
Abstract
Background
Habituation deficit, suggesting a deregulation of cortical excitability, represents a typical hallmark of interictal stages of migraine. We previously demonstrated that several neurophysiological markers of altered cortical excitability are significantly correlated to spontaneous clinical fluctuations of migraine. We therefore aimed at verifying whether clinical fluctuations are correlated to specific patterns of somatosensory evoked potential (SEP) habituation.
Methods
We analyzed habituation after median nerve stimulation of both high-frequency oscillations (HFOs) and N20 SEP in 25 migraine patients and 18 healthy volunteers. Subjects underwent six consecutive series of 500 stimuli.
Results
Migraine patients as a whole showed a significant habituation deficit of the N20 response. Moreover, spontaneously worsening patients show a clear potentiation of this wave in the last block of stimuli, whereas in spontaneously improving patients the N20 amplitude remained stable. Presynaptic HFOs were smaller in worsening patients and larger in improving ones, but they did not undergo habituation in patients as well as in healthy subjects.
Conclusions
Potentiation of the N20 response in spontaneously worsening migraineurs confirms that the reduction of the thalamocortical drive plays a major role in migraine pathogenesis. Moreover, the stable pattern we observed in spontaneously improving patients suggests that compensatory mechanisms can also play an important role. The normal response to repeated stimuli of HFOs in migraineurs might indicate that, although its initial amount depends on clinical conditions, high-frequency thalamocortical drive remains stable during the stimulation and probably reflects the activity of a buffer mechanism.
Keywords
Introduction
The term “habituation” defines a gradual decrease in the strength of the reflex responses when a non-noxious stimulus is delivered repetitively (1). Habituation was first observed in complex behavioral responses (2). However, it can also be observed in bioelectrical responses, such as potentials evoked by visual or somatosensory stimulation. Habituation probably protects the nervous system against sensory overload, saving attention and memory resources for meaningful novel stimuli. This phenomenon has been particularly studied in patients with migraine, since these patients typically show a lack of habituation to repeated stimuli between attacks, whereas during attacks habituation restores (3).
Two main mechanisms have been claimed to explain the lack of habituation in interictal stages of migraine. Several studies on the visual (4–7) and motor cortex (8–10) indirectly suggested that lack of habituation can be consequent to reduced efficiency of intracortical inhibitory circuits. Alternatively, the hyperresponsivity of neurons in primary sensory cortices can be caused by a reduction of the thalamocortical drive. Schoenen et al. (11), by analyzing the response to repeated blocks of stimuli, noticed that the amplitude of the first block was significantly lower in migraineurs than in healthy subjects. More recently, Bohotin et al. (12) evaluated the amplitude of cortical visual evoked response (VEPs) after repetitive transcranial magnetic stimulation (rTMS) in migraineurs. After excitatory (10 Hz) rTMS, habituation became similar to that observed in healthy subjects. Taken together, these data suggest that the hyperresponsivity of cortical sensory neurons is mainly due to a reduction of their refractoriness, rather to a mere disinhibition, in agreement with the earlier “ceiling theory” (13).
The thalamocortical drive in migraineurs has also been studied by analyzing 600 Hz high-frequency oscillations (HFOs) after upper limb electrical stimulation (14,15). HFOs probably reflect the action on the somatosensory system of arousal-related subcortical structures, since they are dramatically reduced by sleep (16), whereas they are significantly enhanced by eye opening (17,18). The activity of this arousal somatosensory system is probably devoted to signal novel stimuli, the relevance of which points out high synaptic efficacy; probably for this reason, HFOs do not undergo habituation in healthy subjects (19). Scalp-recorded HFOs are formed by two subsequent bursts, the former probably generated in thalamocortical radiations, and the latter generated postsynaptically by cortical neurons able to fire repetitively (14,20). It is still debated whether the activity of the postsynaptic burst is generated by excitatory glutamatergic neurons or by inhibitory GABAergic interneurons (15), while it is generally accepted that the activity of the earlier or “presynaptic” burst is linked to the excitatory thalamocortical drive (21). As far as HFO behavior in migraine is concerned, two different studies reported that the presynaptic thalamocortical burst is abnormally reduced during interictal periods in migraineurs (22,23). These results obviously suggest that the reduction of thalamocortical drive plays a major role in determining cortical excitability changes in migraine patients. Some more recent studies, using rTMS or paired associative stimulation (PAS), or analyzing visual evoked responses to repetitive stimulation, reinforced the hypothesis that the reduction of the thalamocortical drive is pivotal in migraine pathophysiology (24–26).
