
Abstract
We prospectively studied headache characteristics during 6 months after craniotomy performed for treatment of cerebral aneurysms in 79 patients. Semistructured interviews, headache diaries, the Hospital Anxiety and Depression Scale and the Epworth Sleepiness Scales, the Short Form-36 Health Survey (SF-36) and McGill Pain Questionnaire were used. Seventy-two patients had headaches, half before the fifth day after surgery. Changes were observed in headache diagnosis, side and site in the postoperative period. Headache frequency increased immediately after surgery and then decreased over time. Headache frequency was associated with depressive and anxiety symptoms. Pain intensity was higher in women and in patients with more anxiety symptoms. An incidence of post-craniotomy headache of 40± was observed according to International Headache Society classification criteria, 10.7± of the acute and 29.3± of the chronic type. The bodily pain domain of the SF-36 was worse in patients with more anxiety symptoms. Greater frequencies of headache were associated with lower scores on bodily pain and social functioning.
Introduction
Post-craniotomy headache (PCH) is recognized as a separate entity in the new International Headache Society (IHS) classification (1). The literature on PCH is based mainly on retrospective studies, a fact that hampers the establishment of a causal relationship between surgery and headache, and a better evaluation of headache characteristics and their temporal pattern. Most studies lack information concerning previous headache characteristics; therefore, it is not clear whether headaches observed in the postoperative period are of a new kind or are previous headaches that have been exacerbated by the surgical procedure.
PCH prevalence figures shows a high rate of variation, a fact probably related to underlying disorders, their retrospective nature, and use of different PCH definitions.
PCH prevalence varies at between 0 and 50% in retrospective studies of patients who had vestibular neurectomies performed for treatment of vertigo (2–5).
There are few studies of PCH after supratentorial neurosurgery. Gee et al., in a retrospective study, have reported a PCH incidence of 19% after craniotomies performed for treatment of several diseases such as brain tumours, epilepsy and intracranial haemorrhage (6). Kaur et al. have reported an incidence of 17.5% of headaches that persisted for > 2 months and of 11.9% for > 1 year after temporal lobectomy for the treatment of epilepsy, considering only headaches with pain localized on the injury site, or headaches of a different type from those of the preoperative period (7).
PCH starts immediately after the surgical procedure in 70–90% of the patients and in 10–20% after ≥ 1 month (8, 9). Pain site is usually on the same side as the craniotomy (9, 10), frequently on the surgical scar (6, 8, 9, 11–16). Pain characteristics are frequently similar to those of tension-type headache (8, 11, 13, 17) and are often different from the headaches reported before surgery (14). PCH prevalence (5, 12, 13, 17–20) and intensity (8, 13) decrease over time.
The objective of our study was to evaluate prospectively PCH characteristics, evolution and effect on the quality of the life of patients who had had craniotomies performed for treatment of cerebral aneurysms.
Methods
Between October 2002 and October 2003, all patients operated for treatment of supratentorial cerebral aneurysms and with a Glasgow coma scale of 15 during the study period were included.
All patients gave informed consent and the study was approved by the hospital Ethics Committee. In the preoperative period, in the hospital ward, data were recorded concerning the presence of previous primary headaches, their characteristics, frequency in the last 3 months based on the patient's recall, and presence of headache related to subarachnoid haemorrhage (SAH).
During follow-up, patients were seen after a mean of 2 weeks (stitches withdrawal, visit 0), 60 (visit 1), 120 (visit 2) and 180 (visit 3) days after surgery. A headache diary was used to record the frequency and characteristics of the PCH and the records were evaluated at each visit.
The incidence of PCH was established according to diagnostic criteria of IHS (Table 1) (1).
Diagnostic criteria for post-craniotomy headache diagnosis according to the International Headache Society (1)

The Hospital Anxiety and Depression Scale (HADS) (21) and Epworth Scale were used in the preoperative period and at visits 1, 2 and 3. The Short Form-36 Health Survey (SF-36) (22) and the McGill Pain Questionnaire (MPQ) (23) were used at visit 2.
Common analgesics were used during the follow-up period for acute headache treatment, but no prophylactic drug therapy was prescribed.
