
Abstract
Migraine with aura (MA) is associated with the persistence of patent foramen ovale (PFO) in about 50% of cases, and migraineurs tend to have larger shunts than controls, suggesting that right-to-left shunt (RILES) determined by PFO could play a role in triggering migraine attacks. Moreover, some preliminary reports have suggested that PFO closure may give relief to both migraine and aura attacks. The aim of this study was to clarify if shunt-associated migraine (SAM) has clinical features that allow a distinction from shunt-unrelated migraine (SUM), in a prospective, multicentre, observational study (SAM study). We enrolled consecutive MA patients, who underwent a structured, standardized questionnaire for family and personal history and for detailed migraine features. All were systematically screened for RILES with transcranial Doppler, and for coagulation disorders. Overall, 460 patients were included; the SUM and SAM classes comprised 58% and 42% of patients, respectively. SAM patients were significantly younger (34.1 ± 10 vs. 37.1 ± 11 years), had a more frequent family history of migraine (76% vs. 66%) and a higher frequency of sensory symptoms of aura (51% vs. 41%); by contrast, there was a lesser association of SAM with other cardiac abnormalities and with coagulation disorders. The SAM study suggests that the effect of RILES on migraine features is not relevant. The higher family history of migraine in SAM suggests a possible genetic linkage between migraine and RILES.
Introduction
Migraine and patent foramen ovale (PFO) are associated to an extent that goes beyond what would be predicted by the chance co-occurrence of two common conditions. In case–control studies, migraine with aura (MA) has been found to be associated with PFO in nearly 50% of cases, twice the figure usually reported in non-migraineurs (1–3), and in patients with PFO migraine has been found twice as frequently as in patients without PFO (4–6). Moreover, MA patients tend to have larger shunts than controls, and closure of PFO may bring relief to migraine, suggesting that the right-to-left shunt (RILES) determined by PFO could play a role in triggering migraine attacks through the mechanism of paradoxical brain embolism of platelets or chemical substances (7–11). The question then arises of whether in migraineurs with PFO shunt-associated migraine (SAM) has clinical features that allow a distinction from shunt-unrelated migraine (SUM).
We undertook a multicentre study to elucidate this issue in a prospective series of migraine patients. The aim was to assess whether clinical features help in differentiating SAM from migraine without shunt in order to identify a specific syndrome that could be tested in ad hoc trials of PFO closure.
Materials and methods
From January 2005 to December 2006 the prospective, multicentre, observational SAM study enrolled all consecutive MA patients attending the out-patient clinics of the participating centres. In four out of 12 recruiting centres the patients were drawn from headache clinics, and in the remaining eight from general neurology clinics. Criteria for admission were: diagnosis of MA according to the International Headache Society 2004 criteria (12), age < 55 years, no prophylactic treatment at the time of inclusion and willingness to sign the informed consent to undergo the prespecified diagnostic work-up.
This included a detailed history taking, full neurological examination, brain magnetic resonance imaging (MRI) with prespecified sequences which were the same in all participating centres, screening for RILES with saline contrast-enhanced transcranial Doppler (sce-TCD), complete screening for coagulation abnormalities (plasma levels of protein C, protein S and homocysteine, activated protein C resistance, factor II and V Leiden, presence of antiphospholipid antibodies, methylenetetrahydrofolate reductase gene polymorphisms) and screening for mitral valve prolapse, atrial septal aneurysm and Eustachian valve with transthoracic echocardiography (TTE). We defined a thrombophilic disorder as present when at least one of the above-mentioned tests was abnormal. To avoid the enrolment of RILES due to pulmonary fistulas, only patients with TTE-confirmed PFO were included. The history taking was structured with a computer-based standard questionnaire so as to include personal or family history