
Abstract
Objective: The study’s objective was to assess self-awareness and medical recognition of migraine and their determinants in Germany.
Methods: We conducted a nationally representative study of the general population of Germany (N = 7341, aged ≥18 years) by means of computer-assisted telephone interviews. Migraine was diagnosed based on the International Classification of Headache Disorders, second edition (ICDH-II).
Results: Twelve-month prevalence of ICHD-II-migraine was 10.6% (women 15.6%, men 5.3%). Seventy percent of ICDH-II-migraineurs recognised their headaches as migraine (moderate agreement between ICDH-II and self-diagnosis, κ = 0.46). Only 42% of migraineurs consulted a physician in the previous 12 months. Of those, 63% reported a medical diagnosis of migraine (moderate agreement, κ = 0.40). Women were more likely to be self-aware (odds ratio [OR] 1.81, 95% confidence interval [CI] 1.27–2.60), but the difference was no longer significant when adjusting for migraine features. Physician recognition was more likely in patients with higher educational level (high vs. low education OR 3.90, 95% CI 1.43–10.61 after adjusting for migrainous features). Best predictors for self-awareness and medical recognition of migraine were typical migraine accompaniments and greater headache intensity.
Conclusion: Self-awareness and physician recognition of migraine are low in Germany. Presence of typical migraine features and greater headache intensity facilitate medical recognition and awareness of migraine, especially in females.
Introduction
Although migraine is one of the most debilitating primary headache disorders and is associated with a considerable health-related impact (1–7), medical management of migraine patients in most countries remains unsatisfactory (1,7–10). Several potential barriers to optimal patient care have been identified, including lack of migraine awareness (8,9,11) and underconsultation among affected individuals (2,8,10,12–15) as well as under-recognition and undertreatment of migraine by health care providers (2,7–10,12,14,15). Only half of migraine sufferers consult a physician for headaches despite substantial disability (2,9,12,14) and half of migraineurs never receive a medical diagnosis of migraine (1,2,9–11,15).
Because some of these barriers to adequate migraine management may largely depend on sociocultural factors and specific patterns of health care use (16), the aim of this study was to assess self-awareness and the medical recognition rate of migraine and their determinants in a representative sample of the adult general population in Germany.
Methods
This study was conducted as part of a nationally representative survey of the adult population living in Germany, the German Telephone Health Interview Survey (GNT-HIS) 2004. The methods have been reported in detail previously (17). In brief, a large representative sample of the general adult population in Germany aged 18 years or older (N = 7341; 3545 men and 3796 women) was assessed by means of computer-assisted telephone interviews. Participants were contacted using a modified random-digit dialling sampling design (18) in combination with a next-birthday method to lower selection bias: the interviewer asked to speak with the person in the household aged 18 years or older who had the next birthday. The GNT-HIS had a response rate of 52.3% and covered various aspects of physical health, demographic and socioeconomic characteristics, lifestyle behaviour and health care utilization. Demographic characteristics and selected health care indicators of the study sample did not differ from distribution in the general population when compared to national population statistics, with the exception of moderate differences in the distribution of educational groups (17). The study was approved by the Federal Data Safety Commissioner.
All participants of the GNT-HIS were first screened for severe headaches by asking if they had suffered from headaches during the previous 12 months and if intensity of headaches had been (a) predominantly severe, (b) both severe and mild or (c) predominantly mild. Only participants with severe headaches fulfilling criterion (a) or (b) were further explored for migrainous headaches. A diagnosis of migraine based on the second edition of the International Classification of Headache Disorders (ICHD-II) (19) was assigned if participants fulfilled all of the following criteria: (1) severe headaches during the previous 12 months, (2) unilateral pain or pulsatile pain or pain aggravated by routine physical activity, (3) nausea or vomiting or photo- with phonophobia with headaches and (4) an attack duration of 4–72 hours. Migraine with visual aura was diagnosed if participants reported flickering lights, lasting at least five minutes, together with headaches. Migraine with and without aura were considered mutually exclusive. Complete data for classification of migraine status were available for 98.6% of the 7341 participants of the GNT-HIS.
Self-awareness of migraine was assessed by asking participants with severe headaches if they believed that their headaches were, at least in part, due to migraine. For assessment of a previous medical diagnosis of migraine, participants who had consulted a physician for headaches in the past 12 months were asked which subspecialty of medicine they had mainly consulted and which of the following diagnoses had been assigned to headaches by the treating physician: (1) sinus headache, (2) migraine, (3) tension-type headache or (4) “other diagnosis”.
