
Abstract
Introduction
Headache is the most common adverse event immediately following craniotomy and is due to the surgical procedure and meningeal irritation.
Objectives
The aim of this study was to investigate the prevalence of headache during the first week after a craniotomy, as well as headache intensity, whether pain was registered in the patient's medical records, the use of analgesics and predictors of headache.
Methods
Ninety-one patients who underwent craniotomy were evaluated from the first to the seventh post-operative day. The variables analysed were gender, age, medical history, indication for craniotomy, surgery, occurrence of headache, pain registration in the medical records, length of hospital stay and analgesics consumption.
Results
On the second post-operative day, 29.2% of patients had a headache and there was under-reporting of this pain in the patients’ records. The analgesics used were non-steroidal anti-inflammatory in 75% of cases. An age of <45 years (odds ratio = 3.0, p = 0.041) and surgery duration lasting >4 hours (odds ratio = 3.7, p = 0.019) were associated with the occurrence of immediate post-craniotomy headache.
Conclusion
Further training should be provided to professionals caring for patients undergoing craniotomy to better manage post-operative headache.
Keywords
Introduction
Craniotomy is indicated for traumatic brain injury, brain tumours, aneurysms and arteriovenous malformations. In general, the technique involves creating an opening in the skull to access the meninges and brain mass (1). As a result of the surgical procedure, many patients experience headache episodes in the post-operative period, with an incidence ranging from 5% to 91% (2,3).
According to the International Headache Society (IHS) (4), the definitive diagnosis of post-craniotomy headache (ICHD-II 5.7) depends on the onset of pain within 7 days after surgery, which can be of variable intensity. In addition, the craniotomy should have been performed for a reason other than brain trauma. The classification of pain as acute (ICDHD-II 5.7.1 G44.880) or chronic (ICDH-II 5.7.2 G44.30) depends on its duration and has a 3 month post-craniotomy period as a cut-off point (4).
Although an immediate headache is not included as a diagnostic subtype, the IHS reports that up to 80% (4) of patients experience episodes of headache in the first hours after craniotomy and this symptom improves during the first post-operative week in most cases. The present study is motivated by the current limitations in the understanding of immediate post-craniotomy headache and, in particular, its occurrence, characterisation, pain management and factors that predict its onset.
The lack of brain tissue sensitivity due to the absence of nociceptors in its parenchyma, and innervation virtually limited to the meninges and extracranial muscles and fascia, has led to the belief that patients would experience minimal pain following craniotomy. Therefore, the use of post-operative analgesics has received little attention (5). However, two-thirds of patients experience moderate to severe pain post-craniotomy, especially in the first 48 hours after surgery (6). Therefore, adequate pain control is an important matter for the patient and health care provider.
Although the pathophysiological mechanisms of headache after craniotomy need to be elucidated, inflammation and meningeal fibrosis, compression and entrapment of nerves and the formation of traumatic neuromas are thought to be commonly associated factors (7). Surgical incision and other adverse perioperative events can also induce changes in central neural function through phenomena such as sensitisation and wind-up, which contribute to the pathogenesis of the post-operative pain (8–10).
This study aimed to investigate headache prevalence immediately after craniotomy (up to 1 week post operation), headache pain intensity, the incidence of pain registration in the medical records, the prescription of analgesics and the factors associated with the occurrence of headaches.
Methods
Study design
Between September 2010 and October 2011, a prospective study was conducted with patients undergoing elective craniotomy in the Neurology Sector of the Charitable Hospital Foundation for Surgery, Sergipe, Brazil.
Participants
A total of 91 patients were included. Patients with less than 15 points on the Glasgow Coma Scale (GCS) at the time of evaluation, victims of traumatic brain injury, patients who subsequently died and patients aged <18 years were excluded from the study. All patients gave informed consent before being enrolled in the study. Study approval was obtained from the Committee for Ethics in Medical Research of the Federal University of Sergipe.