In a previous study (27) we found that HFO reduction was correlated to spontaneous clinical worsening, whereas patients with spontaneous clinical improvement showed enhanced HFOs. Further, we demonstrated that presynaptic HFO reduction in spontaneously worsening patients positively correlated with shortened recovery cycle of the N20 primary response to paired stimulation of the median nerve, which in turn indicates that the refractoriness of cortical neurons in primary sensory cortex is reduced in these patients (28). In this study, we aimed at verifying whether N20 habituation was correlated to spontaneous clinical fluctuations of the disease; moreover, we verified whether HFOs undergo habituation in interictal stages of migraine.
Methods
Subjects
Patients were recruited among the members of the staff of the Hospital “A. Gemelli,” Rome (Italy) and of the IRCCS “La Nostra Famiglia – E. Medea,” Polo FVG, Pasian di Prato (Udine). Only patients who fulfilled diagnostic criteria for migraine with aura (MA. International Classification of Headache Disorders, II (ICHD-II), Headache Classification Committee of the International Headache Society, 2004: code 1.2) and migraine without aura (MO. ICHD-II: code 1.1) were included in the study. We therefore recorded 25 migraine patients (mean age: 31.76 years, range 22–46; 18 women and seven men): five MA (mean age: 33.8 years; three women and two men), and 20 MO (mean age: 31.25 years; 15 women and five men). None of them had ever been administered prophylactic treatments for migraine. No patients were put on any prophylactic drug during the present study. They were compared with 18 healthy volunteers of comparable age (mean age 32.3 years, range 24–48) and gender distribution (12 women and six men) without personal or family history of migraine and devoid of any detectable medical condition, recruited among the members of the staff of the Hospital “A. Gemelli,” Rome (Italy) and of the IRCCS “La Nostra Famiglia – E. Medea,” Polo FVG, Pasian di Prato (Udine). In all 25 migraine patients, somatosensory evoked potential (SEP) recording was performed at least three days before or after their last or their next migraine attack, on the basis of migraine diaries regularly checked by two authors (DR and CV). All participants gave informed consent in accordance with the Declaration of Helsinki and the study was approved by the local ethics committee.
Summary of the clinical features in our migraine patients.

MO: migraine without aura; MA: migraine with aura; F: female; M: male; SD: standard deviation.
SEP recording
SEP recording was performed by using a commercially available five-channel Micromed Evo-quick apparatus. SEPs were elicited on electrical stimulation of the right median nerve on the wrist by using a constant current square wave pulse (0.2 ms width, cathode proximal) and a stimulus intensity set just above the motor threshold. Active electrodes were placed over the contralateral parietal area (P3) referenced to F3. Subjects were asked to lie with eyes closed on a couch in a warm and darkened room. Since high-frequency SEPs are largely influenced by drowsiness or sleep (15), they were asked to signal the occurrence of drowsiness, in order to temporarily stop the examination. However, this maneuver was never necessary. The analysis time was 50 ms, with a sampling rate of 32,000 Hz. The amplifier bandpass was 0.1–3000 Hz (12 dB roll-off). An automatic artifact-rejection system excluded from the average all runs containing transients exceeding ±65 µV at any recording channel. To ensure baseline stabilization, SEPs were filtered off-line by means of a digital filter with a bandpass of 20–2000 Hz. Stimuli were delivered continuously at a repetition rate of 5 Hz; without interrupting the stimulation, six consecutive blocks of 500 sweeps were collected. To analyze HFOs, each P3-to-F3 trace was digitally filtered with a bandpass of 400–800 Hz (continuous wavelet transform, CWT) by means of an automated signal analysis software (Autosignal™, version 1.6).