Statistical analysis
In order to investigate the behaviour of headache frequency and time of outset of PCH during follow-up, patients were divided into three groups: G0, patients without SAH; G1, patients with SAH and without headache due to SAH during the preoperative evaluation; G2, patients with SAH and with headache due to SAH during the preoperative evaluation. The headache frequency recorded in the diaries was grouped into two periods, months 1–3 and 4–6, and statistical analysis was performed using the Kruskal–Wallis (KW) non-parametric test, for comparison between the three groups.
The relationship between headache frequency and degree of depression, anxiety and daytime somnolence, respectively, were calculated with the Pearson correlation test.
Two groups of headache types were considered for statistical analysis: ‘migrainous’, headaches that fulfilled the diagnostic criteria for migraine of to the IHS, and ‘non-migrainous’, patients who had another type of primary headache.
Homogeneity marginal tests were performed and the κ coefficient calculated to compare the characteristics of preoperative with postoperative headaches. Preoperative headaches were primary headaches that the patients had during their lifetime before surgery (headaches due to SAH were not included in this analysis).
Analysis of the MPQ was based on the Pain Rating Index (PRI) and on the Number of Words Chosen (NWC).
The linear multivariate regression model was used with a stepwise process of selection for the multivariate study of the pain domain of the SF-36 and the MPQ (24). The variables initially selected for the model were: age, gender, presence of neurological sequelae, number of surgeries, temporomandibular disorder, headache presence either fulfilling or not the criteria for PCH according to the IHS, type of previous headache (migrainous vs. non-migrainous), depression and anxiety scores at visit 2, SAH, and presence of primary headaches in the last 3 months before surgery. The significance level was P ≤ 0.05. The same model was used to evaluate the relationship between headache frequency and domains of SF-36, controlling for anxiety and depression.
The following computer programs were used for statistical analysis: Excel for Windows, version 2000; Minitab for Windows, version 13.0; SAS for Windows, version 8.0 (SAS Inc., Cary, NC, USA); S-Plus 2000 and SPSS for Windows, version 10 (SPSS Inc., Chicago, IL, USA).
Results
Eighty-six patients were hospitalized with Glasgow coma scale of 15 and operated for treatment of intracranial aneurysms in our institution during the study period. Seven patients died in the immediate postoperative period, and were excluded. Thus, 79 patients were included in the study group. The mean age of the study group was 45.3 years (range 23–71 years), 51 (64.6%) were women and 11 (13.9%) had no previous primary headaches. Of the 68 patients with primary headaches, 46 (60.5%) had migraine, 28 (36.8%) tension-type headache, one stabbing and one sexual activity-associated headache.
Of the 69 patients who had SAH, 68 reported headache associated with the bleeding. One patient did not recall having headache associated with the bleeding, but had been unconscious at the time. SAH-related headaches were reported as diffuse in 45.6% and bilateral in 92.6% of patients.
Eighty seven surgeries were performed: 78 (89.7%) by pterional approach, five (5.8%) by fronto-orbital-zygomatic and four (4.6%) by frontal. Eight patients were operated twice, all through the pterional approach.
Headaches were observed in 72 patients (91.1%) after surgery. Only 60% of patients had headache within 7 days after craniotomy, compared with 91.1% who had at least one headache during the follow-up period. We observed that 68.2% of patients who had headache in the craniotomy area developed headaches up to 7 days after surgery. This figure would have risen to 93.2% if the time period had been extended to 30 days.
Eight patients (10.1%) did not complete the follow-up: one after visit 0, two after visit 1 and five after visit 2. One patient had the headache diaries sent by mail. Two patients had already fulfilled PCH diagnostic criteria when lost to follow-up, and one patient had the headache onset beyond 7 days in the postoperative period. All seven patients who were headache free during the whole follow-up period completed the study. Of the 75 patients included, 30 (40%) had PCH, eight (10.7%) of the acute and 22 (29.3%) of the chronic type, according to the IHS diagnostic criteria.
Ten patients did not have SAH, having their aneurysms incidentally diagnosed through neuroimaging. Nine patients had had previous primary headaches. Six patients had headache outset during the first week in the postoperative period, but only four (40%) fulfilled PCH diagnostic criteria, all of the chronic type.
Table 2 shows the elapsed time between surgery and headache outset. Figure 1 shows the latency curves for time of headache onset for each study group. Log rank tests demonstrated a significant difference between groups G0, G1 and G2 (P = 0.02), but no significant difference between G0 and G1 (P = 0.96).

