
Abstract
Wilfred Harris was a London neurologist with a significant interest in the treatment of neuralgia. Harris' descriptions of what he called migrainous neuralgia were the first recorded of cluster headache in the English medical literature. He was probably one of the first to describe the cluster phenomenon itself and the effectiveness of ergotamine in treating acute attacks of cluster headache. His seminal contributions to the clinical and therapeutic spectrum of cluster headache are reviewed.
Introduction
The publications by Bayard T. Horton (Fig. 1) of the Mayo Clinic were instrumental in the general recognition of cluster headache (1). The 1939 clinical description by Horton and colleagues (2) was comprehensive, except for the omission of Horner's syndrome and the male predominance of the disorder. In a later article, Horton (3) noted both the male predominance and the frequent association with Horner's syndrome. He was aware of, but did not fully appreciate, the remitting nature of cluster headache. It is this flaw that most likely led to the claims of the effectiveness of histamine desensitization. Regardless, he made the plight of cluster headache sufferers known. He was one of the first to report the usefulness of oxygen (3), ergotamine (4), dihydroergotamine (5), and corticosteroids (6) in the treatment of cluster headache.

Photograph of Bayard T. Horton.
It is clear that Horton was familiar with the older literature on the subject of headache. In his seminal article from 1941, Horton (4) commented that some patients could relieve their head pain by compressing the ipsilateral common carotid or temporal artery, and he quoted an article from 1792 touting the effectiveness of arterial compression in alleviating head pain. Later in the same article, he mentioned Edward Liveing and his classic book On Megrim and Sick-Headache, and Some Allied Disorders: A Contribution to the Pathology of Nerve-storms when discussing the relationship of alcohol use and headache. Horton was unaware of the earlier descriptions of cluster headache and commented that ‘the syndrome had not been described adequately in the literature’ (4). This statement does a disservice to Wilfred Harris (Fig. 2), whose case reports of migrainous neuralgia were the first recorded reports of cluster headache in the English medical literature (7).

Photograph of Wilfred Harris.
Background
Wilfred John Harris was born on 2 December 1869, in Madras, where his father, who was in the Indian Medical Service, was a professor of midwifery and the diseases of women and children (8). He graduated in 1894 from Cambridge and St Mary's Hospital in London. After house appointments at St Mary's Hospital and obtaining the London MRCP in 1896, he spent 2 years as a resident at the National Hospital, Queen Square.
He proceeded to obtain an MD in 1898. He then returned to St Mary's Hospital, where he became first medical registrar and then medical tutor. In 1902 he was appointed Registrar and Assistant Physician to the Maida Vale Hospital for the Paralysed and Epileptic. In 1905 he was appointed Assistant Physician and Physician to Outpatients at St Mary's Hospital and was elected FRCP. In 1907 he became Lecturer of Neurology and established a department of neurology at St Mary's Hospital, the first in any undergraduate teaching hospital. In 1933 he became the first president of the Association of British Neurologists. He retired in 1935 but returned to St Mary's Hospital to take charge of the Neurological Department for a time during the Second World War. It is recorded that he was ‘a man seemingly without fear who positively enjoyed being a warden during some of the worst air raids’ (9). He ultimately retired in 1945, at age 75. He died on 28 February 1960, at age 90.
He was renowned as a teacher and demanded much of his students and junior staff. Macdonald Critchley, who met Harris in 1923 when Critchley became a resident at Maida Vale, commented that Harris ‘was, perhaps quick-tempered … but never … obnoxious or unpleasant’, and when the two played tennis together, Harris ‘certainly became cross when he served a double fault’ (8). Critchley stated that he had ‘many pleasant memories of Wilfred Harris [and] always held him in affection and great admiration’ (8).
Harris wrote more than 200 papers and several books. Two of his books, Neuritis and Neuralgia in 1926 (10) and The Facial Neuralgias in 1937 (11), covered the topic of migrainous neuralgia, later to be recognized as cluster headache. His last book was published in 1939 and was entitled The Morphology of the Brachial Plexus With a Note on the Pectoral Muscle and Its Tendon Twist (12). This book was the result of more than 40 years of work at the London Zoo Prosectorium. He investigated the different forms of the brachial plexus in all varieties of animals, including toads, crocodiles, hummingbirds, a giant panda, monkeys, and several others. He also examined 26 adult and four fetal plexuses. In this book, Harris described and appreciated the importance of the prefixed and post-fixed plexus (8).