Statistical analysis
For statistical analysis SPSS, version 18 (SPSS, Chicago, IL, USA), was used. Sampling weights were used to account for unequal sampling probabilities by household size and to reflect the distribution of the population with respect to age, sex and geographic region of Germany. The chi2-test was applied to assess differences of categorical variables. Student's t-test was used to test for differences in means. Correlation coefficient kappa (κ) was calculated to assess agreement between self-, physician- and ICHD-II-diagnosed migraine. A kappa of 0.0 is interpreted as evidence that the agreement is no better than chance alone, while a kappa between 0.81 and 1.00 demonstrates very good agreement. Values of ≤0.20, 0.21–0.40, 0.41–0.60 and 0.61–0.80 are interpreted as showing poor, fair, moderate and good agreement, respectively (20).
Sensitivity, specificity and positive predictive value of a self-diagnosis of migraine and a prior physician diagnosis of migraine for presence of ICHD-II-migraine were estimated.
Two separate multivariate logistic regression models were calculated to test for associations of various factors with self-awareness and correct medical diagnosis of migraine. The first model (Table 2) looked at self-awareness of migraine as a dependent variable among the 769 interview-diagnosed ICDH-II-migraineurs and included independent variables based on the prior hypothesis that both sociodemographic factors and migraine features are associated with self-awareness (sex, age, educational level, medical consultation for migraine, number of headache days, various headache characteristics and associated symptoms). The second model analysed 299 interview-diagnosed ICDH-II-migraineurs who had consulted a physician, had physician diagnosis of migraine as a dependent variable and included as independent variables the same sociodemographic factors as the first model except for physician consultation.
A two-sided significance level of p < 0.05 was adopted for all tests.
Results
The 12-month prevalence of severe headaches in unselected adults in Germany was 60% (women 66%, men 53%) and the 12-month prevalence of total migraine (including migraine with and without aura) as diagnosed by interview according to the ICHD-II-criteria was 10.6% (women 15.6%, men 5.3%). The prevalence of migraine with aura was 3.6% (women 5.6%, men 1.5%).
Sensitivity, specificity, PPV and NPV of a self-report of migraine and of a previous physician diagnosis of migraine for detecting ICHD-II-migraine (in %) among participants with severe headaches in the past 12 months.
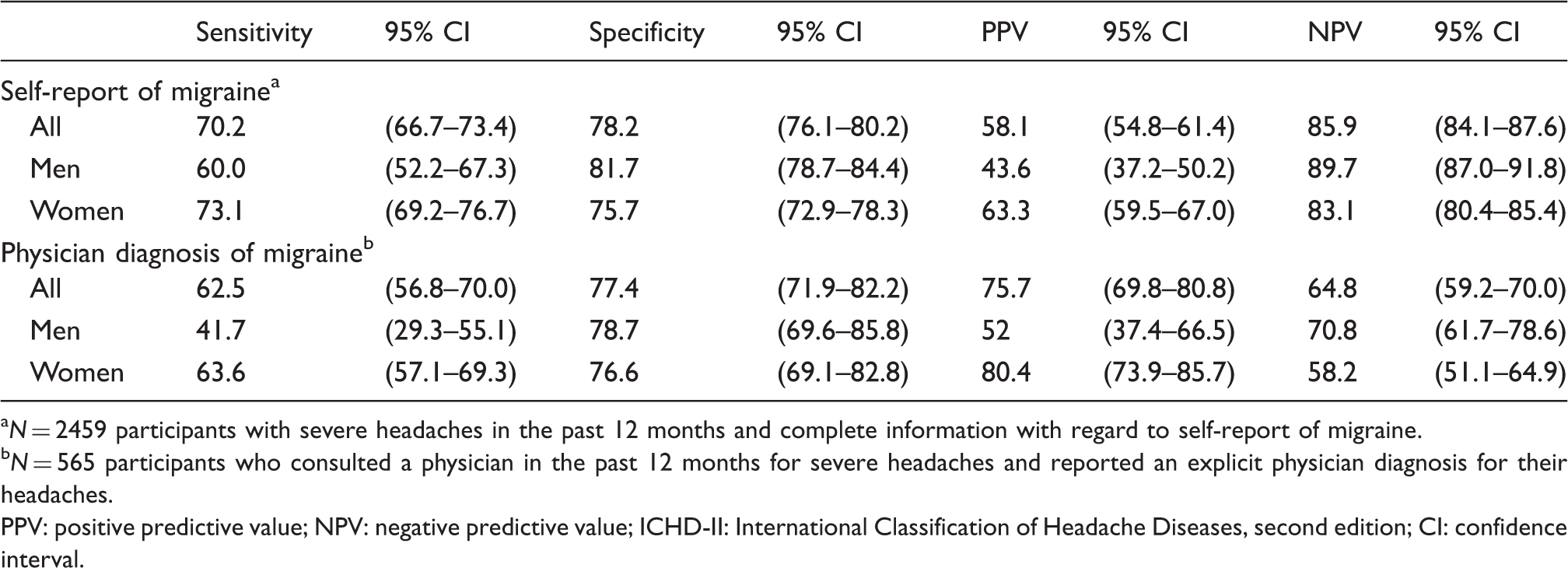
N = 2459 participants with severe headaches in the past 12 months and complete information with regard to self-report of migraine.