Data analysis
Data were loaded by technicians on a storage device as anonymous ASCII files and then analyzed on separate computers. Data analysis was performed in a blinded manner by two of the authors of the study (DR and CV); results were then compared. When discrepancies between separated neurophysiological evaluations were larger than 10%, data were discarded, but this was never necessary in the present study. The amplitude of the primary N20 response on the P3-to-F3 traces was measured from the preceding positive peak. For evaluating HFO AUC, we used the same method previously described in a former paper (27). The beginning of the burst was detected approximately in correspondence to the N20 onset on the corresponding low-frequency (LF)-SEP trace, measuring from the first wavelet having a 50% larger amplitude than the electrical noise, while the burst ending at the last wavelet had a 50% larger amplitude than the electrical noise. The burst recorded at the P3-to-F3 array, consisting of a train of about five to eight wavelets, was further divided into two subsequent segments, respectively ending and beginning in correspondence to the N20 peak. The N20 peak latency has already been used as a cut-off point to measure subsequent components within the cortical burst (28). By considering that both bursts had an approximate duration of 5 ms, we calculated the electrical noise in a 5 ms interval (from 35 to 40 ms) where the signal was presumably not generated by neural activity. Since the early burst is thought to be generated in terminals of thalamocortical radiation fibers, whereas the late burst is probably generated by postsynaptic contributions from intracortical neurons, these bursts will be termed “presynaptic” and “postsynaptic” respectively for the rest of the paper. Burst amplitudes were measured as the area under the rectified waveform (AUC). AUC values were then corrected by subtracting the AUC of the electrical noise calculated within the 35–40 ms interval from presynaptic as well as postsynaptic burst areas.
To estimate habituation, we evaluated the individual amplitude slopes of N20, presynaptic HFOs, and postsynaptic HFOs across the six blocks of stimuli. To evaluate clinical fluctuations, clinical changes were expressed as the percentage changes of the number of migraine attacks, according to the following formula: (number of attacks six months after the SEP recording/number of migraine attacks six months before the SEP recording) × 100.
Statistical analysis
Analysis of the first block of stimuli
We first compared SEP data in the first block of stimuli (N20 amplitude, AUC of both presynaptic and postsynaptic HFOs) between healthy volunteers and the whole population of migraine patients. Comparisons were performed by means of Mann-Whitney U-tests.
We further performed nonparametric correlation tests (Spearman) between clinical index and neurophysiological data (N20 amplitude, AUC of both presynaptic and postsynaptic HFOs). When the correlation test was significant, further comparisons were performed by means of Kruskall-Wallis one-way analyses of variance (ANOVAs). To perform Kruskall-Wallis ANOVAs between neurophysiological parameters and clinical scoring, patients were divided into three groups: 1) improving patients: the number of migraine attacks after the test was at least 50% smaller than before; 2) worsening patients: the number of migraine attacks increased by at least 50% after the test; 3) stable patients: no variations (frequency of migraine attacks ranging from less than 50% decrease and less than 50% increase). Such a classification was performed in analogy with therapeutic trials, in which response to drugs is commonly defined as at least a 50% reduction in average monthly migraine frequency (29). Kruskall-Wallis one-way ANOVA ((stable, improved, worsening) condition × neurophysiological parameter) was then performed. Significance level was set at p < 0.05. Post-hoc analysis was performed by means of Mann-Whitney U-tests.
Analysis of habituation
We then compared the individual amplitude slopes concerning N20 and presynaptic and postsynaptic HFOs, between healthy volunteers and the whole population of migraine patients. Comparisons were performed by means of Mann-Whitney U-tests.
We further performed nonparametric correlation tests (Spearman) between clinical index and neurophysiological data (N20 amplitude, AUC of both presynaptic and postsynaptic HFOs). When correlation test was significant, further comparisons were performed by means of Kruskall-Wallis one-way ANOVAs. Kruskall-Wallis one-way ANOVA ((stable, improved, worsening) condition × neurophysiological parameter) was then performed. Significance level was set at p < 0.05. Post-hoc analysis was performed by means of Mann-Whitney U-tests.