of cerebrovascular disease and cerebrovascular risk factors (hypertension, diabetes, known heart disease, dyslipidaemia, cigarette smoking, use of oral contraceptives). The following migraine features were systematically investigated: family history of headache, age of migraine onset, duration and characteristics of aura, frequency and severity of migraine attacks in the last 12 months, trigger factors and type of drugs used to abort attacks. To characterize aura, five domains of symptoms were systematically investigated, which included visual scintillating scotoma, unilateral somatic sensory troubles, aphasic symptoms, lateralized motor troubles and vertebrobasilar symptoms (dizziness, diplopia or faintness) occurring before headache. A score for aura complexity was derived as the sum of domains involved during the aura, which ranged from 1 to 5. Drug efficacy was defined as the disappearance of headache within 2 h of ingestion. A single experienced rater in each centre, blinded to the sce-TCD results, collected all clinical information. The assessment of RILES with sce-TCD was performed as detailed elsewhere (13). The highest number of microbubbles recorded in the right middle cerebral artery after i.v. injection of agitated saline during normal breathing and before a Valsalva manoeuvre was used to exclude (if bubble count = 0 in both conditions) or to quantify (if bubble count > 0) RILES. The amount of RILES with Valsalva strain was semiquantitatively graded in four categories based on the number of bubbles: 0, no shunt; I, < 10 bubbles; II, > 10 bubbles single spikes; III, > 10 bubbles, shower or curtain pattern. A set of test TCD tracings had to be preliminarily assessed by each participating centre before starting enrolment. The interobserver agreement with the score used as reference was high for each centre, with k-values ranging from 0.7 to 0.9.
For dichotomous comparisons grades 0 and I were collated (NO SHUNT) and contrasted with RILES II and III (SHUNT), as grade I was considered haemodynamically non-significant and therefore functionally irrelevant. Subsequent analysis contrasting grade 0 with grade III was undertaken to explore the possibility that further differences might emerge in patients with the largest shunt.
The study was approved by the Ethics Committee of the S. Orsola Hospital FBF.
Statistical analyses (SPSS version 13.0; SPSS Inc., Chicago, IL, USA) were done for continuous variables with t-test or Mann–Whitney tests according to whether or not data were distributed normally as preliminary assessed with Kolmogorov–Smirnov test. Frequencies were analysed with χ2 test. Statistical significance was set at P < 0.05.
Clinical and TCD data are described in the present paper. MRI findings will be reported elsewhere
Results
Overall 460 patients were included (age 35 ± 11 years, M/F 107/353) by the 13 participating centres. One hundred and seventy-three patients (37.6%) had no detectable RILES, 92 (20%) had type I, 85 (18.5%) type II and 110 (23.9%) type III RILES. After pooling together type 0 with type I and type II with type III shunts, the resulting NO SHUNT and SHUNT classes comprised 58% and 42% of the entire cohort, respectively.
The results of univariate analyses comparing SHUNT vs. NO SHUNT patients are shown in Tables 1 and 2 and in Figs 1–4. SHUNT patients were significantly younger (34 ± 10 vs. 37 ± 11 years, P = 0.003), had a significantly higher frequency of migraine in the family history (76% vs. 66%, P = 0.045), had a significantly higher frequency of sensory symptoms characterizing the aura (51% vs. 41%, P = 0.031), a significantly decreased association of cardiac abnormalities other than PFO (4% vs. 10%, P = 0.020) and were significantly less likely to exhibit coagulation abnormalities (23% vs. 37%, P = 0.011). Moreover, they exhibited a non-significant trend for a lower body mass index (BMI) (22 vs. 23, P = 0.057) and for a lesser number of migraine attacks (20 vs. 24, P = 0.07) in the 12 months preceding their inclusion.
General characteristics of patients with SHUNT (types II and III pooled together) and NO SHUNT (types 0 and I pooled together)

Characteristics of migraine attacks in patients with SHUNT (type III) and NO SHUNT (type 0)

In the previous 12 months.
The score of aura complexity is the sum of the involved domains (visual, sensory, motor, aphasic, vertebrobasilar).