Harris was the first to suggest the possibility of injecting alcohol directly into the ganglion without a surgical incision for the treatment of trigeminal neuralgia (13). He perfected the technique required by injecting hundreds of cadavers with methylene blue, and he was so adept at the procedure that he flew to South Africa in his 80s to inject a patient (8). He was one of the first to inject the ganglion in a live patient, although the first procedure was probably done by Taptas (14). Harris appears to have planned and performed the procedure, whereas Taptas first did it ‘accidentally’ during a planned alcohol injection of the mandibular division at the foramen ovale (14). This accidental trigeminal ganglion injection appears to have predated Harris' first injection (14). Taptas did subsequently perform the procedure intentionally (14). In addition to contributing significantly to the treatment of trigeminal neuralgia, Harris is credited as being the first to recognize glossopharyngeal neuralgia as a distinct pain syndrome (15).
Harris' concept of migrainous neuralgia
In his 1926 book Neuritis and Neuralgia, Harris (10) described migrainous neuralgia in general and then discussed subdivisions of this general diagnosis. These subdivisions included migrainous supraorbital neuralgia, periodic migrainous neuralgia, and ciliary neuralgia. He noted that some patients with migrainous neuralgia had a history of migraine, with the migrainous neuralgia substituting for the typical migraine attacks. In general, he stated that the attacks occurred at frequent intervals, such as once in 2–3 weeks up to three to four in a week. In a few cases, he noted that patients with pain in the temple or in the cheek had attacks lasting an hour or less, repeated three to four times per day for years. He differentiated the pain of migrainous neuralgia from trigeminal neuralgia (Table 1) and migraine proper (Table 2). When discussing ‘general’ migrainous neuralgia and supraorbital neuralgia, Harris appears to have included cases that we would now classify as migraine without aura, chronic migraine, or atypical facial pain.
Harris' concept of migrainous neuralgia compared with trigeminal neuralgia
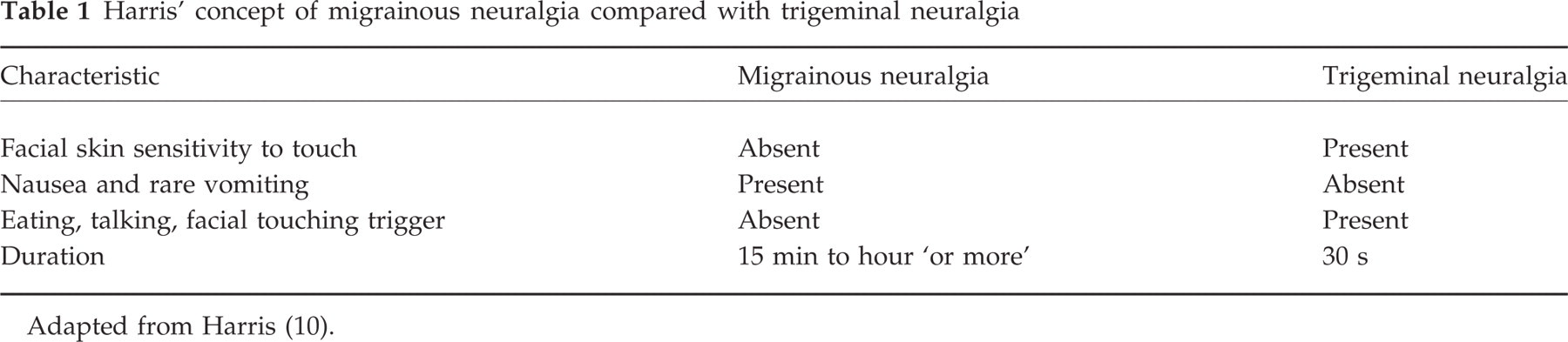
Adapted from Harris (10).