Results
Analysis of the first block of stimuli
Statistical analysis failed to find significant differences in neurophysiological parameters between the whole population of migraine patients and healthy controls (N20 amplitude, U-test = 188.5, p = 0.369; presynaptic HFOs, U-test = 175.0, p = 0.218; postsynaptic HFOs, U-test = 207.0, p = 0.658).
Correlation tests failed to find significant correlation between N20 amplitude and clinical index (Spearman test, rho = –0.326, p = 0.11), as well as between clinical index and AUC of the postsynaptic burst (Spearman test, rho = −0.359, p = 0.07). Conversely, correlation test revealed a significant correlation between AUC of the presynaptic burst and clinical index (Spearman test, rho = −0.630, p = 0.0007; see Figure 1).
Migraine patients, clinical index plotted against presynaptic HFO AUC. Spearman test showed a significant correlation between frequency decline of migraine attacks and amplitude increase of presynaptic HFOs.
Since presynaptic HFO AUC showed a significant correlation with the clinical index, we further compared clinical subgroups of patients. As stated above, they were divided into three groups: 10 patients showed a reduction of 50% or more in the number of migraine attacks during the six months following the test (average number of attacks before the test: 4.7/month; average number of attacks after the test: 1.4/month), and were thus classified as “improving.” Eight patients did not show changes in the migraine attack frequency greater than 50% (average number of attacks before the test: 4.12/month; average number of attacks after the test: 4.12/month), and were therefore classified as “stable.” Lastly, seven patients showed a 50% or higher increase in the number of migraine attacks during the six months following the test (average number of attacks before the test: 3.29/month; average number of attacks after the test: 8.29/month), and thus were classified as “worsening.” See Table 1 for analytical data.
Kruskall-Wallis ANOVA showed significant difference between groups (p = 0.002). Post-hoc analysis by means Mann-Whitney U-tests showed that presynaptic burst AUCs differed between stable and improving patients (U-test = 75.0, p = 0.002), and between improving and worsening patients (U-test = 63.0, p = 0.006). No differences were found between stable and worsened patients (U-test = 36.0, p = 0.355).
Analysis of habituation
Statistical analysis failed to find significant differences in neurophysiological parameters between the whole population of migraine patients and healthy controls, except for the comparison between the N20 amplitude slopes across the six blocks of stimuli (Mann-Whitney U-test = 354.0, p = 0.001).
Correlation tests showed significant correlation between N20 amplitude slope and clinical index (Spearman test, rho = 0.516, p = 0.0082; see Figure 2). Conversely, no correlation was found between presynaptic HFOs’ amplitude slope and clinical index (Spearman test, rho = 0.126, p = 0.546) as well as between postsynaptic HFOs’ amplitude slope and clinical index (Spearman test, rho = 0.006, p = 0.973).
Migraine patients, clinical index plotted against N20 amplitude slope across the six blocks of stimuli. Spearman test showed a significant correlation between frequency decline of migraine attacks and amplitude increase of presynaptic HFOs.
Since N20 amplitude slope showed a significant correlation with the clinical index, we further compared clinical subgroups of patients (see Figure 3).
(a) The line-diagram shows the N20 mean amplitudes of healthy subjects and patients for each block of stimuli. Mean N20 amplitude after the first block of stimuli is slightly higher in improving patients than in worsening ones. The N20 amplitude remains stable across stimulation in improving and stable patients, while it tends to increase in worsening ones. (b) The histogram shows the mean N20 amplitude slopes of healthy subjects and patients. The average value of N20 amplitude slope is clearly negative in healthy subjects and improving patients, whereas it is positive in worsening ones.
Kruskall-Wallis ANOVA showed significant difference between groups (p = 0.026). Post-hoc analysis by Mann-Whitney U-tests showed that presynaptic burst AUCs differed between worsening and improving patients (U-test = 7.0, p = 0.006). No differences were found between stable and improving patients (U-test = 26.0, p = 0.214) and between stable and worsened patients (U-test = 17.0, p = 0.203).
Summary of neurophysiological data.
