
Abstract
Seventy-nine patients with intracranial aneurysms were evaluated in the presurgical period, and followed up to 6 months after surgery. We compare patients who fulfilled with those that did not post-craniotomy headache (PCH) diagnostic criteria, according to the International Classification of Headache Disorders. Semistructured interviews, headache diaries, Short Form-36 and McGill Pain Questionnaire were used. Seventy-two patients (91%) had headaches during the follow-up period. The incidence of PCH according to the International Headache Society diagnostic criteria was 40%. Age, sex, type of surgery, temporomandibular disorder, vasospasm, presence and type of previous headaches, and subarachnoid haemorrhage were not related to headache classification. There were no differences in the quality of life, headache frequency and characteristics or pain intensity between patients with headache that fulfilled or not PCH criteria. We proposed a revision of the diagnostic criteria for PCH, extending the headache outset after surgery from 7 to 30 days, and including the presence of headaches after surgery in patients with no past history of headaches, or an increase in headache frequency during the first 30 days of the postsurgical period followed by a decrease over time. Using these criteria we would classify 65% of our patients as having PCH.
Introduction
The presence of post-craniotomy headaches (PCH) often interfere with patients' quality of life (1–5) and constitute a challenge for those who deal with them (6). Only recently has scientific interest increased concerning this type of headache (7).
The incidence of PCH is highly variable (0–75%), most of the studies showing values > 40% (1–3,8–17). This variability is probably due to the lack of uniform diagnostic criteria and the retrospective nature of most of the reports in the literature.
There is some evidence that PCH incidence may vary according to the surgical technique. Headache incidence is higher in those with craniectomy than in those with craniotomy with bone flap replacement (13,18) or with cranioplasty (19,20). Patients operated for vestibular schwannoma using the suboccipital approach had a higher PCH incidence than those with the translabyrinthine approach (2,9). Notwithstanding, a prospective study that followed up patients only for 48 h after the surgery found no difference in headache incidence between the surgical routes (21).
Patients with preoperative headache also seem to have a higher PCH incidence (9,22,23). The role played by age (9,15,21) and sex (9,23,24) is controversial.
Post-craniotomy headache diagnostic criteria according to the International Headache Society (25)

The objective of this study was to compare patients submitted to craniotomy for treatment of intracranial aneurysms who fulfilled PCH diagnostic criteria according to the IHS (25) with those that did not in order to evaluate its usefulness. We proposed a modification of the criteria used for PCH diagnosis and classified our study group accordingly.
Subjects and methods
From October 2002 to October 2003, all patients hospitalized in our institution for surgical treatment of supratentorial intracranial aneurysms were selected if they had a Glasgow coma scale score of 15 at the time of evaluation. Patients with central nervous system infections were excluded.
All patients were interviewed and examined by the same neurologist at the surgical ward during the presurgical period, and at 15 days, 2, 4 and 6 months after surgery, at the out-patient clinic. The neurological examination included sensory testing of the skin at the operation area. Headache frequency was monitored with a headache diary, during follow-up. On the fourth month of follow-up, the Brazilian version of the McGill Pain Questionnaire (MPQ) (26) and Short Form (SF)-36 quality of life generic questionnaire (27) were completed.
The diagnosis of PCH was based on the IHS criteria (25).
Patients were evaluated at the Orofacial Pain Clinic of our hospital with the objective of identifying temporomandibular disorder (TMD). The masticatory and neck muscles and their insertions were palpated at this evaluation. The diagnosis of TMD was based on the IHS criteria, except for item D, ‘headache resolves within 3 months after the treatment’, because these patients were evaluated only once (25).
All the patients gave informed consent and the study was approved by the Ethics Committee of our institution.
Data are presented as mean and S.D. or as frequency and percentage. Categorical variables were compared across groups using Fisher's exact test or χ2 test for trend for ordered categories. Continuous variables were compared across groups using Student's t-test.
The analysis of the MPQ was based on the pain rating index (PRI) based on the descriptive scores and on the number of words chosen (NWC). This analysis was made by the questionnaire as a whole and by the four subscales.