Variables
Document analysis and semi-structured interviews were used to collect data, including demographic variables, medical history, indication for craniotomy, surgery, duration of hospital stay, occurrence of headache, registry of pain in their medical records and consumption of analgesics.
Diagnosis of immediate post-craniotomy headache
For the diagnosis of immediate post-craniotomy headache, the following IHS criteria were used: headache of variable intensity with maximum intensity in the area of the craniotomy; craniotomy performed for a reason other than head trauma; the headache must have occurred within 7 days after the craniotomy.
The intensity of the headache was analysed by means of a 0–10 numerical rating scale and categorised according to the International Association for the Study of Pain (IASP; 11): no pain = 0; mild pain = 1–3; moderate pain = 4–7; severe pain = 8–10.
Setting
In accordance with the local protocol, all patients received nerve block anaesthesia and 10 mg morphine i.v. bolus during the perioperative period. As this drug can have satisfactory analgesic effects up to 24 hours after its administration in craniotomy cases (12), the patients were evaluated every day from the first 24 hours (day 1) until the seventh day (day 7) of post-operative care or hospital discharge.
Data collection occurred before the patients underwent the craniotomy. These patients were also monitored in the first 24 hours post-surgery (day 1) and until the seventh day after the craniotomy (day 7), unless the patient was discharged before day 7. The presence of headaches and their intensity were investigated.
Assessment of analgesic consumption
The prescription of analgesics (non-steroidal anti-inflammatory drugs (NSAIDs), weak opioids and strong opioids) was recorded at all times during the study (days 1–7). For those patients who received analgesic medication, we evaluated the intensity of the headache before and after 1 hour of medication administration. For patients who received no pain medication, a period of 1 hour was also adopted as the standard for reassessing the severity of the headache.
Statistical methods
Data were stored in the OriginPro 8.0 SRO® software (OriginLab Corporation, Northampton, MA, USA) for the analysis of descriptive (frequency, measures of central tendency and dispersion) and inferential statistics. Point prevalence was used as a measure of the proportion of people in the study who had a headache at a particular time and took into consideration the number of patients diagnosed with headache and the total number of patients hospitalised at the time of evaluation.
Pain intensity comparison before and after the use of analgesics was performed using a one-sided paired t-test. Pain reduction at the time of reassessment between the patients who received analgesics and those who did not was performed by one way analysis of variance. A Fisher's exact test was used to detect differences between patients treated with analgesics and untreated patients at day 1. A p-value <0.05 was deemed to be statistically significant.
A multiple logistic regression model was developed to determine factors that could explain the presence of immediate post-craniotomy headache. The logistic regression model used was taken from epidemiological studies and, in this case, the binary response was the presence or absence of a headache and the predictive variables were the risk factors and possible confounding variables (13). The following pre-specified variables were selected as potential predictors for immediate post-craniotomy headache: gender; age (>45 years or ≤45 years); presence of preoperative pain (yes or no); use of preoperative analgesic (yes or no); indication for craniotomy, surgical approach (infratentorial or supratentorial); surgery duration (>4 hours or ≤4 hours). Variables with a p-value <0.25 in the univariable logistic regression were retained for adjustment and the final model was found by a backward selection of predictor variables, as described by Hosmer and Lemeshow (13). At each step, the variable providing the highest p-value was deleted from the model. Variables were kept in the final model if the p-value was <0.05.
Results
A total of 116 patients were eligible for the study. However, 25 participants were excluded due to death (n = 2), by showing less than 15 points in the GCS (n = 17) or because they were aged <18 years (n = 6). The final cohort consisted of 91 patients, 56 women and 35 men. Ages ranged from 18 to 69 years, with an average of 44.8 years. A total of 63.8% of patients had no history of systemic disease, 27.5% had a history of hypertension, 5.5% had diabetes mellitus, 2.2% had both those diseases and 1% had heart disease. In more than half of the cases (60.4%), the craniotomies were performed due to the presence of a brain tumour and 39.6% were due to a non-ruptured aneurysm. The supratentorial surgical approach was performed in 91.2% of the cases and the majority of surgeries lasted between 3 and 4 hours (3.5 ± 2.8 hours). A total of 86 patients were admitted to the Intensive Care Unit (ICU), with a mean stay of 2.8 days. The total average hospital stay was 16.5 days. No patient had a post-operative infection.