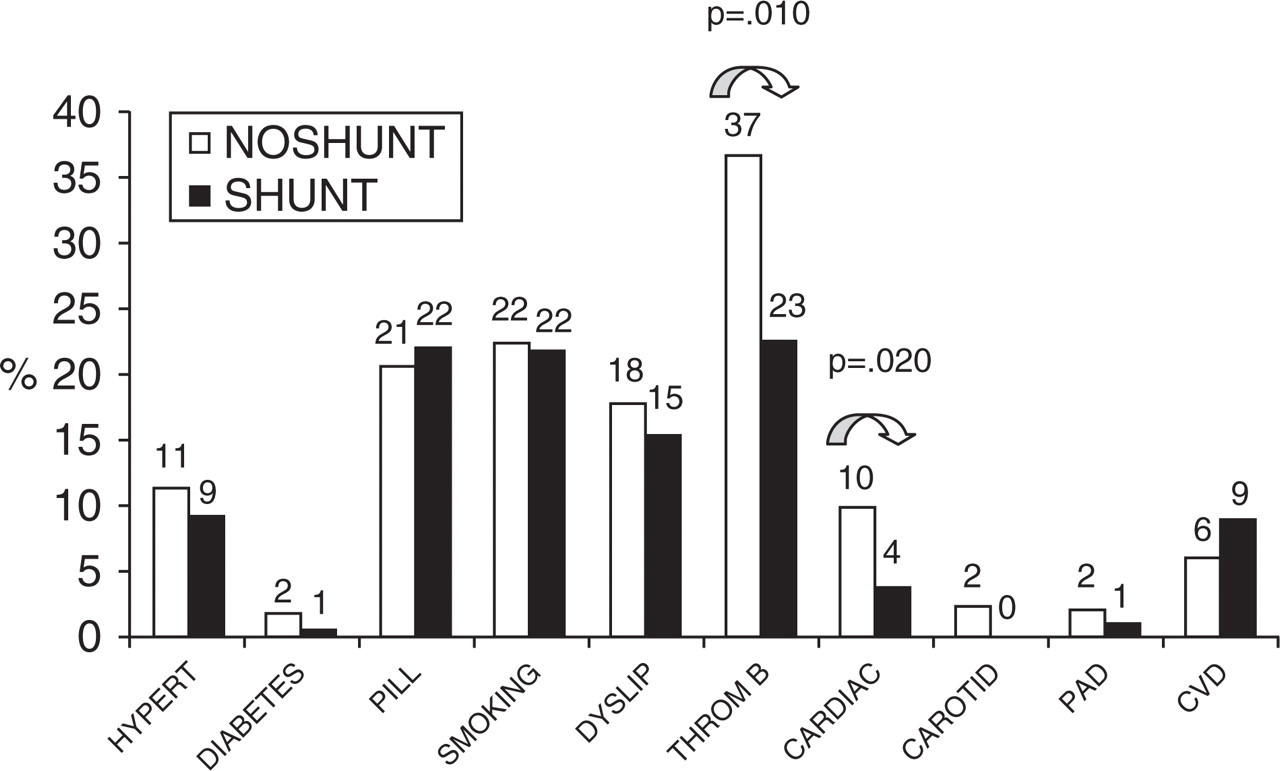
Cerebrovascular risk factors. Vertical axis: percentage of patients. Hypert, Hypertension; Diabetes, diabetes mellitus; Pill, current use of oral contraceptives; Smoking, current cigarette smoking; Dyslip, dyslipidaemia (total cholesterol > 200 mg/dl or current use of cholesterol-lowering agents); Thromb, thrombophilic disorder (see Introduction for details); Cardiac, known heart disease; Carotid, carotid stenosis; PAD, peripheral artery disease; CVD, previous stroke or transient ischaemic attack; SHUNT, type II and III patients pooled together; NO SHUNT, type 0 and type I patients pooled together.