We compared the results of the MPQ between the patients who fulfilled the criteria for PCH and the others (with and without headache in the diary) and SF-36 questionnaires of the patients who fulfilled the criteria for PCH and the others who matched headaches in the diary (25). This distinction was made because some patients matched some descriptors on MPQ, but did not interpret this as pain and did not match the headache diary. Statistical analysis was performed using the Mann–Whitney non-parametric test.
A multivariate logistic regression model, with a stepwise selection process, was used to study the presence of PCH criteria, according to the IHS, among the patients who had headaches in the postsurgical period. The initial variables selected in the model in a stepwise process were: age, sex, type of surgery, presence of TMD, type of previous headache (migrainous or non-migrainous), presence of subarachnoid haemorrhage (SAH), previous primary headache, presence of vasospasm, no headache in the 3-month period before surgery vs. presence of headache in the 3 months before surgery vs. no primary headache.
Significance level was established at 0.05 (5%).
Statistical analysis was carried out with
Results
Seventy-nine patients were included, 65% female, with a mean age of 45.3 years. Four patients were lost to follow-up before answering the questionnaires.
Forty-nine patients had headache during the 3 months before surgery, five of whom had chronic daily headache.
Seventy-two (91%) of 79 patients had headaches anytime during the follow-up period. Thirty patients (40%) [95% confidence interval (CI) 27.3, 49.3] fulfilled the IHS diagnostic criteria of PCH, 73% (22/30) of these of the chronic type. The incidence was 41% (21/51) in women and 32% (9/28) in men.
Sixty per cent (47/79) of the patients had headache outset within 7 days and 82% (65/79) within 30 days after craniotomy. Forty-four patients (56%) had pain on the site of the craniotomy at any time during the follow-up period.
Fourteen patients (19.5%) developed headache after 7 days in the postsurgical period, out of 72 patients who had headache after surgery, 24% (17/72) experienced pain outside the craniotomy area and 15% (11/72) both.