Harris' concept of migrainous neuralgia compared with migraine
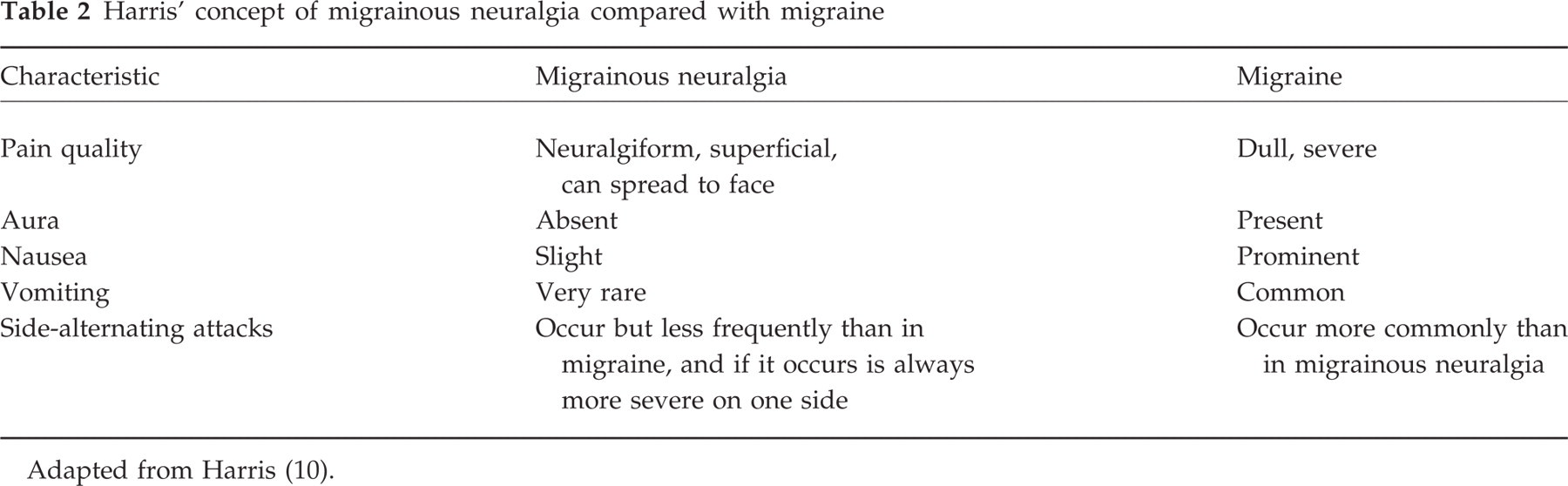
Adapted from Harris (10).
In 1936, Harris (16) clarified his concept of migrainous neuralgia as follows.
I have employed the term ‘migrainous neuralgia’ to describe cases of recurrent neuralgia affecting the temple or the side of the forehead and often both jaws, sometimes extending to the back of the head, usually strictly unilateral. The pain in these cases is often most intense and excruciating, and may start suddenly or gradually and subside in the same way, the duration of the pain varying from ten minutes to half an hour, or often for five or six hours and occasionally twenty-four to thirty hours. In the attacks of brief duration there may be three or more recurrences every twenty-four hours for periods of six to eight weeks yearly. Nausea occasionally accompanies the pain, thus suggesting its association with migraine, but vomiting is rare, and visual spectra and transient hemianopia are never met with as in the usual form of migraine (p. 457).
Periodic migrainous neuralgia
When describing periodic migrainous neuralgia in his 1926 text, Harris (10) noted that the attacks ‘may occur daily for weeks on end and then disappear for many months.’ He later reiterated that attacks ‘may occur daily at about the same time and last for several hours for a period of a few weeks only in the year, and may recur annually at about the same time.’ He described the duration of attacks as occasionally being 10–60 min, but he stated that in most cases the duration was ‘several hours.’ When the attacks were of short duration, Harris noted that they might recur several times within 24 h. He commented that most patients had side-alternating attacks, but that even then the more severe attacks were always on one particular side; in some cases the attacks were on one side only. The pain was ‘likened to a knife being driven in through a point between the outer canthus of the eye and the hair line’, and was associated with scalp sensitivity. In this section, Harris discussed a case that we would now probably classify as migraine without aura. He also reviewed several cases that meet duration and frequency criteria for cluster headache, but autonomic features were not mentioned. One case (10) does meet International Headache Society (IHS) criteria, and the patient appears to be have suffered side-alternating attacks.
A young man of 25, when aged 19 began to suffer from daily attacks, for three or four weeks every year, of severe pain in the back of the right eyeball and forehead, with lachrymation and reddening of the eye; this would last for an hour or two, no nausea, but voracious appetite accompanying the neuralgia. During the last two years he had had similar attacks of pain behind the left eyeball, and they would then transfer and become severe on the right side. He had never been subject to sick headaches, but his mother suffered from periodic headaches and was neurotic, and his eldest brother was neurasthenic (p. 305).