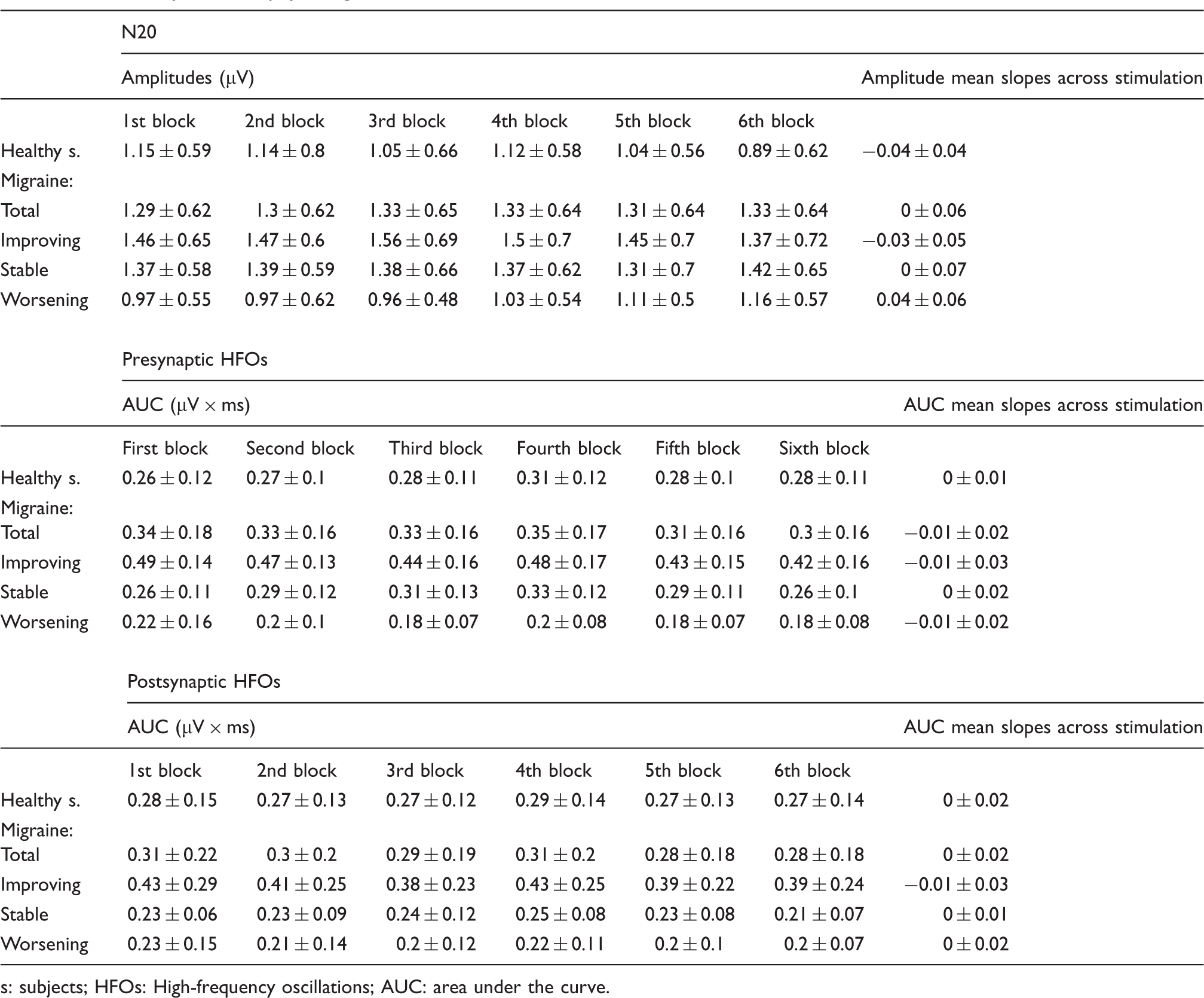
s: subjects; HFOs: High-frequency oscillations; AUC: area under the curve.
For illustrative purposes, grand averages of SEP traces in healthy subjects as well as in patients are shown in Figure 4. Before grand averaging, all traces were carried out coincident at the peak latency of the N20 potential. We performed this normalization of latencies to avoid artificial “smoothing” due to different latencies of the responses between the subjects.