Of the 11 patients with no past history of headache, nine had headache in the postsurgical period. Four did not fulfill the IHS criteria, two because pain was localized outside the surgical area, and two because the time of onset occurred after the first week in the postsurgical period.
General characteristics of the study group, according to whether or not they fulfilled the International Headache Society diagnostic criteria for post-craniotomy headache (PCH)
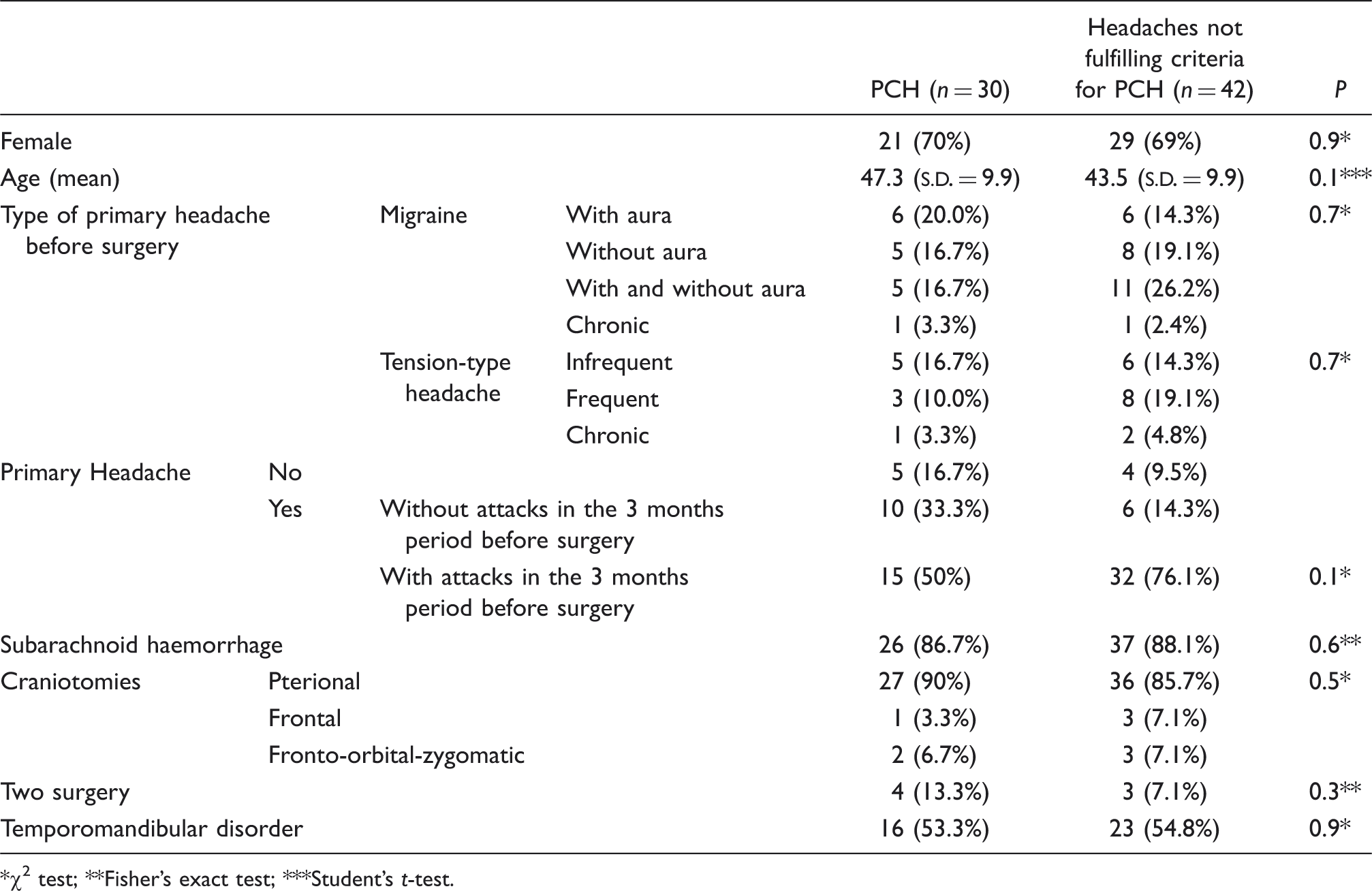
χ2 test; **Fisher's exact test; ***Student's t-test.
None of the variables included in the logistic regression model was found to be important to explain the presence of the IHS diagnostic criteria for PCH.
Figure 1 shows the headache frequency comparing patients with PCH with those not fulfilling the IHS criteria during the follow-up period. We observed the same behaviour in both groups with an initial increase in mean headache frequency followed by a decrease over time.
Headache frequency comparing patients with post-craniotomy headache (PCH) with other headaches not fulfilling the International Headache Society criteria (Non-PCH) during the follow-up period.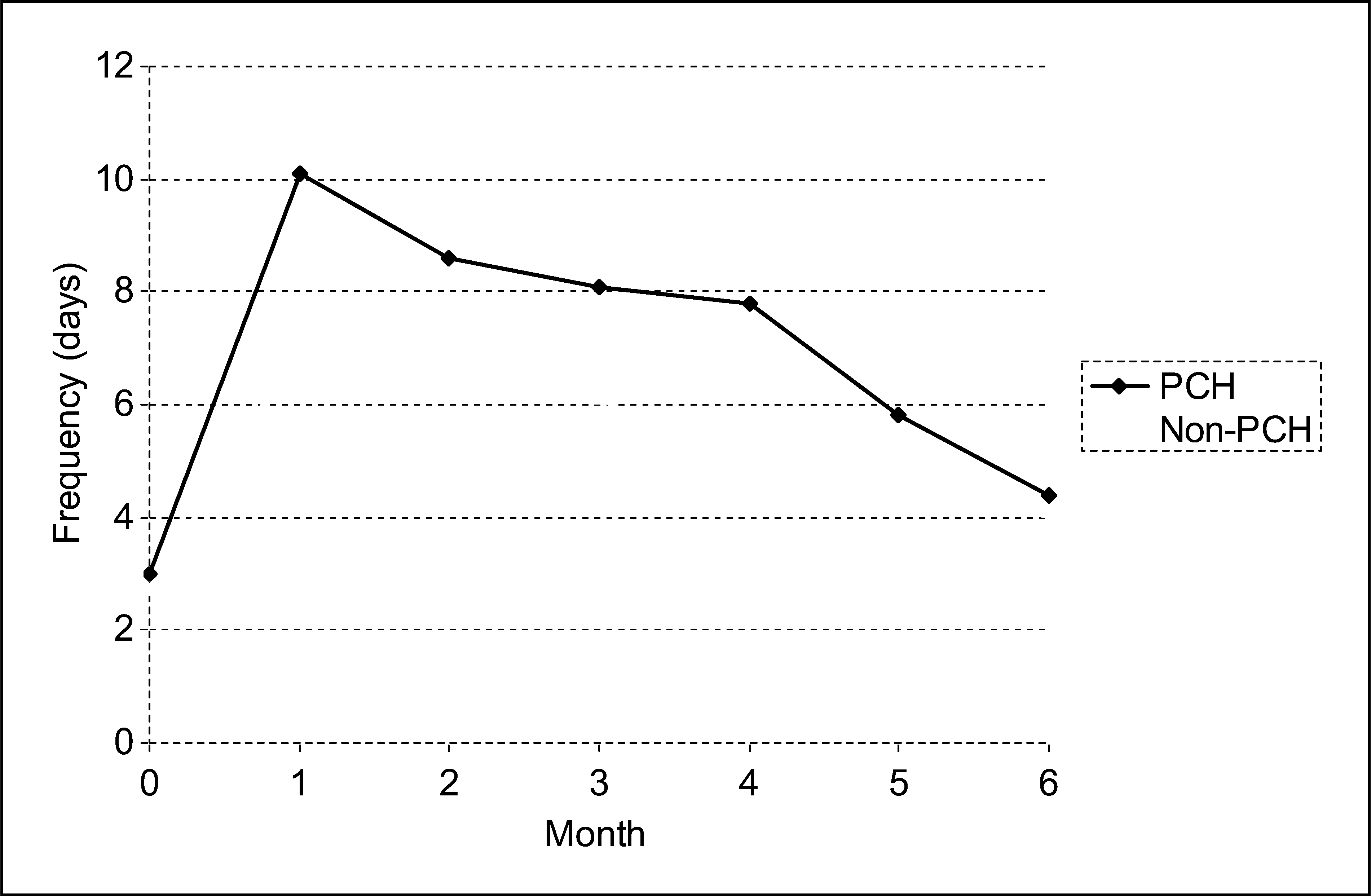