Another man (10) is described who would not meet IHS criteria, because autonomic features are not mentioned, but who clearly displays clustering.
In 1907 I saw a man, age 44, who every year since he was 17 years old had suffered for some weeks in the autumn from neuralgia affecting the right temple. Usually he was awakened about 3 a.m., the pain appearing to start quite suddenly as a sharp stabbing in the temple behind the outer canthus of the eye. The pain appeared to throb slowly, though not with the pulse, and became so severe that he said he was almost crazy with it and could not stand without staggering. The attacks lasted two or three hours, and often the neuralgia disappeared quite suddenly, though sometimes a very severe attack would make him vomit, after which the pain ceased. On some occasions he had two or three attacks in one day, and he was also subject to occasional left-sided sick headache, though he said the pain in that form was quite different and not so intense (pp. 303–304).
Harris described the cluster phenomenon but less clearly than Ekbom (17) and Kunkle et al. (18). The two patients in the periodic migrainous neuralgia section of Harris' 1926 book who either fit or are closest to fitting the IHS criteria were both men. In a 1940 article, he (19) described a woman with what appears to be episodic cluster headache. ‘A married woman, aged 46, seen in April, 1911. Had suffered from spasms of neuralgia in head since the age of 16, always in [the] summer. Pain began gradually outside [the] right eyebrow and spread across [the] eye, which became blood-red; pain stabbing for 3/4 h. Might have several attacks in a night’ (p. 482).
Ciliary neuralgia and Horner's syndrome
In his 1926 text, Harris (10) discussed ciliary neuralgia as migrainous neuralgia with pain localized to the orbital or retro-orbital region. A previous writer has inferred that Harris was not aware of the occurrence of Horner's syndrome in cluster headache (1), whereas others have stated correctly that he was one of the first to note this sign in this particular variety of headache (20). A case report from his classic book Neuritis and Neuralgia (10) clarifies this issue.
A man, age 47, had his first attack of neuralgia in January 1917, when in the trenches in front of Beaumont Hamel. The pain struck him suddenly across the left temple and forehead, and lasted for three-quarters of an hour, like an ‘electric battery’, while his face became flushed and he felt faint. The neuralgia recurred thrice daily, at about eight hour intervals for six weeks, and then disappeared entirely for two years. Ever since his first attack he had left cervical sympathetic paralysis, there being slight ptosis, with a small pupil. In subsequent attacks the neuralgia began on the left side of the top of the head, the eyeball being very painful and red, and the pain spreading down the nose into the left side of the cheek. The second attack lasted for six weeks, while his third attack did not occur until three years later, the pain awaking him shortly before 5 a.m. His face became sore during the attack, but there were no physical signs except the sympathetic palsy referred to (pp. 307–308).
It is not clear why Harris would choose the name ciliary neuralgia to refer to migrainous neuralgia centred on the eye, as he commented that ‘this could not have been an inflammatory lesion of the ciliary ganglion as the pupil would then have been dilated from paralysis of the constrictor pupillae’ (10). He explained that he used the term ‘ciliary’‘more for descriptive purposes than with any certainty of … pathology.’ Again in this section he described some cases that we would today probably classify as migraine or atypical facial pain. He ended his discussion of ciliary neuralgia in his 1926 book (10) with the following brief case of cluster headache in a 51-year-old man.
The first attack occurred quite suddenly in the left eyeball and around the eye, with lachrymation, and occurred daily in the evening for about three-quarters of an hour for four months. The pain then disappeared for nearly three years, when daily recurrences took place after considerable worries due to the War. Infra-orbital nerve injection broke the sequence of attacks, which soon disappeared and afterwards he was quite well for some years (p. 312).
In 1936, Harris clarified the clinical spectrum of ciliary neuralgia (16). He stated that the pain of ciliary neuralgia was localized within or behind the eye and was associated in many cases with conjunctival injection and lacrimation. He commented that eight of his 23 patients had the onset of headache between age 40 and 50 years and that the onset of pain was ‘commonly in the early hours after midnight’ (16). Ten of his 23 patients noted conjunctival congestion and injection as well as lacrimation.