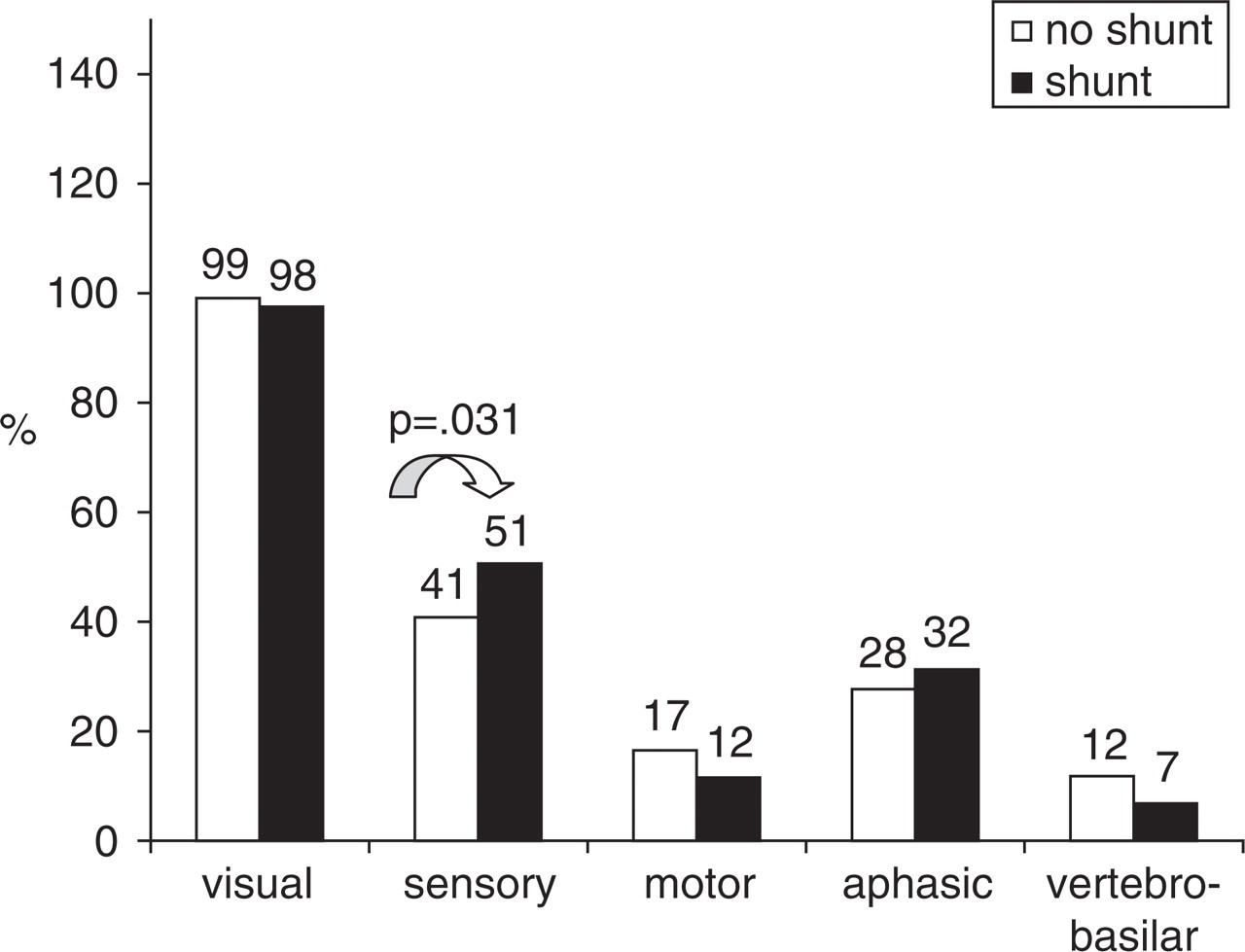
Domains of symptoms occurring during aura. Vertical axis: percentage of patients. SHUNT, Type II and III patients pooled together; NO SHUNT, type 0 and type I patients pooled together.

Trigger factors for migraine attacks. Vertical axis: percentage of patients. SHUNT, Type II and III patients pooled together; NO SHUNT, type 0 and type I patients pooled together.

Responsiveness to abortive agents. Vertical axis: percentage of patients reporting the drug efficacious. NSAIDs, Non-steroidal anti-inflammatory drugs; SHUNT, type II and III patients pooled together; NO SHUNT, type 0 and type I patients pooled together.
No difference in the sensitivity to abortive agents was apparent.