Grand average of SEPs obtained from 18 healthy volunteers (top) and from improving, stable and worsening patients. P3-to-F3 recordings, wide-bandpass standard SEPs showing the N20 response on the top, narrow-bandpass (400–800 Hz) recordings showing both pre- and postsynaptic HFOs on the bottom. Black traces: first block of stimuli. Red traces: sixth block of stimuli. N20 is clearly reduced in healthy subjects at the sixth block of stimuli. Conversely, it is apparently potentiated in stable and worsening patients. HFOs do not show apparent changes between the first and the sixth block of stimuli.
Discussion
Our study confirms that migraine patients, as a whole, show a significant habituation deficit of the N20 response after repeated stimulations (3). Moreover, the analysis of our own data highlights some relevant findings, which can be summarized as follows: 1) Neither N20 amplitude nor HFO AUCs in the first block of stimuli show significant differences between healthy subjects and the whole population of migraineurs; 2) both presynaptic HFO AUC in the first block of stimuli and N20 habituation show significant correlation with clinical fluctuations occurring in the six months preceding and following the test; in particular, presynaptic HFOs in the first block of stimuli were significantly larger in spontaneously improving patients and tended to be smaller in worsening ones, whereas N20 remained stable in spontaneously improving patients and was potentiated in worsening ones; 3) whatever their amplitude in the first block of stimuli, presynaptic HFOs do not undergo habituation to repeated stimulation in controls as well as in migraine patients.
Baseline recordings: First block of stimuli
Statistical analysis failed to find any significant difference between healthy subjects and migraineurs concerning the baseline values of N20 amplitude and HFOs’ AUC. Conversely, when SEP amplitudes were further correlated to the clinical index, a strong correlation was observed for presynaptic HFOs, but not for the N20 response. The former finding has already been reported in our previous studies (27), and it is in apparent contrast with other studies, reporting abnormally low (22,23) or abnormally high (30) presynaptic HFOs in migraine; we have already suggested that the most probable reason for these apparent discrepancies could be the variable percentage of spontaneously improving or spontaneously worsening patients in previous series (27). By contrast, this cannot explain the discrepancy between data reported by Coppola et al. (31) and our own. Coppola et al. (31) noticed that N20 amplitude was smaller in migraineurs than in healthy subjects; even by hypothesizing that most of the patients studied by Coppola et al. were in a worsening phase of the disease, this should not have modified the N20 amplitude, since we did not find any significant difference in N20 amplitude between worsening and improving patients. By considering that a slight, not significant, difference was evident between the N20 mean amplitudes in improving and worsening patients also in our series (1.46 ± 0.65 µV vs 0.97 ± 0.55 µV), we cannot exclude that this slight difference might become significant in a larger sample. Moreover, patients studied by Coppola et al. (31) underwent shorter blocks of stimuli (100 stimuli instead of 500 as in our present study). Taking into account the N20 potentiation to prolonged stimulation, this could explain why the N20 was reduced in patients studied by Coppola et al. (31), but normal in our own series. However, our own data strongly suggest that modifications of the thalamocortical drive related to spontaneous clinical changes are more evident for HFOs than for standard wide-bandpass SEPs. Any possible explanation for this dissociation should take into account the different functional meaning of wide-bandpass SEPs and HFOs. Whereas low-frequency N20 is thought to reflect the whole amount of somatosensory input to the cortex, presynaptic HFOs are likely to reflect the activity of a particular pool of thalamocortical cells specifically influenced by arousal-related structures (21). It is well known that the activation of subcortical arousal-related structures can produce opposite effects on their target cells, depending on the composition of postsynaptic transmitter receptor subtypes (32). In particular, the activation of serotonergic receptors from monoaminergic nuclei inhibits glutamate release, but their effect changes to the opposite direction when the effect of γ-aminobutyric-acid B (GABAB) receptor activation is maximal, increasing glutamate release through activation of 5-hydroxytryptamine2 (5-HT2) receptors (33). It is thus conceivable that the preferential involvement of the HFO system in migraine could be interpreted as the expression of a mechanism by which monoaminergic subcortical structures tend to compensate a dysfunction of cortical excitability.