The data show that, among the 91 patients who participated in the study, some patients could not be monitored over the entire follow-up period because they were discharged from the hospital before the end of the study. On day 2 and day 3, four patients were discharged; on day 4 and day 5, 16 patients were discharged; on day 6 and day 7, 29 patients were discharged (Figures 1 and 2).
Point prevalence of immediate post-craniotomy headache. Grey bars indicate the number of patients on each day of evaluation. The loss of follow-up refers to the number of hospital discharges in each period. Registration of pain in the medical records of patients with immediate post-craniotomy headache and analgesic usage.

Preoperative pain
Variables associated with preoperative pain in the head region of patients undergoing elective craniotomy.
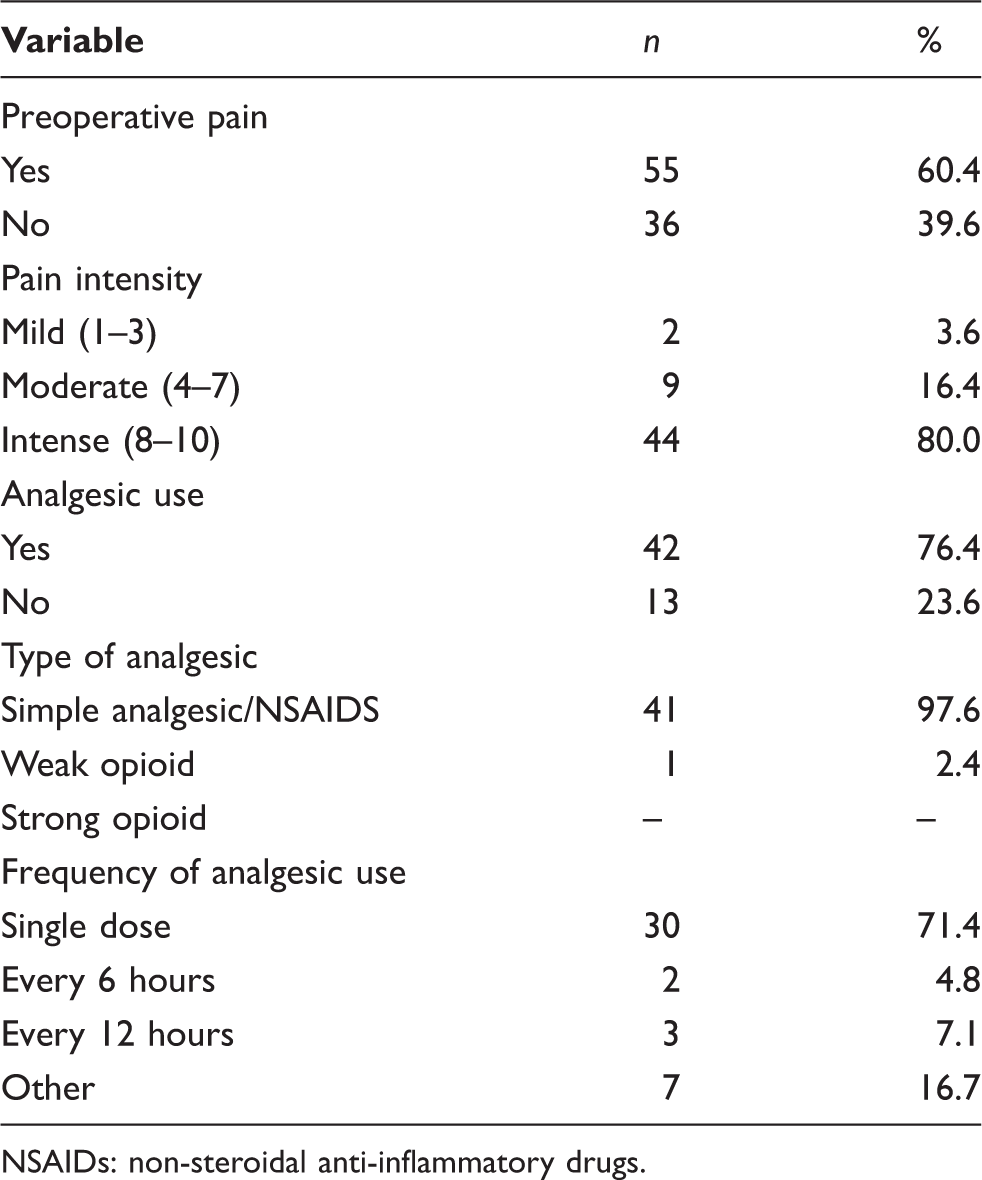
NSAIDs: non-steroidal anti-inflammatory drugs.
It is important to emphasise that the preoperative headaches reported by the patients were progressive; they were worse in the morning and were aggravated by coughing and forward tilting of the head. Furthermore, all the patients were diagnosed with neoplasia on the basis of the results of the imaging studies. All of the patients used corticosteroids in the pre-and post-operative periods. These observations are consistent with the criteria established by the IHS (4) regarding the classification of Headache Attributed Directly to Neoplasm.