In a further analysis, only patients with type 0 (n = 173, M/F 42/131) and type III shunts (n = 110, M/F 19/91) were included. Again type III patients turned out to be younger (34 ± 10 vs. 38 ± 12 years, P = 0.002), had a higher frequency of migraine in the family history (76% vs. 64%, P = 0.035), a higher frequency of sensory symptoms during auras (50% vs. 37%, P = 0.035), fewer cardiac abnormalities (4% vs. 11%, P = 0.041) and fewer coagulation abnormalities (19% vs. 41%, P = 0.003). The difference in BMI was now significant (22 vs. 23, P = 0.025) as well as the difference in the total number of attacks (median n = 18 vs. 27, P = 0.014). Moreover, type III patients had significantly fewer migraine without aura (MoA) attacks (median n = 2 vs. 12, P = 0.011), which was mirrored by an almost significant higher percentage of attacks preceded by aura (90% vs. 60%, P = 0.076), a lower frequency of menstruation as a trigger for migraine attacks (30% vs. 65%, P = 0.034) and a lower frequency of vertebrobasilar symptoms during auras (3% vs. 12%, P = 0.007).
Discussion
Migraine is a complex disorder in which many psychological, environmental, biochemical and neurophysiological factors may play a role in triggering attacks (14, 15). Thus, the reported high frequency of RILES in MA has raised the hypothesis that an accumulating overload of putative triggers shunted from the venous to the arterial side of circulation at any cardiac cycle may at times exceed the clearance capacity of the lung and initiate the attack (7, 16, 17). This does not obviously imply that RILES is the cause of migraine, as only 50% of MA patients exhibit atrial septal defects and not all subjects with PFO have migraine. However, this mechanism might play a significant, perhaps the most significant role in subjects with a constitutional susceptibility to migraine. In support of this contention is the finding that in consecutive series of PFO patients, migraine has consistently been found with a frequency exceeding the expected prevalence (18–20) and SAM patients have on average a larger shunt than PFO subjects without migraine (8, 9).
The SAM study is the first prospective study to enroll MA patients with the aim of searching for the specific clinical features of SAM by systematically exploring in detail any item of the MA syndrome.
SHUNT patients were significantly younger than NO SHUNT patients, which means that they looked for medical advice at a younger age. The reason for this is not entirely clear, although we would tentatively attribute it to the relatively atypical characteristics of auras with more sensory symptoms possibly raising doubts for alternative diagnoses and thus leading to earlier medical consultation. Apart from a higher frequency of family history positive for migraine, SHUNT patients did not exhibit specific clinical features that could identify a migraine syndrome linked to RILES. Some trends which were apparent in the dichotomized comparison became significant when patients with no shunt whatsoever were compared with those with the largest shunts. Paradoxically, shunt patients had significantly fewer attacks in the previous 12 months (see Table 2), although the attacks were more often with aura. It appears therefore as if the presence of RILES reduced the susceptibility to develop a migraine attack following exposure to other triggers, but enhanced the likelihood of initiating the attack with an aura. Consistent with this view is the particularly relevant improvement in the frequency of auras following PFO closure (21). Patients with RILES reported fewer cardiac diseases than those with no atrial shunts, a finding which might result from recall bias. On the other hand, the reduced frequency of coagulation disorders might be genetically determined in association with the persistence of foramen ovale or, alternatively, might reflect the enhanced susceptibility of PFO patients to develop headache even for minor hypercoagulable states because of the bypass to the brain of coagulation by-products (22).
Finally, the reduced frequency of vertebrobasilar symptoms in type III patients, which was not apparent in the dichotomized comparisons, might have occurred by chance.
Schwerzman et al. recently reported on their single-centre experience with 93 MA patients. They found a 47% prevalence of PFO and did not find any difference in the clinical picture of patients with PFO compared with those without RILES (8). However, the sample size was small and it is unclear which clinical characteristics were explored and if these were looked for systematically in a standardized format.
Likewise, Dalla Volta et al. (23) were unable to find any phenotypic difference between patients with and without PFO. Again, the retrospective and non-standardized assessment of migraine features limits the validity of their findings.
In a recent paper, Domitrz et al. (24), in accordance with our findings, found that MA patients with RILES had a family history positive for MA in 82% of cases, whereas in patients without RILES the figure was 64%. However, this difference was not statistically significant, probably because of the small sample size.
