
Abstract
Background
The prevalence of patent foramen ovale (PFO) is higher among adult migraine patients. The purpose of this study was to determine the frequency of PFO in children and adolescent migraine patients.
Methods and results
A total of 32 patients with migraine (divided into two subgroups, the migraine with aura subgroup and the migraine without aura subgroup) and 31 normal control subjects were enrolled in this study. All of the participants underwent transthoracic echocardiography with an agitated saline test. We compared the prevalence of PFO and the severity of right-to-left shunt (RLS) in each group. No statistical difference in age and sex ratio was observed in either group. The prevalence of PFO was higher in the migraine group than in the control group, but without statistical significance (46.9% vs. 25.8%, p = 0.084). The prevalence of PFO was significantly higher in the migraine with aura subgroup than in the migraine without aura subgroup (p = 0.031) and the normal control group (p = 0.0074). Migraine with aura was the only significant factor showing an association with PFO (<0.01). RLS size did not have an influence on migraine.
Conclusions
Considering the significantly high prevalence of PFO in pediatric migraine with aura patients, migraine with aura is a clear predictor of PFO among children and adolescents.
Introduction
Migraine, the most common acute and recurrent type of headache in children (1,2), can become a chronic, disabling disorder, having a substantial effect on the lives of patients and their families. These headaches commonly occur during childhood and adolescence (3–5), and the incidence of migraine in children has shown a substantial increase (6).
Patent foramen ovale (PFO) is the result of incomplete fusion of the septum primum and septum secundum of the atrium that normally occurs after birth. In patients with this condition, a right-to-left shunt (RLS) occurs when the right atrial pressure exceeds the left atrial pressure. PFO can be detected in 20–30% of the general population (7,8) and is a well-known risk factor for ischemic stroke in young patients (9,10). In adults, many studies have shown that the prevalence of PFO is higher among patients with migraine. In addition, PFO is more prevalent among individuals suffering from migraine with aura than migraine patients without aura (11–14). Few studies of the association between PFO and migraine in children have been reported (15).
The current study was designed to examine the frequency of PFO in patients with pediatric migraine with or without aura and to determine whether migraine is a predictor of PFO in children and adolescents.
Methods
Our study included a total of 32 patients diagnosed with migraine at the pediatric neurology outpatient clinic of Gachon University Gil hospital from September 2008 to December 2011. A diagnosis of migraine was based on the criteria of the International Headache Society (The International Classification of Headache Disorders: 2nd edition (ICHD-II)) (16). The control group consisted of 31 non-migraineur individuals of similar ages and gender distribution. Information about the patients’ migraine history was obtained by a single pediatric neurologist during a face-to-face interview. Visual, sensory, or motor aura-related symptoms were also evaluated. The duration of the pain problem was presented as mean ± standard deviation (SD) in hours, which was calculated from the time when the current pain problem or aura began to the time when the pain disappeared or the patient went to sleep. The maximal and average pain intensity in the last four weeks was measured using a numeric rating scale (NRS; with 0 = no pain to 10 = maximal pain) and presented as mean ± SD. In children aged 11 years and older, duration of pain and pain intensity in the past four weeks was measured by self-report, while the information was obtained by parent proxy report for children younger than 11 years of age (17). The institutional review board of Gachon University Gil Hospital approved the acquisition, analysis, reporting of patient data, saline injection, and contrast echocardiography (number: GIRBA 2513).
The presence of PFO was determined by two-dimensional (2D) transthoracic echocardiography (TTE) using standardized procedures with infused agitated saline. Two 10-cc syringes were used; one contained 9 cc of normal saline and the other contained 1 cc of air. The contents of both syringes were rapidly mixed through a three-way stopcock until a homogeneous solution was obtained. The solution was then rapidly injected by hand into the antecubital vein through a venous cannula while the patient was at rest. PFO was diagnosed if microbubbles crossed the atrial septum after administration of the agitated saline injection. A 2D TTE image was obtained from the apical four-chamber or subcostal views with both normal breathing and valsalva maneuver by a single pediatric cardiologist.
The patient was considered PFO positive if three or more microbubbles appeared in the left atrium either during normal breathing or valsalva maneuver within three cardiac cycles after complete opacification of the right atrium. The RLS was graded as small (three to nine microbubbles), moderate (10 to 30 microbubbles), or large (>30 microbubbles).
