the brain or brain stem; pressure on (or traction or distortion of) different cranial nerves; or pressure changes in the veins, venous sinuses, and peripheral labyrinthine system (pressure changes in the endolymphatic and perilymphatic fluid) (2,5). Several uncommon manifestations of spontaneous CSF leaks have been attributed to pressure on deep midline structures of the brain, brain stem, or diencephalic or mesencephalic structures. Examples include stupor (6), coma (7), parkinsonism (8), encephalopathy (9), and chorea (4).
Pakiam et al. (8) described a 54-year-old woman with intracranial hypotension with an unusual presentation of bradykinesia, gait imbalance, and resting tremor of one hand leading to a referral diagnosis of Parkinson’s disease. She later also developed dysphagia and nasal speech. She had only mild headaches with non-convincing orthostatic features. On head MRI, there was definite evidence of sinking of the brain and distortion of the brain stem. The patient had low CSF opening pressure and showed a very good response to EBP. The authors thought that the patient’s parkinsonism had likely resulted from compression on and distortion of the brain stem. In our patient with parkinsonism, although the cerebellar tonsils were not below the foramen magnum, there was significant descent of the iter below the incisural line. Iter is the caudal (proximal) opening of the aqueduct of Sylvius as seen in midsagittal MR images of the brain. The incisural line is a line drawn from confluence of straight sinus, inferior sagittal sinus, and great vein of Galen to the anterior tuberculum sellae. In the series of Pannullo et al. (10), in six patients with documented intracranial hypotensions and imaging evidence of brain sagging, careful measurements showed descent of cerebellar tonsils below the foramen magnum alone in one patient, cerebellar tonsillar descent plus descent of iter in two patients, and descent of the iter only in three patients. Our patient with parkinsonism, in addition to diffuse pachymeningeal enhancement and low CSF opening pressure, had descent of the iter only and seems to fall into this category. Chorea in patients with spontaneous CSF leak has been attributed to sagging of the brain and pressure on the deep midline structures, basal ganglia, and their connections (4). Both of our patients with chorea had notable descent of the cerebellar tonsils below the foramen magnum. Of the two remaining patients, one with mixed tremor and the other with spasmodic torticollis, both had descent of cerebellar tonsils below the foramen magnum. Although spontaneous remission of cervical dystonia has been reported (11), in our patient with cervical dystonia, resolution of the torticollis occurred in conjunction with resolution of her other symptoms including the headaches and dizziness. Turgut et al. reported the case of a 57-year-old man with gradually increasing postural bilateral hand tremor and typical head MRI findings for intracranial hypotension with confirmation of the leak by MR cisternography. The tremor resolved following EBP (12). Head MRI in the five patients with CSF leaks and movement disorder reported in this communication showed diffuse pachymeningeal enhancement in all. Four patients showed descent of the cerebellar tonsils below the foramen magnum. In one of these four, the location of the iter could not be reliably identified as the result of brain stem distortion. In the remaining three, the iter was low lying. Finally, in one patient, descent of the cerebellar tonsils was not noted but the iter had notably descended below the incisural line. Thus all patients had evidence of sinking of the brain, which is presumed to be the fundamental underlying cause for these movement disorders by compressing, stretching, and distorting the deep brain and brain stem structures.
Targeted EBP resulted in complete resolution of choreiform movements in one patient. In the second patient with choreiform movements, the symptoms responded drastically although not entirely completely to surgery aimed at correction of the CSF leak. When symptoms began to reoccur, EBP proved to be very beneficial. Two patients, one with torticollis and the other with parkinsonism, spontaneously and gradually improved, most likely as the result of spontaneous resolution or considerable slowdown of the leak. Finally, one patient with mixed tremor responded to surgery and EBPs quite well, but unfortunately the responses were not durable.
The main concern of each patient at presentation was not about the movement disorder but other symptoms. None had been treated pharmacologically for movement disorder. Patient No. 5 had a five-year history of restless leg syndrome and was on pramipexole 0.25 mg at bedtime. In the past she had tried carbidopa/levodopa and also gabapentin.
The ideal diagnostic triad of orthostatic headaches, low CSF opening pressure, and diffuse pachymeningeal enhancement on MRI unfortunately cannot be expected in many patients. There is substantial variability in just about every aspect of spontaneous CSF leaks including clinical and imaging manifestations, CSF findings, as well as response to treatment (5). As a result, there are substantial and sometimes frustrating challenges in the management of these patients. Even in only these five patients reported here, several challenges such as unusual presentation, incomplete symptom resolution, recurrences, and unpredictability of outcome come to light. While with treatment some patients become symptom free, some continue with low-grade lingering symptoms likely in connection with transformation of the leak to a slower flow leak, and sometimes spontaneous resolution occurs without any treatment as the result of spontaneous cessation of the leak.
Movement disorder is an uncommon component of clinical presentation of the CSF leaks. The five patients reported here were all seen and evaluated by the author. Therefore, their selection was through his daily practice observations rather than formal screening of all patients seen in the parent institution. Furthermore, the author’s practice in connection with CSF leaks is skewed toward leak site identification difficulties, treatment failures, or unusual presentations. Therefore, it is not possible to give an estimate on overall frequency of this uncommon manifestation on the basis of this experience.
Conclusion
Clinical presentations of spontaneous CSF leaks vary considerably. A variety of movement disorders can be among the components of this spectrum. They are uncommon but need to be recognized to help minimize diagnostic confusion.
Clinical implications
Headache is the most common clinical presentation of spontaneous cerebrospinal fluid (CSF) leaks but commonly, although not invariably, it is accompanied by additional clinical manifestations. One or more of the additional manifestations may sometimes dominate the clinical presentation. Movement disorders as one of the components of the clinical presentation of spontaneous CSF leaks are quite uncommon and can cause diagnostic confusion. Five patients with spontaneous CSF leaks and various types of movement disorders are reported to draw attention to this uncommon but diagnostically important association.
Footnotes
Acknowledgments
Dr Mokri had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. He wishes to thank Ms Lori Lynn Reinstrom, research administrative assistant, Mayo Clinic Rochester, for her excellent editorial assistance.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.