Latency curves for time of headache outset, according to the study groups (Kaplan–Meier method).
Time (in days) of headache onset after surgery of the study groups

All groups had a similar headache frequency in the preoperative period (KW test; P = 0.36). Figure 2 shows the headache frequency during follow-up. An initial increase in mean headache frequency was observed, followed by a decrease. There was a mean increase of 14 days in headache frequency in the first 3 months of the postoperative compared with the preoperative period. No significant difference between groups was found when both periods were compared (KW test; P = 0.29). The mean headache frequency was 6.9 days greater in the last 3 months of follow-up compared with that observed before surgery. No significant difference was observed between groups (KW test; P = 0.05). There was a decrease of 7.9 days in headache frequency between the first and second trimesters of the follow-up period, but, again, no significant difference was observed between groups (KW test; P = 0.33).
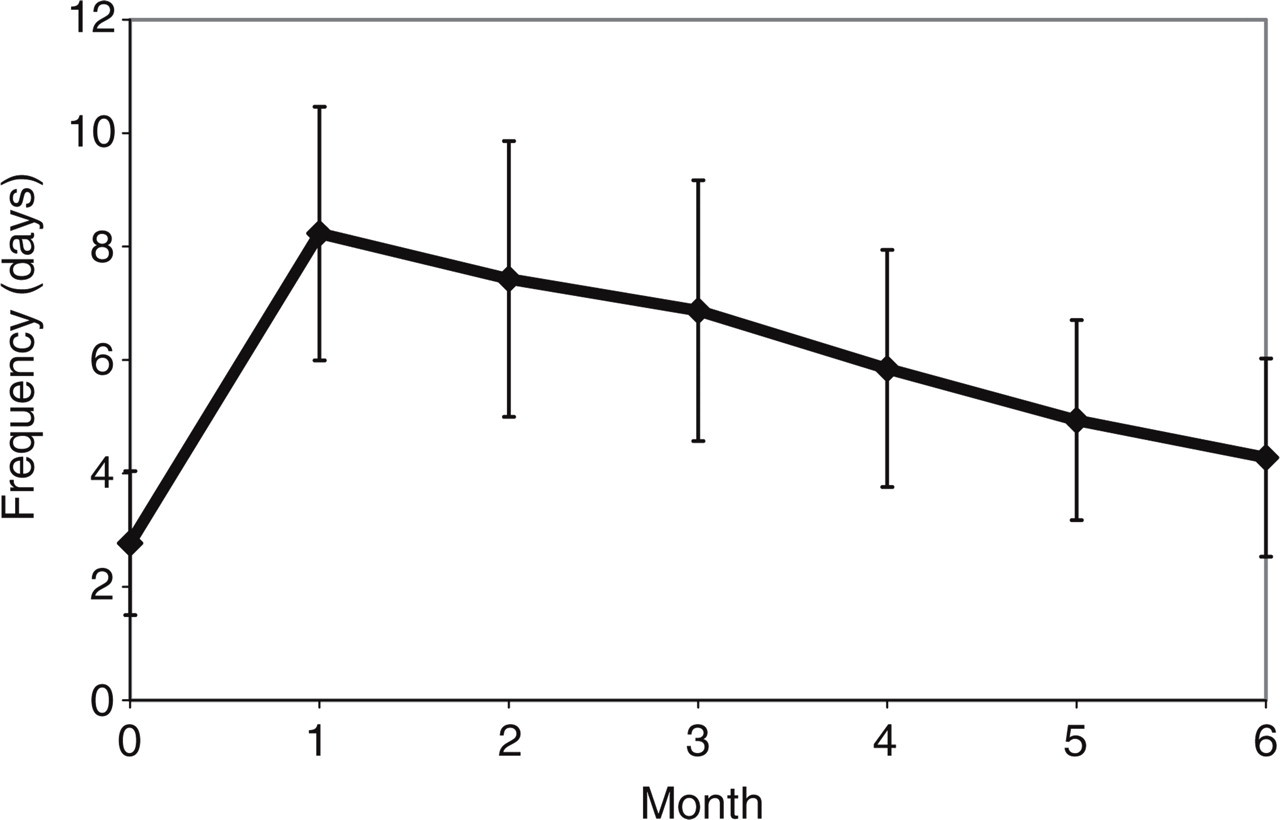
Headache frequency in the follow-up period.