Statistical analysis
Clinical data and cardiac imaging findings of the migraine and control groups were compared. The migraine group was divided into two subgroups (with or without aura). The prevalence of PFO between three groups (migraine with aura, migraine without aura, and control) was compared, and the relationship between PFO grading and aura was analyzed. Comparisons between groups were made using a chi-square test and Fisher’s exact test using MedCalc® version 11.2.1.0 (MedCalc Software, Mariakerke, Belgium). A p value <0.05 was considered statistically significant. Logistic regression analysis was performed for identification of predictors showing an independent association with PFO. The odds ratio (OR) and 95% confidence interval (CI) also were calculated.
Results
Demographic data of the total groups.
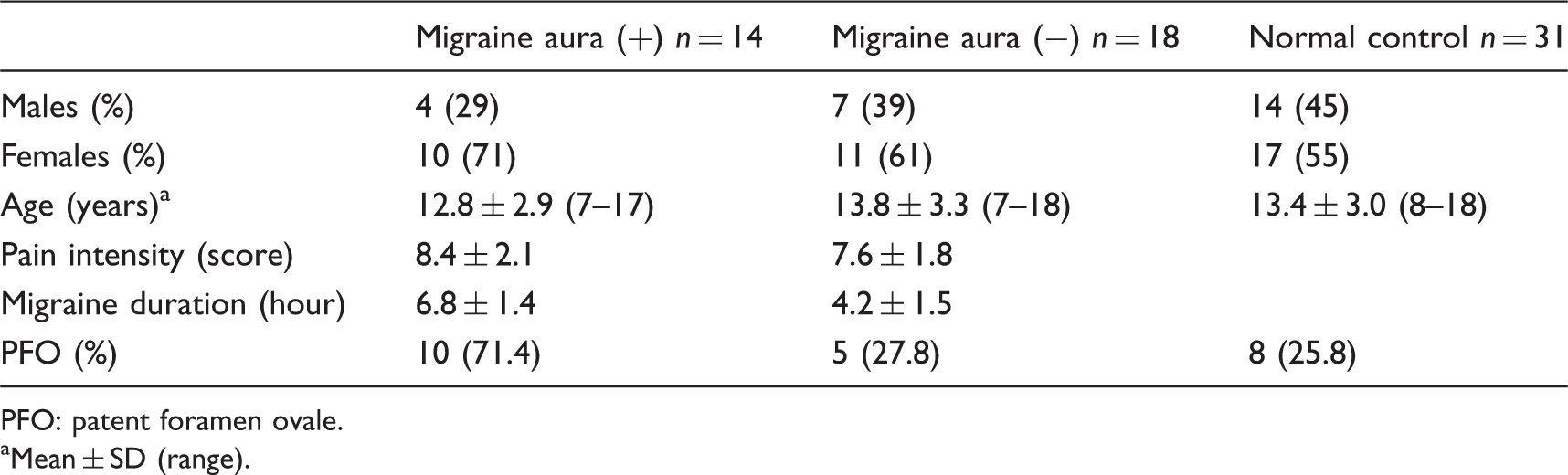
PFO: patent foramen ovale. aMean ± SD (range).
A total of 38 girls and 25 boys were included in this study. Patient and control groups included 21 (65.6%) and 17 (54.8%) girls, respectively. No significant gender-associated difference in the prevalence of migraines was observed. Age of the study participants ranged from 7–18 years for patients and 8–18 years for the control group. No significant differences were observed between the age or sex of participants in the two groups. Fourteen patients had experienced migraine with an aura, while migraine was not accompanied by an aura in the remaining 18 patients.
Among subjects in the migraine group, the mean maximal pain intensity was 8.4 ± 2.1 in the migraine with aura subgroup and 7.6 ± 1.8 in the migraine without aura subgroup, respectively (NRS 0–10). The duration of pain was 6.8 ± 1.4 hours in the migraine with aura subgroup and 4.2 ± 1.5 hours in the migraine without aura subgroup, respectively.
PFO prevalence in each subgroup.

PFO: patent foramen ovale. aMigraine versus the normal control group. bMigraine with aura versus the normal control group. cMigraine without aura versus the normal control group.
Comparison between PFO-positive and -negative groups.

PFO: patent foramen ovale.
Association with PFO according to logistic regression analysis.

PFO: patent foramen ovale; OR: odds ratio; CI: confidence interval.
Comparison between shunt size, morphology and subgroups among PFO-positive individuals.a

PFO: patent foramen ovale; ASA: atrial septal aneurysm. aNo significant difference between the three groups.