In 80% of cases, the headache was severe and the vast majority used NSAIDS for pain control. The majority of patients (76.4%) took analgesics only when they felt pain (Table 1).
Prevalence of immediate post-craniotomy headache and pain registration
Of the patients who underwent elective craniotomy, 24.2% had a headache at the first evaluation (day 1). The headache prevalence did not vary significantly over time, but was slightly higher on day 2 (29.2%) and slightly lower on day 5 (14.1%; Figure 1). The post-craniotomy headache was recorded if it was continuous and interfered with the patient's daily activities; there was no report of nausea, vomiting or visual changes. Although headache is a frequent complaint in the first post-surgical days, it is commonly under-reported in patient medical records (Figure 2).
Post-surgery analgesic consumption
Characteristics of patients with headache with and without the use of post-operative analgesics at the first evaluation (day 1).
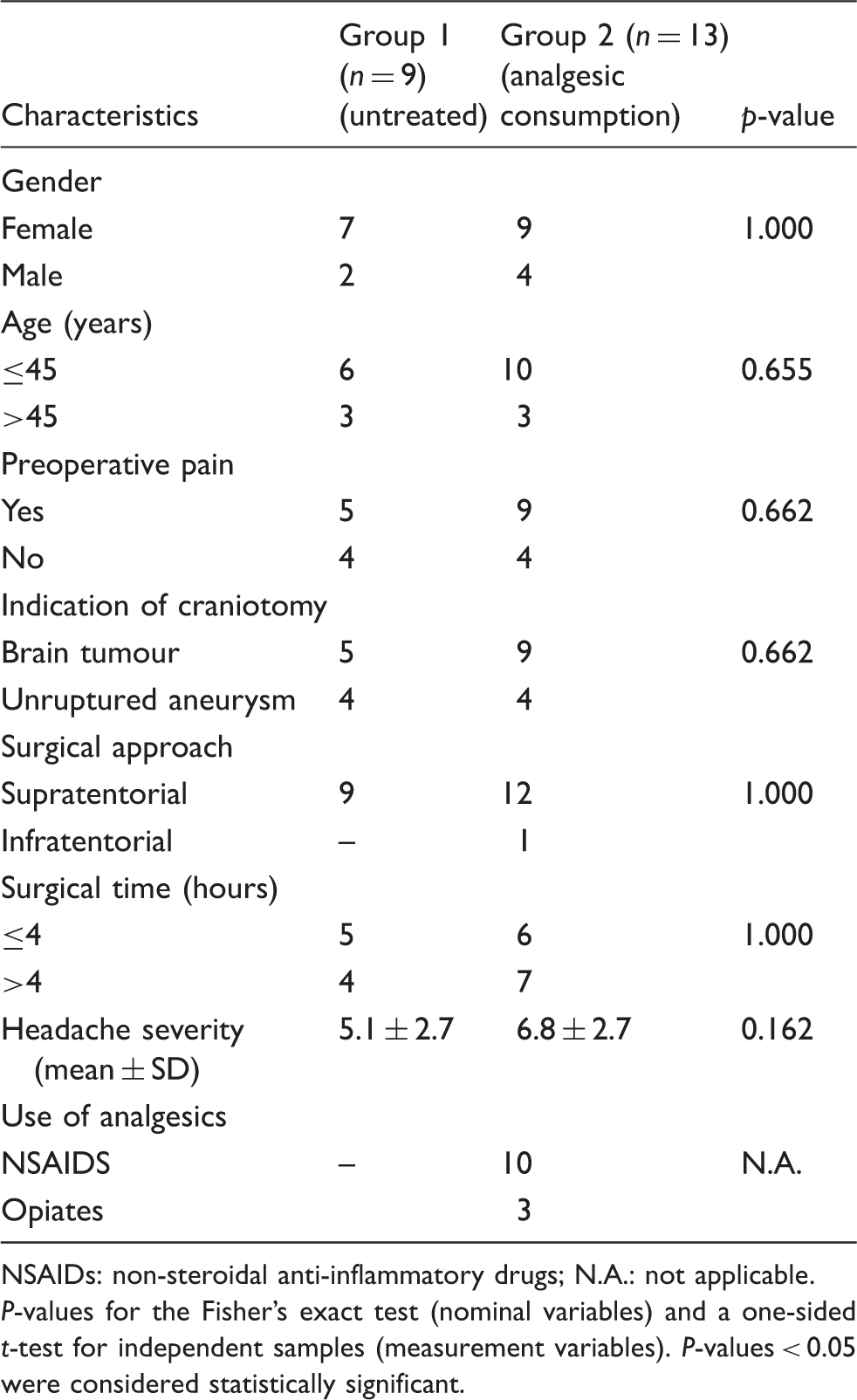
NSAIDs: non-steroidal anti-inflammatory drugs; N.A.: not applicable.
P-values for the Fisher's exact test (nominal variables) and a one-sided t-test for independent samples (measurement variables). P-values < 0.05 were considered statistically significant.
Intra-group comparison of headache intensity at the time of assessment and reassessment.