There was a positive, significant correlation between anxiety and depression, and headache frequency during the whole study period (Table 3). The correlation between intensity of daily somnolence and headache frequency was positive and significant only in visit 1 (r = 0.24; P = 0.05).
Correlation between headache frequency and depression and anxiety scales during the study period

r = Pearson correlation coefficient.
A poor concordance was found between primary headache type in the preoperative period and that observed in each follow-up visit (Table 4), suggesting that the patients had different primary headaches types in the postoperative period compared with those experienced before surgery. Patients with more than one type of primary headache in the preoperative period and one patient lost to follow-up after visit 0 were excluded. A decrease was observed in the number of patients in the migrainous group during the follow-up period and an increase in headache-free patients.
Types of primary headache diagnosis in the preoperative and in each follow-up visit during the study period

No past history of primary headache.
We performed homogeneity marginal tests to compare the distribution of primary headache diagnosis. A statistically significant difference in headache diagnosis was observed between the preoperative period and visits 2 (P < 0.01) and 3 (P < 0.01). There was no statistically significant difference between headache diagnosis in the preoperative period and that observed at visit 1 (P = 0.10), between visits 1 and 2 (P = 0.06) or between visits 2 and 3 (P = 0.53).
Table 5 shows the distribution according to pain laterality during the study period. Patients that were operated twice were excluded. Kappa coefficient value estimates indicated poor concordance evidence between headache laterality in the preoperative period and visits 0, 1, 2 and 3, suggesting that headache laterality changed after surgery. Homogeneity marginal tests were performed to compare the distribution patterns of headache laterality at each visit. Data from visit 0 were excluded because, at that moment, all patients with headache had pain localized on the same side as surgery. A statistically significant difference was observed between pain laterality in the preoperative period and visits 1 (P < 0.01), 2 (P < 0.01) and 3 (P < 0.01), but not between visits 1 and 2 (P = 0.56) or visits 2 and 3 (P = 0.54). These results suggest an influence of surgery on pain laterality.
Pain laterality compared with surgical side during the study period

No past history of primary headaches.
Table 6 shows the distribution according to pain site during the study period. The results show poor concordance evidence between pain site in the preoperative period and the various follow-up visits, suggesting an influence of surgical procedure on pain site. Homogeneity marginal tests comparing pain site distribution patterns and surgical site showed a statistically significant difference between the preoperative period and visits 0 (P < 0.01), 1 (P < 0.01), 2 (P < 0.01) and 3 (P < 0.01), and no difference between the postoperative visits 0 and 1 (P = 0.83), 1 and 2 (P = 0.47) or 2 and 3 (P = 0.90).
Comparisons between pain site and surgical site

No past history of primary headache.
The multivariate analysis of the MPQ showed that pain intensity was higher in women (NWC), and that there was a positive correlation between pain intensity and the degree of anxiety symptoms (PRI).
The SF-36 scores were lower in all domains when compared with a sample of the national urban population (Table 7) (25). Multivariate analysis of the pain domain of SF-36 showed a statistically significant relation between higher scores of anxiety, in the HADS, and lower scores in the pain domain. There was a negative and significant association between headache frequency in the month before the application of SF-36 and the Social Functioning and Bodily Pain domains of SF-36.
Comparisons between mean SF-36 scores of the study group and those of a national urban population (25)

P < 0.05 (t-test for mean comparison).
Discussion
We studied headache frequency, types and characteristics in patients who had had craniotomies performed for treatment of intracranial aneurysms. Although SAH is a well-known cause of headache, by definition its duration is limited to 30 days after the acute bleeding (1). The bleeding effect, as expected, occurred early in the postoperative period, as shown by the earlier headache onset observed in patients with SAH and headache (G2), compared with those without headache, with (G1) and without (G0) SAH in the preoperative period (Table 2). Considering only the G1 and G0 groups, headache onset occurred in strict relation to the surgical procedure, a pattern already observed by others (8, 9). There was no difference in headache frequency between the study groups during the follow-up period. Headache frequencies before surgery were homogeneous between the study groups, a fact that suggests that there was no memory bias in the estimated frequencies.