Number of words chosen (NWC) and pain rating index (PRI) of the McGill questionnaire subscales results between the patients with post-craniotomy headache (PCH) and other headaches not fulfilling the International Headache Society (IHS) criteria for PCH diagnosis
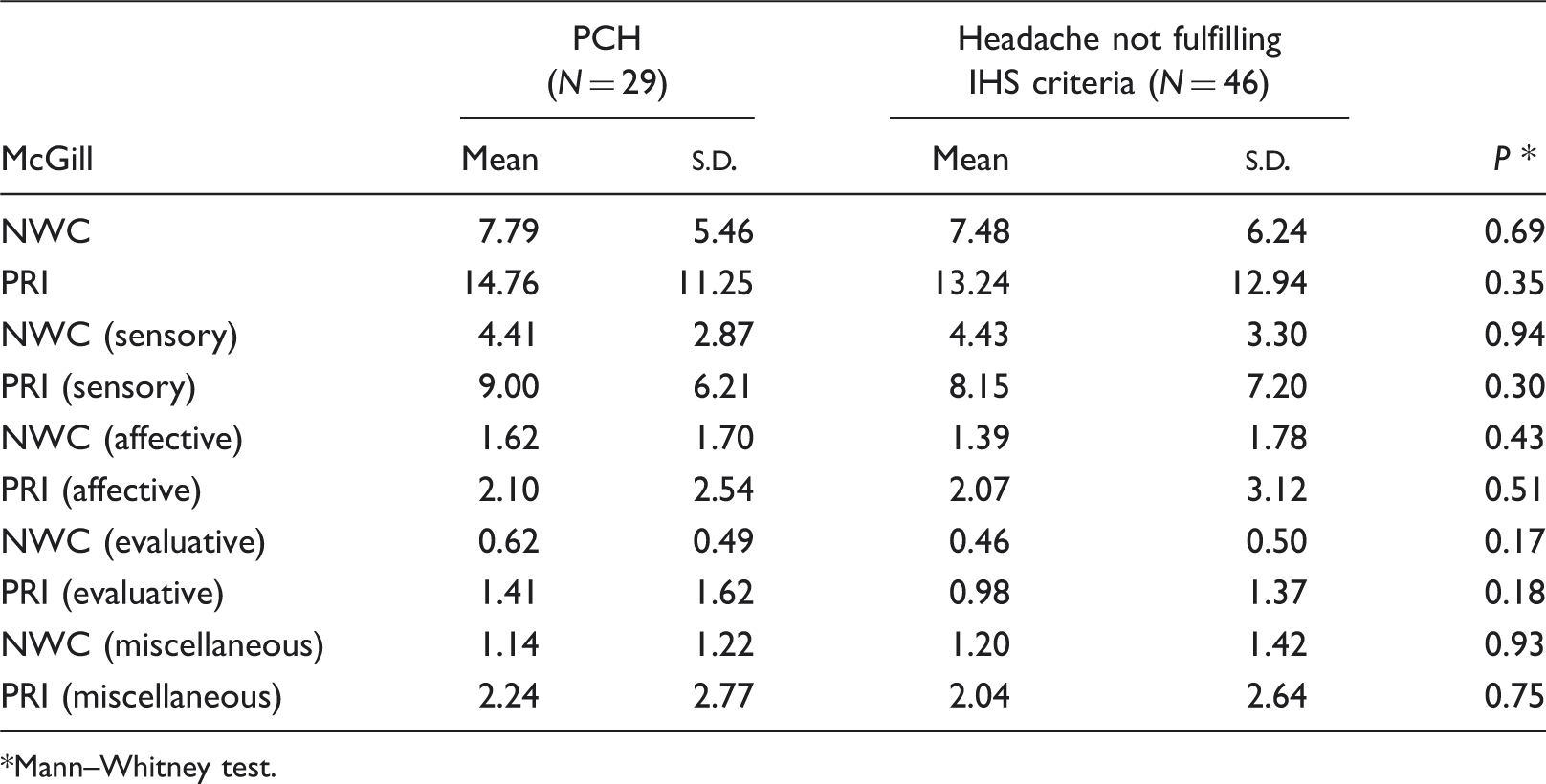
Mann–Whitney test.
Short Form (SF)-36 quality of life questionnaire results comparing patients with post-craniotomy headache (PCH) and other headaches not fulfilling the International Headache Society (IHS) criteria

Mann–Whitney test.
Patients with postsurgical headache had a mean of 8.5 painful craniocervical muscles on palpation (S.D. = 6.0), and a mean of 14.9 tender points (S.D. = 11.7). There was no statistically significant difference in the number of painful muscles (Mann–Whitney; P = 0.6) or in the number of tender points (Mann–Whitney; P = 0.7) between patients with PCH and those with headaches not fulfilling the IHS criteria.
If we consider the patients without previous headache together with those that had a different headache pattern any time during the follow-up period, they would represent 61% (44/62) of the patients that experienced headache after craniotomy.