Group 1: patients who did not use analgesic medication; Group 2: patients who used analgesic medication.
P-values were calculated using one-sided paired t-tests. P-values < 0.05 were considered statistically significant.
Pain intensity: no pain = 0; mild pain = 1-3; moderate pain = 4-7; severe pain = 8-10.
Pain reduction between groups at the time of reassessment.

Group 1: patients who did not use analgesic medication; Group 2: patients who made use of analgesic medication.
P-value for the one way analysis of variance. P-values < 0.05 were considered statistically significant.
Pain intensity: no pain = 0; mild pain = 1-3; moderate pain = 4-7; severe pain = 8-10.
However, when comparing the average pain intensity between the groups at the time of reassessment, there was no statistical significant difference at any time (Table 4). A possible explanation for this is that the majority of patients used NSAIDS (75%) for the study period. In 25% of cases, weak opioids were prescribed to patients with headache. In these cases, the intensity of pain was notably lower than in the group of untreated patients (day 1: 2.5 ± 2.7 vs. 5.1 ± 2.7; day 2: 1.0 ± 1.4 vs. 4.1 ± 1.8; day 3: 2.5 ± 2.7 vs. 5.5 ± 2.4; days 4 and 5: no patients were treated with opiates; day 6: 2.0 ± 0.0 vs. 3.4 ± 2.5; day 7: 2.0 ± 0.0 vs. 2.5 ± 0.0); however, no statistical tests were performed because a very small number of patients used opiates.