N = 565 participants who consulted a physician in the past 12 months for severe headaches and reported an explicit physician diagnosis for their headaches.
PPV: positive predictive value; NPV: negative predictive value; ICHD-II: International Classification of Headache Diseases, second edition; CI: confidence interval.
Predictors for self-awareness of migraine among interview-diagnosed ICHD-II migraineurs
Predictors for self-awareness of migraine among 769 ICDH-II-migraineurs. a

Adjusted for all variables in the table rows.
OR = 1 represents the reference value.
ICHD-II: International Classification of Headache Disorders, second edition; OR: odds ratio; CI: confidence interval; SD: standard deviation.
Women were more likely to be self-aware of migraine than men (73% vs. 60%, OR 1.81, 95% CI 1.27–2.60), while age and educational level had no effect on self-awareness in univariate analysis (Table 2). Medical consultation in the previous 12 months increased the likelihood of migraine awareness in migraineurs who had consulted a neurologist (OR 5.28, 95% CI 1.09–2.15) and, to a lesser extent, also in those who had consulted another specialist, compared to non-consulters (OR 1.53, 95% CI 1.62–17.18) (Table 2).
However, when adjusting for migraine features in multivariate logistic regression analysis, the effects of gender and medical consultation in the previous 12 months on self-awareness were no longer significant. Migraineurs with a high educational level were more likely to be self-aware of migraine than those with low educational level after correction for other factors (OR 2.42, 95% CI 1.29–4.54). Multivariate analysis largely confirmed the effects of typical migraine features on migraine awareness found in univariate analysis. The strongest associations were found for the factors vomiting and presence of both photo- and phonophobia, followed by unilateral pain, number of headache days, headache severity and visual aura (Table 2).
Predictors for a physician diagnosis of migraine among interview-diagnosed ICHD-II migraineurs who had consulted a physician in the previous year
Predictors for a physician diagnosis of migraine in 299 ICHD-II-migraineurs who had consulted a physician for migraine headaches in the previous 12 months. a

Adjusted for all variables in the table rows.
OR = 1 represents the reference value.
ICHD-II: International Classification of Headache Disorders, second edition; OR: odds ratio; CI: confidence interval; SD: standard deviation.
Multivariate analysis confirmed a strong association of educational level, typical migraine symptoms, including nausea or vomiting, presence of both photo- and phonophobia as well as unilateral pain, and headache severity with physician recognition of migraine in the previous year, while gender and the medical subspecialty consulted for headaches failed to show an effect after correction for migraine features (Table 3).
Discussion
The results of our large, population-based survey show that self-awareness and medical recognition of migraine are low in Germany. Only 70% of participants with migraine according to ICHD-II-criteria recognised their headaches as migraine and less than two-thirds (62.5%) of migraineurs who had consulted for headaches in the previous year (current consulters) reported that their treating physician had diagnosed them with migraine.
Only a few studies have assessed migraine awareness in population-based settings, reporting somewhat divergent results. Self-awareness of migraine in our survey lies within the upper range of previous estimates: in a sample of 3074 migraineurs recruited from several large US cities, only 53% recognised their headaches as migraine (11), while in two population-based studies carried out in France, migraine awareness rates ranged from 52%9 to 80%13 of individuals with migraine according to ICHD criteria. Physician recognition among current consulters for headache in our sample was similar to previously reported rates, ranging from 60% to 73% of migraineurs who ever consulted for migraine (12,14,21). When measured as the proportion of migraine sufferers who ever received a physician diagnosis of migraine relative to all individuals with a research diagnosis of migraine, the proportion of recognised migraineurs has been estimated at 38–56% in the United States and Europe (2,9,14,15), while slightly lower rates of around 35% have been reported for Latin American countries (10).
Some of the variability of migraine awareness among affected individuals and physician recognition of migraine may be explained by methodological differences of previous studies, including varying population samples and differing methods of ascertaining migraine recognition. Recognition rates are likely to be higher with the use of closed or multiple-choice questions that already suggest the term “migraine” compared to open questions. However, other factors, such as consultation behaviour, the level of expertise in migraine diagnosis among physicians as well as sociocultural differences in perception and acceptance of headaches and migraine presumably account for some of the variation found across countries.
Several clinical migraine features were identified in both univariate and multivariate analysis that increased the likelihood for self-awareness of migraine in our sample. The strongest effects were found for typical migraine accompaniments such as nausea and vomiting and occurrence of both photo- and phonophobia, followed by unilateral pain and visual aura. Occurrence of predominantly severe headache and a greater number of migraine attacks in the previous year also increased the probability of migraine awareness, which supports previous findings showing that severe intensity of headaches and a high impact of migraine on daily living promoted self-awareness of migraine in migraineurs in France (9).