Harris' concept of sympathetic headache
Harris discussed the concept of sympathetic neuralgic headache in The Facial Neuralgias (11) as well as in two journal articles (16, 21). Sympathetic headache or hemicrania was ‘recurrent at more or less regular intervals’ (16), with or without nausea, and the pain could spread to the back of the head and neck. The attacks were associated with sympathetic phenomena, such as profuse unilateral sweating of the forehead and temple, congestion of the eye, lacrimation, and nasal congestion. Sympathetic headache was relieved by stellate ganglionectomy, whereas migrainous neuralgia was relieved by gasserian ganglion injection, and thus the two were believed to have different mechanisms. Harris believed that there were certain forms of afferent sensation along sympathetic pathways and noted that stimulation of the superior cervical ganglion could produce pain in the face (21). He thought that the sympathetic afferent path was normally latent and unused but was capable in certain pathologic states of being a source of pain. Harris (11) described a patient with trigeminal neuralgia who had a gasserian ganglion destruction procedure, but who had persistent pain in the temple that was cured with stellate ganglionectomy.
In three separate publications (11, 16, 21), Harris cited two patients who had recurrent hemicrania associated with autonomic features and relieved by stellate ganglionectomy who were reported in 1935 by Craig (22), a neurosurgeon at the Mayo Clinic. The second patient described in Craig's paper suffered from cluster headache and was described as such in Horton's 1941 article (case 5) (4). This patient's relief by sympathectomy appears to have represented a spontaneous remission. Of interest, Craig was the third author on the classic 1939 paper by Horton et al. (2).
Harris separated migrainous neuralgia from sympathetic headache, but he mentioned that sympathetic headache could be difficult to distinguish from migrainous neuralgia. In describing this difficulty, Harris mentioned a case of Walter Dandy that was published in 1931 (23). Dandy thoroughly presented a patient with episodic cluster headache who would fit today's IHS criteria. The patient underwent stellate and inferior cervical sympathetic ganglionectomies and was headache-free for 6.5 months after the procedure. Dandy acknowledged that the follow-up period was too short to permit an unreserved opinion concerning the value of the procedure.
Aetiology of migrainous neuralgia
Harris believed migrainous neuralgia was a substituted or anterior form of migraine. He thought that migrainous neuralgia was probably associated with a vasomotor spasm affecting the anterior region of the meninges (he later specified the middle meningeal artery), thus causing referred pain over areas of the trigeminal nerve through recurrent meningeal branches of the three divisions of this nerve (16). To Harris (10), ciliary neuralgia was the result of a ‘spasmodic vasomotor neurosis rather than due to local disease of any ganglion or nervous structure.’ He reasoned that visual aura was unusual in migrainous neuralgia because the vasomotor spasm did not affect the posterior cerebral arteries.
Treatment of migrainous neuralgia
Harris was the first to suggest injection of alcohol in the gasserian ganglion as therapy for particularly severe cases of migrainous neuralgia (24). He was aware that this was not always successful, but he noted that ‘certain picked cases undoubtedly may be … cured’ (16). In 1940 he (19) reported that of the 29 patients he had injected, 19 were completely cured and five were much improved. In the remaining five, the attacks returned, although they were less violent. He postulated that the injection worked by blocking the recurrent meningeal trigeminal branches, thereby obstructing the afferent path of the painful impulses triggered by the vasomotor changes in the meningeal vessels (16). Otherwise, Harris (10) recommended luminal (phenobarbital, phenobarbitone). When describing the therapy for migrainous neuralgia in his 1937 book The Facial Neuralgias, Harris (11) commented that the ‘treatment of the acute attacks by subcutaneous injections of ergotamine tartrate (Femergin) 0.5 mg, usually aborts the attack speedily.’
Discussion
Wilfred Harris described many of the key features of what we now call cluster headache, including the typical unilaterality, severity, brevity, frequency, and autonomic features. He recognized that Horner's syndrome could occur in cluster headache. He was probably the first to describe the cluster phenomenon itself. He was also the first to comment on the effectiveness of ergotamine in treating acute attacks of migrainous neuralgia. Horton is usually given credit for first using ergotamine in the treatment of cluster headache (25). Horton's 1941 article contained a description of a patient seen at the Mayo Clinic in September 1937 who was successfully treated with ergotamine (4). However, Harris' comment concerning ergotamine was published in 1937 (11). As such, priority should be given to Harris. Harris was the first to use trigeminal ganglion injection for the treatment of migrainous neuralgia or cluster headache. He therefore influenced the subsequent development of ablative procedures directed at destruction of the trigeminal afferent pathway, which are used today in certain refractory cases of cluster headache.
