
Abstract
We present a new case of cardiac myxoma triggering migraine auras. A 52-year-old woman was suffering from migraine attacks with aura. Magnetic resonance imaging (MRI) showed no abnormalities. Subsequently, she had a minor stroke with multiple ischaemic lesions bilaterally on repeat MRI. An echocardiogram showed a myxoma of the left atrial wall. After removal of the myxoma she was free of symptoms. In the past, seven cardiac myxoma associated migraine patients have been reported. Other cardiac abnormalities, patent foramen ovale in particular, are known to be associated with migraine with aura. We attempted to compare the mechanisms by which cardiac myxoma and other cardiac abnormalities could trigger cortical spreading depression leading to migraine with aura.
Keywords
Introduction
Numerous papers have shown an association between migraine, in particular migraine with aura (MA), and cardiac abnormalities (1). Patent foramen ovale (PFO) has been a popular, but controversial, subject of migraine research in recent years. Several studies have shown an association between PFO and MA and various pathophysiological mechanisms have been suggested (2).
Atrial myxomas are the most common primary heart tumours. Primary cardiac tumours have an incidence of 1 in 5000 at autopsy and myxomas account for 40–50% of primary cardiac tumours. They are most commonly found in the left atrium. Patients can present with a variety of symptoms, including malaise, weight loss, and cardiac and embolic symptoms. Approximately 30% of patients present with neurological signs, the most frequent being stroke, particularly in young patients. Left-sided tumours are more likely to embolise to the brain, but even right-sided myxomas may do so through an atrial septal defect or PFO (3–5). Migraine with aura is a relatively uncommon presentation of cardiac myxoma, but several case reports have been published (6–12). In this paper, we present a new case of cardiac myxoma triggering migraine auras, review the literature on the association, and hypothesise on the mechanisms of MA triggered by cardiac myxoma as well as other cardiac abnormalities and right-to-left shunt conditions.
Case history
A 52-year-old woman was seen for evaluation of neurological symptoms followed by headache. A few months before the final diagnosis was made, she reported visual auras over several weeks. All auras started with flickering lights in the upper temporal quadrants bilaterally and increased in size. The auras lasted for about 30 min and were sometimes followed by occipital headache, which started about 30 min after the aura. The headache was accompanied by nausea and lasted several hours. Between the attacks she was symptom-free. Magnetic resonance imaging (MRI) of the brain, performed elsewhere, was normal. Migraine with aura was diagnosed. Several prophylactic treatments including propranolol and sodium valproate were unsuccessful, but topiramate resulted in a decrease of the frequency.
Six weeks after the first visual auras occurred, she complained of transient numbness of the left arm followed, a few minutes later, by numbness of the lips on the left side. It lasted for about 1 week. Her medical history mentioned hypertension and smoking. The family history was negative for migraine and epilepsy. Neurological examination was normal. Repeat MRI of the brain showed several small cortical and subcortical ischaemic lesions (Figure 1). Duplex of her carotid arteries was normal and an EEG showed no abnormalities. She was diagnosed with cerebral infarction of the right hemisphere with several silent ischaemic lesions bilaterally. Suspecting cardiac embolism, a transthoracic echocardiogram was performed which showed a large myxoma of the left atrial wall. Three months after surgical removal of the myxoma, she was free of symptoms.