Discussion
Available data suggest that PFO is more common in patients with migraine with aura, and that migraine with aura is more common in adults with PFO (14,18). History of migraine headache commonly starts during childhood and adolescence. In 1962, Bille reported on the epidemiology of pediatric migraine in 8993 children (3). Migraine was reported in 3.9% of children aged 7–15 years; this percentage showed an increase from 1.7% among 7-year-old children to 5.3% among 15-year-old patients (5). A recent epidemiological study of 2669 children in Istanbul, Turkey, reported that 3.4% of children aged 5–13 suffered from migraine and that 8.7% of children had experienced probable migraine (4). According to findings of our study, the relationship between PFO prevalence and migraine in children and adolescents (ages 7 to 18 years) was similar to those reported in adults and other children described above. Prevalence of PFO in patients experiencing migraine with aura was significantly higher, compared to that of patients experiencing migraine without aura and normal control subjects. Although the prevalence of PFO was higher in the migraine group (with or without aura) than in the control group, and showed borderline significance, the result was not statistically significant (p = 0.084). This result may be due to low power caused by a small sample size. Performance of a further study using a large number of cases will be needed.
The mechanism underlying the possible relationship between PFO and migraine remains unclear. Co-inheritance has been proposed as an explanation for increased prevalence of RLS in patients with migraine. Migraine is associated not only with PFO but also other cardiac and pulmonary RLS diseases (19,20). Co-inheritance alone is not likely, given the improvement of migraine observed after shunt closure. Thus, an additional interaction between the RLS and increased migraine susceptibility has been postulated (21,22). RLS has been proposed as an alternative trigger of migraine attacks. According to one hypothesis PFO may allow venous-circulating, migraine-triggering, vasoactive chemicals to bypass the pulmonary filter and enter the cerebral circulation, thereby inducing a migraine attack, particularly venous emboli and serotonin (20).
PFO is a risk factor for paradoxical embolism and cryptogenic stroke (23,24). Small paradoxical embolism has also been proposed as a migraine-promoting factor. Paradoxical emboli appear to have a propensity for the posterior circulation, an area in which hypoperfusion occurs with a migraine aura (25). Experimental data in mice have indicated that cerebral microembolization can evoke cortical spreading depression, a putative biological substrate for migraine with aura and paradoxical emboli, which can occur as a result of RLSs within the heart and can create a transient hypoxic-ischemic focus to induce cortical spreading depression followed by migraine attack (26). Percutaneous closure of PFO has recently been recognized as an effective treatment for prevention of paradoxical embolism (27,28).
Many studies have reported an increased risk of stroke in migraine patients as well as in those taking oral contraceptives (29–32). In addition, migraine with aura has been identified as an independent risk factor for stroke (31,32). Migraine with aura is an important risk factor for stroke, along with PFO. Several retrospective and prospective studies to prove the efficacy and safety of PFO closing intervention for treatment of migraine are in progress (33–35), although the migraine intervention with STARflex® technology I (MIST study) failed to demonstrate that any benefit from PFO closure was effective treatment (36).
In conclusion, we demonstrated that prevalence of PFO among children and adolescents suffering from migraine with aura is significantly higher compared to that of patients experiencing migraine without aura and normal individuals. Therefore, migraine with aura among children and adolescents was identified as an important predictor of PFO.
Study limitations
This study has several limitations. First, the sample size was too small. Due to difficulty in enrolling child volunteers, we did not calculate the sample size prior to beginning this study. In this study, small sample size limits the significance of several findings, such as the result of the comparison of PFO prevalence between the migraine group and control group (46.9% vs. 25.8%, p = 0.084, respectively). Although this difference may be clinically relevant, it was not significant in this study. This may be due to the small sample size, related to the possibility of a type II error. Second, we did not perform an evaluation using magnetic resonance imaging (MRI) in order to disclose previous silent ischemic brain lesions or cerebrovascular abnormalities. Third, we did not include data on drug treatment, such as several migraine-preventive medications, antiplatelet, and anti-inflammatory agents, and individual response. Therefore, analysis of the therapeutic effect of percutaneous closure for migraineurs not responsive to medication could not be performed. Fourth, the cardiologist was not blind to the patients’ headache status, which can influence important readings of results.
Clinical implications
The prevalence of PFO was significantly higher in the migraine with aura subgroup than in the migraine without aura subgroup and the normal control group. Migraine with aura was the only significant factor showing an association with PFO. Considering the significantly high prevalence of PFO in pediatric migraine with aura patients, migraine with aura is a clear predictor of PFO among children and adolescents.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.