In contrast with previous reports (8, 23, 24), the SAM study has some merits: it is multicentre, the recruitment was prospective and data acquisition was standardized. Its main weakness is the retrospective assessment of many clinical parameters (such as the number, duration and severity of attacks as well as the duration of auras) and the fact that these were reported by the patients, thus introducing recall bias. Despite these limitations, however, the present study provides the best available dataset to derive the phenotypic expression of the SAM syndrome.
From our findings it appears that the overall vascular profile does not differentiate SAM from SUM, except perhaps a reduced frequency of coagulation disorders in SAM.
Migraine itself does not appear to discriminate between SAM and SUM in terms of overall severity, sensitivity to food triggers or responsiveness to abortive agents. There was a significantly higher frequency of sensory symptoms during auras in SAM, but this finding was by no means peculiar to SAM patients, as it also occurred in two-fifths of patients without RILES.
However, SAM patients were significantly more likely to have at least one first-degree relative affected by migraine. The finding of a more pronounced family history of headache in SAM is in accordance with a recent report by Wilmshurst et al. (25), who studied 71 relatives of 20 probands with a significantly sized atrial shunt. When the proband had MA and an atrial shunt, 15 of the 21 (71.4%) first-degree relatives with a significant RILES also had MA, compared with three of 14 (21.4%) without a significant shunt (P < 0.02), suggesting that the migraine trait may be inherited in association with atrial shunts, at least in some kinships.
In summary, the results of the SAM study confirm the association of MA with RILES. Overall, > 60% of MA turned out to be RILES carriers and > 40% had a significant RILES. This association would favour the commonly held hypothesis that PFO may promote migraine by shunting to the brain active substances, the most likely of which is serotonin, in amounts sufficient to trigger the attack. This interpretation, however, leads to some predictions: given the longstanding nature of the shunt, migraine would be expected to appear early in life and, because of the continuous stimulating effect on the brain, it would be expected to be more often with aura and overall with a high frequency of attacks. Furthermore, the attacks would have to be facilitated by Valsalva manoeuvres, which increase RILES and hence exposure of the migraine-generating centres to the putative triggers. Finally, the possibility that platelet aggregates are delivered to the brain capillary bed would imply that local ischaemia could occur, which in turn could initiate the neurophysiological cascade of events that ultimately causes the clinical occurrence of aura and then headache. Given the random location of these phenomena, it would be predicted that SAM would entail attacks with more variable duration and complexity of auras.
Our findings met only few of the above predictions. MA was associated with RILES in a proportion of cases even higher than is reported in the literature, SAM patients had a higher prevalence of sensory auras than SUM patients and, at least those with the largest shunts, a relatively higher ratio of MA/MoA attacks. However, they did not exhibit any trend for an earlier start of migraine, for a higher complexity of auras or for a peculiar susceptibility of attacks to activities involving Valsalva strain and, in sharp contrast to the prediction, they had a significantly reduced frequency of attacks than migraineurs without shunt.
Therefore, the direct effect of RILES on migraine appears at best marginal and surely not sufficiently characterized to allow the separation of a distinct clinical entity. Indeed, the striking mismatch in SAM between the expected and the true clinical picture makes in our opinion the interpretation of migraine as promoted by shunted chemicals at best questionable, if not untenable.
On the other hand, what seems to be confirmed from our findings is the genetic linkage between MA and RILES. SAM patients had a higher prevalence of first-degree relatives affected by migraine and a lesser occurrence of genetically determined coagulation abnormalities. These findings, besides suggesting that some hitherto unknown genetic abnormality may disrupt endothelial signalling and thus underlie both the missed PFO closure and the susceptibility to develop migraine, open interesting perspectives for the genetic determination of SAM, which, however, should be viewed as another example of migraine comorbidity (26) rather than a separate clinical entity.
Footnotes
Acknowledgements
The study was partially funded by a grant from AFaR (Associazione Fatebenefratelli per la Ricerca) and was presented in a shortened version as a poster at the 59th Annual Meeting of the American Academy of Neurology Boston MA, 28 April to 5 May 2007.