Second MR-scan of the brain (FLAIR) showing several small ischaemic lesions: (A,B) subcortical; (C,D) cortical.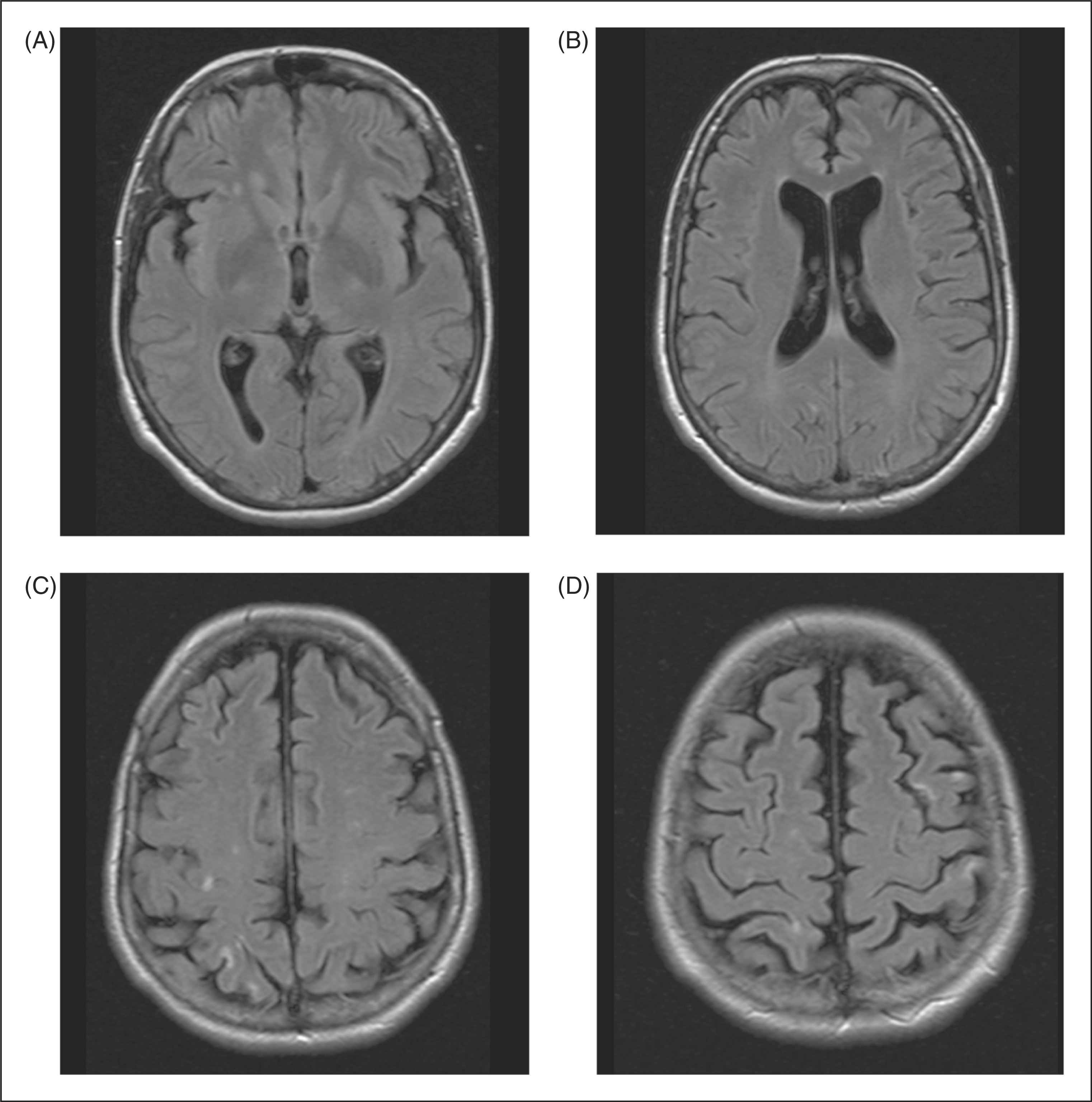
Discussion
Previous and present case reports of migraine associated with cardiac myxoma

F, female; M, male; MA, migraine with aura.
Remarkably, but not unexpectedly, the majority of cases are women (7/8). This would be expected as both migraine and cardiac myxoma are more prevalent among women. Migraine affects over 12% of the general population, with 6% in men and 18% in women (13,14). For cardiac myxoma, the female-to-male ratio varies from 2:1 to 3:1 (3). The mean age at time of diagnosis in the eight patients was 44 years, but some patients had suffered from migraine for years. In all cases where it was mentioned, the migraine ceased after removal of the myxoma, which implies a causal relationship.
Hypotheses on the underlying mechanism
Right-to-left-shunt and non-right-to-left shunt abnormalities associated with migraine with and without aura

+, Proven association; ± , doubtful association; –, no association; U, unknown association.
PFO is by far the most studied cardiac abnormality associated with migraine. A critical meta-analysis of 11 articles showed several biases in these studies, but still found an increased prevalence of migraine in patients with PFO (2). Several hypotheses that could explain the association between MA and PFO have been postulated. Cortical spreading depression (CSD) leading to MA might be triggered by either micro-emboli or vaso-active substances, such as serotonin, that have escaped from the filtering capacity of the lungs (19–25). The hypothesis that we find most likely is that migraine auras are triggered by micro-emboli. Recent experimental data support this hypothesis by proving that micro-emboli can trigger CSD in a mouse model, often without causing micro-infarction (26). In addition, Dalkara et al (27). reported that CSD could be provoked by a brief period of local hypoperfusion and suggested that migraine and stroke might both be triggered by focal cerebral hypoperfusion and, therefore, may be placed on a continuum of vascular complications. Furthermore, all previous mentioned conditions (Table 2), including cardiac myxoma, can trigger CSD if emboli are the mal-factor. In the case of a right-to-left shunt, systemic emboli cannot be captured in the pulmonary circulation and myxoma and other cardiac abnormalities can be a direct source of emboli. But how do micro-emboli trigger CSD? If small emboli reach the small vessels in the cortex for a brief period, they may induce CSD and aura in susceptible patients, perhaps by reactive vasodilatation mediated by vaso-active substances. In contrast, more prolonged occlusion of vessels deeper into the brain by a larger emboli may cause infarction.
Conclusions
Cardiac and non-cardiac right-to-left shunt conditions and cardiac structural disorders, including cardiac myxoma, may trigger cortical spreading depression leading to migraine with aura. The most plausible explanation is that (paradoxically) small emboli reach the brain and locally cause a spreading depression in a hyperexcitable brain. The risk of developing CSD triggered by micro-emboli may depend on the location and duration of hypoperfusion and the size of the emboli.