Univariate and multiple logistic regression analysis
Univariate analysis of potential predictors of immediate post-craniotomy headache.

Odds ratio (OR) for potential predictors and 95% confidence interval (CI).
Variables associated with immediate post-craniotomy headache in univariate analysis with p < 0.25.
Backward selection.

R: coefficient of determination; F: coefficient calculated by the Fisher-Snedecor distribution.
Variables with p-values < 0.05 were considered statistically significant and included in the final logistic regression model.
Final logistic regression model.

Odds ratio (OR) for covariates and 95% confidence interval (CI).
P-values < 0.05 were considered statistically significant.
P = 0.008.
Discussion
The point prevalence of immediate post-craniotomy headache ranged from 14.1% to 29.2%. These data differ from the results of the IHS, in which 80% of the patients had headaches (4) and 40% (14) of patients who underwent craniotomy had a headache in the first 24 hours. These differences in headache prevalence may be due to our patients receiving 10 mg of morphine and scalp block during the perioperative period. The use of these medications may have contributed to the reduction in headache occurrence during the post-operative period.
The scalp nerve block by infiltration of anaesthetics decreases the persistence of post-operative pain and allows the early recovery of neurosurgical patients (15). Other studies have shown that the infiltration of the scalp with anaesthetics, associated with the use of dipyrone during the post-operative period, decreased the intensity of pain in the first 12 hours post-surgery, contributing to the well-being and haemodynamic stability of patients and thereby allowing an early hospital discharge (16,17).
Data from this research show that 80% of patients had severe headache in the preoperative period. Although the great majority of patients presented with severe headache in the preoperative period, none of the patients used strong opioids for pain control. Opioid analgesics are the main intervention for pain control in hospitalised patients, especially for moderate to intense pain (18).
Severe pain is common in hospitalised patients, who may suffer unnecessarily due to delays in the administration of analgesics that are not always effective (19). Untreated acute pain causes neurovegetative changes, worsening clinical signs and physical and psychological suffering in patients.
A proportion of patients had a moderate intensity headache. Our data are in agreement with a previous study (15), in which the surgical approach was supratentorial and patients also complained of post-surgical headache. After completion of the craniotomy, the presence of headache that follows both surgical manipulation and meningeal irritation is common. ‘The post-surgical intracranial pain is often intense, unassessed and not appropriately treated’ (20,21).
The majority of the patients in this study were admitted to the ICU. Patients hospitalised in this sector are often suffering from pain and another severe symptom (22). After completion of the craniotomy, patients were transferred to the ICU to stabilise their haemodynamic status. As there are health professionals on continuous shifts in the ICU, it should be an optimal environment to adequately treat pain; however, this did not always occur, possibly due to a view that the higher pain scores occurred in the first post-surgery days.
Data from this survey indicate that there were few pain complaint registries in the records of patients. The under-reporting of pain via registration in the patient's medical records may reflect the care provided to patients undergoing craniotomy. This pain needs to be recorded in a systematic manner in order to be adequately treated. Adequate pain evaluation and management should be viewed as inalienable patient rights; however, the findings of this study show that pain management may be suboptimal given that on the seventh day after surgery some patients still had a headache.
A total of 30% of patients did not receive any type of analgesic medication, although they complained of a headache. The use of analgesia in the post-operative period of craniotomy remains a concern and there is controversy between neurosurgeons. Despite the effectiveness of opioids in reducing post-operative pain, many surgeons are still reluctant to prescribe these medicines. This may be driven by a concern that opioid effects will mask the signs of intracranial complications and by a pre-established bias that the pain after craniotomy is minimal (20). Other studies have shown, in contrast with the present study, that until the seventh post-surgical day, some of the patients complained of headache (20).