Proposed diagnostic criteria for post-craniotomy headache (PCH) diagnosis
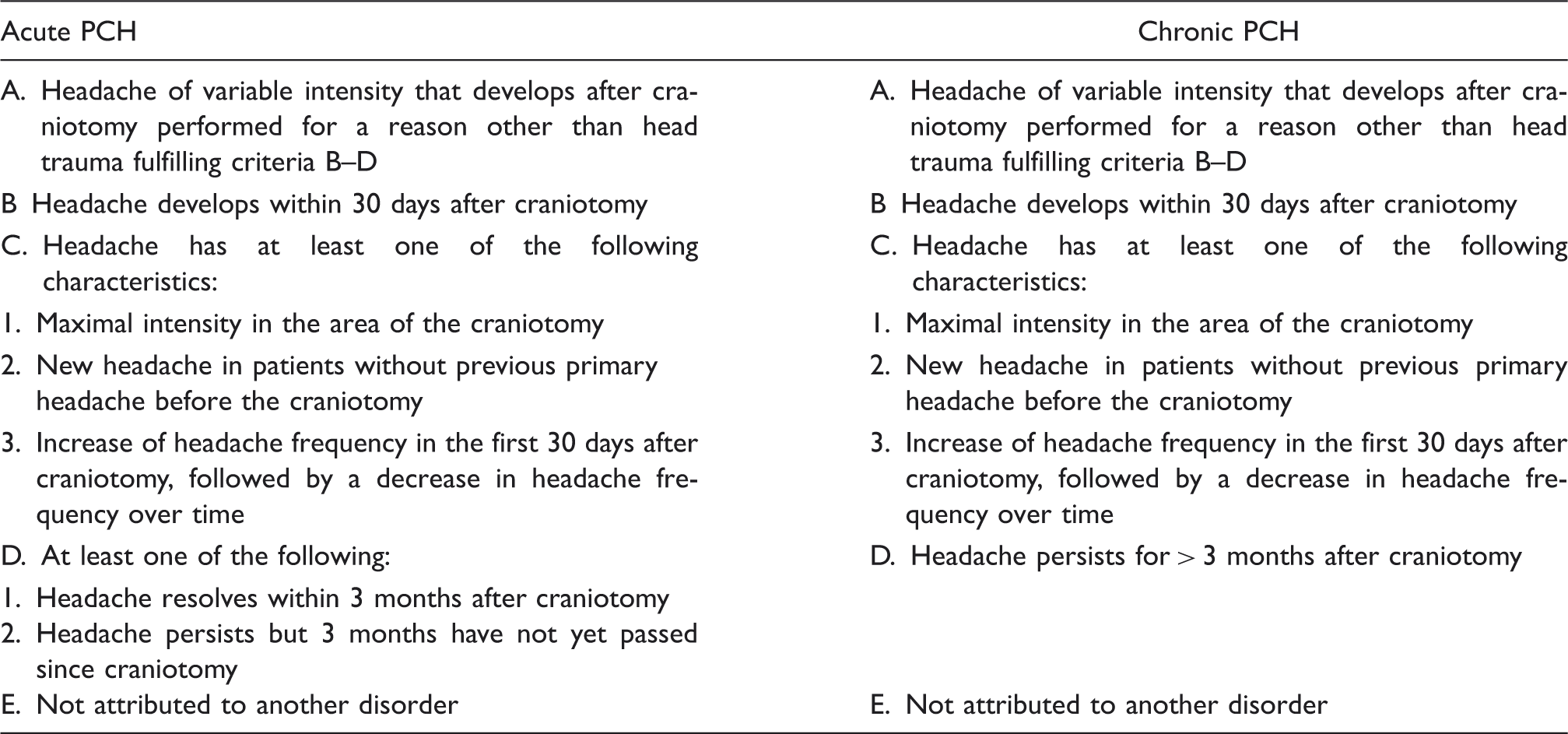
Using the revised criteria, 49 (65%) patients (95% CI 50.4, 72.7) would be classified as having PCH, 17 of the acute, and 32 of the chronic type. All patients without previous headache who had headache after surgery would fulfil the revised criteria.