Although Harris quoted the work by Craig, a Mayo Clinic neurosurgeon, concerning headache (11, 16, 21), he himself was never awarded a similar courtesy by Horton. Later Mayo Clinic physicians did recognize Harris' seminal contribution. Rooke, Rushton, and Peters (26) quite clearly stated that ‘when Horton and his associates at the [Mayo] Clinic described this headache in 1939, they were actually redescribing a syndrome about which Harris had written in 1926 and again in 1936 under the terms “ciliary” or “migrainous” neuralgia.’
There were some flaws in Harris' concept of migrainous neuralgia. The term itself is misleading, given that cluster headache is neither truly migrainous nor neuralgiform. Although the frequency of migraine may be slightly higher in the cluster headache population than in the general population given the higher male-to-female ratio seen in cluster headache (1), the two are believed to be separate pathophysiological entities. However, this concept became generally accepted only in the 1970s after landmark reviews by Ekbom (27) and Lance and Anthony (7). Horton himself thought that the two diseases were separate, although it took his colleagues and time to convince him of this. Some of the cases that made up his 1939 paper were first presented at the staff meetings of the Mayo Clinic in March 1938 as unusual cases of migraine (28). After this unpublished presentation, his colleagues commented that what he was describing did not seem to be a migrainous phenomenon (28). It was only after this that he developed the notion that cluster and migraine were separate diseases, a point he defended from his original publication in 1939 onward.
There were flaws also in Harris' case descriptions. When describing migrainous neuralgia, he included some cases that we would today classify as migraine without aura, chronic migraine, or atypical facial pain. In comparison, Horton presented a homogeneous group of patients, which may explain why he is often recognized for giving the definitive description of cluster headache. Perhaps because of Harris' tendency to be a ‘lumper’ rather than a ‘splitter’, he missed the male predominance of cluster headache, because migraine and atypical face pain have a high female-to-male ratio (29, 30). The migrainous neuralgia patients described by Harris who are closest to fitting today's IHS cluster headache criteria are primarily men.
When describing periodic migrainous neuralgia, Harris (10) stated that ‘in the majority the pain may attack either side’, and that the attack duration was usually several hours. This prevalence of side-alternating attacks would be higher than the 16% rate accepted today (31), and a usual duration of ‘several hours’ would be longer than the mean usual attack duration of 1 h quoted in Kudrow's large series (32). Perhaps the contamination of his cluster headache cases with migraine increased Harris' notion of what the usual duration and side-alternating attack frequency of migrainous neuralgia were. When describing migrainous neuralgia in 1940, he (19) made the following comment.
The duration and frequency of the attacks [vary] much. Some patients suffer daily for a month or six weeks every year, while in others the attacks at first may be at intervals of weeks and gradually become more common until they occur three or four times a week, lasting most of the day and entirely crippling the patient's activities. The duration of the individual attacks also varies widely, lasting 24–48 h in some, and as short a time as 10 min in others (p. 481).
One could hypothesize that the patients with longer lasting attacks occurring at ‘intervals of weeks’ had migraine, and the patients with daily, frequent, short-duration attacks occurring in bouts had cluster headache.
Harris did not recognize that sympathetic headache and migrainous neuralgia were the same disease, a point that seems obvious with hindsight. He also did not recognize that sympathectomies had no clear role in the treatment of primary headache. White and Smithwick (33) subsequently showed that blocking the stellate ganglion during an attack of migraine did not produce relief, and Rowbotham (34) tried cervicothoracic sympathetic ganglionectomy in 20 patients who had migraine and reported unsatisfactory results. Horton (28) thought that cluster headache was a medical and not a surgical problem, and commented that sympathectomy gave unsatisfactory results.
Previous authors have outlined the historical development of the concept of cluster headache (1, 7, 17, 25, 35). The purpose of this paper was to point out the significant contributions of Wilfred Harris to our current understanding of cluster headache, not to diminish the importance of Bayard Horton's contribution. As Sjaastad (1) states, both men deserve praise for revealing this entity to the medical world.