The therapeutic success for pain control is based on the correlation between the pain mechanism and the effect of the drug used; however, our data contradict the World Health Organization (WHO, which advocates (23) the use of an analgesic ladder for the choice of an appropriate therapeutic treatment. The WHO analgesic ladder indicates the use of weak and strong opioids to treat moderate and strong pain intensity, respectively; opioids are used in conjunction with non-opioid analgesics or NSAIDS and adjuvant drugs in the former.
We noted a statistically significant difference between the first and second assessment of headache. Conversely, there was no statistically significant difference in further reassessments. These data suggest that, although analgesics decreased pain intensity, they were not sufficient for complete headache relief. It is important to highlight that there was also pain reduction in the group of patients who did not use analgesics. The possible explanation for the pain persisting in the group of patients treated with analgesics was related to the medical diagnosis before the surgery and the duration of the operation being >4 hours. The low use of opioids for moderate pain may also have contributed to the persistence of the painful phenomenon in this group of patients.
The lack of strong opioid prescriptions for pain relief may have contributed to headache persistence in these groups of patients. Among the opioids, morphine is considered the standard medication for the treatment of acute and chronic pain. This is because morphine has a high efficacy for the treatment of moderate and intense pain and, unlike NSAIDS and mixed opioids, it does not have a dosage ceiling (24,25).
In the post-craniotomy period, headache may become a problem when not appropriately treated and systematised by the multi-disciplinary team. Health professionals must consider that pain is an experience that is unique to each person and that to assess and treat a patient's pain assistance should be based on scientific principles, technical training and attitude, which are the three forming competence factors.
To reduce post-craniotomy headache intensity, health professionals need to be aware of the importance of proper pain management, multi-disciplinary team participation, analgesia protocols, specialised teams and the creation of services for acute pain with appropriate quality assistance. Although pain is considered as the fifth vital sign, there are still health professionals who do not value the pain process assessment and, consequently, inadequate pain treatment continues to be a clinical problem in hospitalised patients (19,26,27).
The final logistic regression model indicated that an age of <45 years was associated with the occurrence of headache in the post-operative period. Individuals with advanced age are thought to experience lower pain intensity than young adults due to neurobiological alteration of nociceptors that occurs with the ageing process. The changes that occur in pain perception in elderly people are not clearly elucidated, but a nociception model in animals has shown, via electrical stimulation of repetitive afferent fibres, that the receiving properties of afferent terminals and conduction membranes of the axon are altered with age, suggesting that the elderly feel less pain than young adults (28).
Multiple logistic regression also indicated that a surgery time of >4 hours increases the likelihood of post-surgical headache. Post-operative pain, in general, is almost always proportional to the degree of stimulation of free nerve endings, the surgical incision, tissue trauma and surgical duration. Hence, there appears to be greater tissue injury with increases in the duration of surgery (29,30).
A limitation of our study is that patients were not specifically assessed for a history of pre-existing primary headache, which has been recognised as a risk factor both for brain tumour-associated headache and for post-craniotomy headache (31,32).
We conclude that a proportion of patients who underwent elective craniotomy had a headache, but this was of moderate intensity for the majority of patients. Furthermore, the pain was under-reported in the patient's medical records. The analgesia used in the post-operative period was not sufficient for pain relief. Health professionals should pay particular attention to patients aged <45 years and whose surgery lasts >4 hours, as these patients are more likely to have painful post-craniotomy headaches. These data highlight the need for investment in the training of professionals who assist patients undergoing craniotomy and the need to create protocols for analgesia and systematic pain assessment.
Footnotes
Clinical implications
Further training should be provided to professionals caring for patients undergoing craniotomy to better manage post-operative headache.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sector.
Conflict of interest
None declared.