N20 habituation
Our data confirm that habituation to repeated stimulation is deficient in migraine patients as a whole. When we further correlated clinical indexes with the habituation pattern, we found that the N20 response remained substantially stable in improving patients, while it was potentiated in spontaneously worsening ones. As far as worsening patients are concerned, our data confirm the hypothesis of Schoenen et al. (11), who suggested that the hyperresponsivity of cortical neurons is mostly due to a reduction of the thalamocortical drive, which in turn causes a significant reduction of the refractoriness of the target cell. This hypothesis has found, however, further support from studies using paired-pulse protocols (28). Conversely, N20 remained substantially stable throughout the whole stimulation in improving patients. This finding, which fits well with other studies using repeated CO2-laser noxious stimulation (34) or paired-pulse stimulation (35) in improving patients, is less easy to explain and requires further speculations. Per se, the notion that improving patients do not show potentiation of the N20 response should indicate that some compensatory mechanism tends to restore the normal responsivity of cortical cells. This mechanism is clearly coupled with a significant increase of presynaptic HFOs. This suggests that the same compensatory mechanism acts via an increased influence of monoaminergic structures on thalamocortical pathways, having, as a final net result, an increase of the refractoriness of target neurons, resulting in turn in a reduction of their responsivity.
HFO habituation
HFOs do not show habituation in our healthy subjects. This finding confirms what has been already reported in an earlier paper (19), and fits well with the notion that the “somatosensory arousal system,” reflected by the HFO activity, is devoted to signal rapid and abrupt changes of the somatosensory input, the relevance of which makes desirable high synaptic efficacy (36). Taking into account the “dual-process theory” (37), effective stimuli result in two independent but interacting processes, a decremental (habituation) and an incremental one (sensitization). Both habituation and sensitization develop in separate state systems, yielding the final behavioral outcome. It is thus conceivable that the “somatosensory arousal system,” reflected by the HFO activity, might sustain the mechanism of sensitization of somatosensory input.
Interestingly, our migraine patients, independently on their clinical status, did not show any habituation of both presynaptic and postsynaptic HFOs, analogously to our control subjects. In principle, this finding strongly indicates that the HFO system responds physiologically to repeated stimulations. Therefore, it is conceivable that the abnormalities of baseline HFOs we observed in our patients could represent different expressions of a single buffer mechanism, rather than a primary dysfunction of the HFO system. We have already hypothesized that the HFO increase noticed in improving patients could reflect a compensatory mechanism, devoted to reduce the responsiveness of cortical neurons by increasing their refractoriness. By contrast, the HFO reduction as well as the N20 potentiation after repeated stimulation can be interpreted as the expression of the same buffer mechanism in a particular condition of very low serotonin availability. A considerable bulk of data (38–41) suggests that serotonergic disposition reaches its minima during preictal stages and increases during the attacks. It is thus conceivable that in our worsening patients serotonergic disposition tends to progressively decrease: This progressively lower serotonergic disposition could determine reduced thalamocortical activity that in turn decreases the amplitude of presynaptic HFOs and explains the N20 potentiation after repeated stimulations. For instance, the same mechanism has been claimed to explain the reduction of the refractory period of neurons in the somatosensory cortex in worsening migraineurs (28).
Conclusions of the study
Our data confirm that reduced preactivation level of sensory cortices due to inefficient thalamocortical drive plays a major role in the pathophysiology of migraine (38). Moreover, in this study we demonstrated that spontaneous clinical fluctuations of migraine can be assessed by means of simple neurophysiological techniques. In our study, because of large interindividual variations, results and conclusions apply to the group of migraine subjects, not to individuals. However, the prolonged neurophysiological follow-up of migraine patient groups by means of simple techniques, together with the clinical observation, could be useful for the clinician researcher to objectively assess the evolution of the disease.
Clinical implications
Our data confirm that reduced preactivation level of sensory cortices due to inefficient thalamocortical drive plays a major role in the pathophysiology of migraine. Spontaneous clinical fluctuations of migraine can be assessed by means of simple neurophysiological techniques, such as N20 recording after repeated stimulation. The follow-up of migraine patient groups by means of habituation studies could be useful, together with the clinical observation, to objectively assess the evolution of the disease.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.