An increase was observed in the mean headache frequency between the pre- and postoperative periods. The few studies that have investigated pain memory have focused on pain intensity and, concerning chronic pain, have shown a tendency towards pain overestimation (26). If this is also true for pain frequency, our patients would have reported a higher headache frequency before surgery and, consequently, a lower than expected increase in headache frequency should have been observed in the follow-up period. The increase in headache frequency also could have been underestimated in the follow-up period, because the headache diaries were delivered to the patients at visit 0, approximately 2 weeks after surgery, in order to decrease the effect of SAH on headache frequency. Assuming that, in the first days of the postoperative period, headache frequency behaviour was similar to that observed in the whole follow-up period, then it was probably higher in the immediate postoperative period.
A decrease in headache frequency was observed over time during follow-up in all study groups, as was a positive relation between headache frequency and anxiety and depressive symptoms intensity, a fact that has not been reported in other studies.
Our patients showed a decrease in headache prevalence over time during follow-up. This is in agreement with other studies in neurosurgical patients (2, 5–8, 10, 12, 13, 17–20). This pattern was observed both in migrainous and non-migrainous headache patients.
A change was observed in headache diagnosis and pain site in the postoperative compared with preoperative period. These changes persisted during the whole follow-up period and were probably due to a surgical effect. Migrainous headaches were observed in 54% of patients in the preoperative period, compared with 40% in visit 1, 27% in visit 2 and 30% in visit 3. On the other hand, a similar incidence of non-migrainous headache was observed in the preoperative period (30%) compared with the follow-up visits (Table 4). Several authors who have studied headache characteristics after craniotomies have observed a pattern similar to tension-type headache, although data were obtained retrospectively, long time after the surgical procedure (6, 8, 9, 13, 17).
SAH headaches had a predominantly bilateral pattern in our patients, and none was predominantly localized in the surgical site. All patients could easily distinguish between primary headaches experienced before surgery and those caused by SAH. The possible influence of SAH over preoperative primary headache patterns was to decrease the observed differences, rendering postoperative headaches more diffuse.
An incidence of PCH of 40% was observed according to IHS classification criteria. This was also observed in the patients with no SAH.
According to the concept that a secondary headache should develop in strict temporal relation to the underlying disorder, a cutting point of 7 days after surgery for headache onset in PCH is reasonable. However, this is somewhat arbitrary and based on little previous empirical evidence in the literature. Our study has shown that increasing the time period for headache onset from 7 to 30 days would lead to a significant rise in the number of patients with PCH diagnosis.
PRI (27, 28) and NWC of MPQ are related to the intensity of pain (27). PRI has been related to headache intensity recorded in headache diary (29) and is more sensitive than NWC to detect changes in pain intensity (27). We found that pain was more intense in women (NWC) and in patients with more anxiety symptoms (PRI), regardless of sex. The gender difference between NWC and PRI results occurred because women matched more words with a smaller score value than men. This is in agreement with other authors, who have also reported that women have higher pain sensitivity than men (30, 31).
Anxiety may lead to a greater perception of pain intensity (32, 33), as seen in our patients. A recent study, using functional magnetic resonance imaging, has shown that the entorhinal cortex of the hippocampal formation responds differently to identical noxious stimuli, depending on pain-relevant anxiety (34).
We observed a significant pain effect on patients' lives (pain domain of SF-36) compared with the general population. This has also been observed by Betchen et al. (35) in patients submitted to acoustic neuroma surgery. Martin et al. (36) observed no such relation, in a retrospective study performed 18 months after surgery.
Anxiety can diminish the eight domain scores of the SF-36, including pain (37). Our study has shown that anxiety was related with higher pain intensity (PRI) and lower scores in pain domain of the SF-36
Our study has shown that headache frequency has a negative effect on patients' quality of life and daily social activities. We used the headache frequency of the month prior to the application of the SF-36 and controlled for associated depressive and anxiety symptoms that could interfere with quality of life (37, 38).
We conclude that there is a causal relation between craniotomy and headaches that occur after surgery. Headache onset in close temporal relation with the craniotomy, changes of headache pattern and increase in headache frequency after craniotomy are evidence that support this assertion. PCH has significant negative effects on patients' quality of life.
Acknowledgement
The authors acknowledge the support of the Mathematics and Statistic Institute of the University of São Paulo for the statistical analysis.