Of 63 patients who had headache before and after craniotomy, 56% had a different pattern of headache any time during the follow-up period. The revised criteria would classify 71% of them as PCH, compared with 49% if the IHS diagnostic criteria are used.
Discussion
Few studies in the literature have evaluated the interval between surgical procedure and headache outset. According to these studies, pain began in the immediate postsurgical period in 70–90% of patients and after the first month in 10–20% (3,24). We observed that in 68% of our patients, headache outset occurred up to 7 days after surgery and that this figure would rise to 93% if the period was extended to 30 days after surgery, considering only patients who had headaches in the craniotomy area during the follow-up period (5).
According to the concept that a secondary headache should develop in strict temporal relation to its underlying disturbance, a cutting point of 7 days after surgery for headache development in PCH is reasonable. However, it is also arbitrary, based on little previous empirical evidence in the literature. The fact that two out of nine of our patients (22%) without previous headache developed headaches > 7 days from the craniotomy suggests that 7 days is perhaps too small a period of time for PCH diagnosis.
The PCH are usually located on the same side of the craniotomy (9,24), frequently on the surgical scar (1–3,14,20,21,24,28,29), but some may occur with maximal intensity, and in places outside the surgical area (1,3,9,14,15,21,24,28,29). Our previous study showed that 35% of patients with headache after craniotomy localized pain outside the surgical area. (5) A recent retrospective study showed that among patients who had headaches that began in the first week after surgery, 40% had a diffuse (bilateral) headache pattern. Fourteen per cent of the patients had headaches predominantly on the opposite side to the surgery. The authors suggested that the classification should be revised to include bilateral headaches, headaches contralateral to the craniotomy side, and headaches with maximal intensity outside the craniotomy area (23). The fact that almost half (4/9) of our patients without previous headache developed headaches outside the craniotomy site clearly shows that pain with maximal intensity in the area of the craniotomy is not an obligatory fact in patients with PCH.
Our study showed that in 61% of patients that experienced headaches in the postsurgical period the attacks could not be explained by their previous primary headaches (patients without previous headaches and patients with different headache patterns any time during the follow-up period). Notwithstanding this finding, the IHS diagnostic criteria classified only 38% of these patients as having PCH.
We observed no difference concerning headache frequency, headache intensity (MPQ), muscle pain or quality of life between patients classified or not as PCH by IHS criteria.
Others have reported that pre-operative headaches (9,22,23), age (21), sex (23) and TMD were associated with PCH (30). We have not found such relationships.
Our results show that craniotomy often causes headache, but the current classification is not able to distinguish the various headache types observed in these patients. Based on these findings, we suggested a modification of the diagnostic criteria for PCH. The modified diagnostic criteria take into account the major characteristics of PCH.
Temporal relationship between craniotomy and headache outset in the postoperative period was extended from 7 to 30 days.
Pain localization may be outside the craniotomy area.
We added increase in headache frequency in relationship with craniotomy followed by decrease over time, which is in accordance with the general instructions for secondary headaches of the International Classification of Headache Disorders, 2nd edn (25). When a primary headache becomes worse in close temporal relation to the occurrence of another disorder that could be a cause of headache, patients could receive two diagnoses, the primary headache diagnosis and the secondary headache diagnosis. The decrease of headache frequency over time is in accordance with the general rule that headache should be greatly reduced after ‘spontaneous remission’ of the causative disorder.
Other conditions associated with neurosurgical procedures such as infections, intracranial haematoma, hydrocephalus and low cerebrospinal fluid can cause headaches and should be ruled out based on patient history, physical and neurological examination, and by appropriate investigations (criterion ‘E’).
The modified diagnostic criteria increased the number of patients classified as having PCH, including all the patients without previous headache and maintaining the predominance of chronic PCH, which seems to be a characteristic of this kind of headache. We believe that these modifications will improve the identification of patients who develop secondary headaches that are directly related to the trigger factor being considered here, i.e. craniotomy.