Self-awareness of migraine did not differ by age, but women were more likely to recognise their migraine than men according to univariate analysis. However, multivariate analysis did not reveal gender as an independent determinant for self-awareness after adjusting for clinical migraine features and medical consultation in the previous year, suggesting that gender-related differences in migraine presentation and consultation behaviour most likely account for the disparity of migraine awareness in men and women. Female migraineurs are more severely affected by migraine headaches, as reflected by more frequent and severe headaches and greater disability due to migraine (5,17) and more frequently report typical migrainous symptoms such as nausea and photo- and phonophobia (5) than do male migraineurs. In addition, women in our sample were more likely to consult a physician for migraine (17), which also increased the likelihood of a self-report of migraine in this as well as in previous studies (9,10). Thus, a plausible explanation for our findings is that severe impact of headaches and typical migraine accompaniments, which are more prevalent in women, may facilitate migraine recognition in two ways: by prompting medical consultation and by making migraine headaches easier to recognise for both physicians and affected individuals. Our results are in line with previous studies, reporting higher migraine awareness among female migraineurs (9,11), but no strong effects of age on self-recognition of migraine (9,11). However, in contrast to a previous report that found no influence of educational level on migraine awareness (11), migraineurs with a high educational level in our sample were more likely to recognise their headaches as migraine than those with a low educational level after adjusting for other demographic factors and migraine characteristics.
Clinical migraine features that promoted a physician diagnosis of migraine in the previous 12 months were similar to those associated with self-awareness of migraine and largely confirm previous findings (2). However, in contrast to previous studies that reported a higher rate of medically diagnosed migraine in females and older age groups (2,14), we found no effect of gender or age on physician recognition of migraine in our sample. Medical recognition of migraine in the past 12 months was more likely in migraineurs with a higher educational level compared to those with lower educational levels in both univariate and multivariate analysis, which is in line with the finding that a higher household income promotes medical migraine recognition in the United States (2).
Less than half of migraine sufferers (42%) had consulted for migraine in the previous year despite occurrence of severe headaches, a proportion similar to consultation rates for migraine (current consulters) in the United States and Europe (2,12,16). Consultation of a neurologist increased the probability of a medical diagnosis of migraine by an OR of 3.14, compared to other specialists, according to univariate analysis. After adjusting for clinical migraine features, however, this difference was no longer significant, suggesting that migraine sufferers with typical migraine symptoms and severe headaches are more likely to consult a headache specialist and receive a migraine diagnosis. The great majority of migraine sufferers had consulted a GP or internist (72%), while only 11% were treated by a neurologist, a consultation pattern that closely resembles health care utilization for migraine in other countries (9,10,12,14).
The most frequent headache diagnosis assigned to migraineurs by their treating physician was tension-type headache, which accounted for more than half of all other non-migraine headache diagnoses (56%). Of note, “sinus headache”, which is a common diagnosis, assigned to up to 43% of medically unrecognised migraineurs in the United States (2,8,11,14,15), made up only a small fraction of non-migraine headache diagnoses in our sample (9%), indicating that perception and concepts of headache disorders may be culturally dependent.
Strengths and limitations of the study
Our survey comprised a large representative sample of the adult general population of Germany. Assessment of headache and migraine was embedded in a general health survey which covered a wide range of health-related issues and medical disorders. This should have minimized selection bias towards a higher response rate of individuals more severely affected by headaches, who may have a greater awareness for migraine.
There are a few potential limitations of our survey that need to be addressed. Our “gold standard” interview diagnosis was based on the current ICHD-II-criteria—however, with two modifications. First, the criteria applied did not specify the number of migraine attacks, as required by the ICHD-II (≥5 attacks) (19). By including participants with fewer attacks, who may not have received a physician diagnosis of migraine because they do not meet all ICHD-II-criteria, we may have underestimated migraine recognition in our sample. Secondly, we included only participants with severe headaches during the 12 months prior to assessment. This, on the contrary, might have led to an overestimation of migraine recognition, which is higher in the presence of severe headaches. Because a prior physician diagnosis of migraine was inquired about only among migraineurs who had consulted for headaches in the previous 12 months, our rate of medical migraine recognition reflects only recognition among current consulters.
Conclusion
Our findings of a low rate of self-awareness and physician recognition of migraine may have implications for health care management of migraine in Germany. As medical consultation may increase self-awareness of migraine, individuals suffering from severe headaches should be encouraged to seek medical care. Educational programs to raise public awareness about migraine symptoms and specific treatment options may reach those who do not seek consultation, especially male migraineurs, who are less likely to be aware of migraine than females.
Footnotes
Funding
We gratefully acknowledge the funding of the GNT-HIS by the German Ministry of Health.