
Abstract
FRAMIG 2000 is a population-based survey of medical and therapeutic management of migraine in France. A total of 312 migraine sufferers were first identified from a representative sample of 4689 adult subjects using a validated questionnaire based on the IHS migraine diagnostic criteria and administered by telephone. Subjects were then interviewed using a branching questionnaire and a computer-assisted interview technique. Although 80% were self-aware of their migrainous state, 82% of migraine sufferers had no medical follow-up for migraine. The proportion of migraine sufferers who did not consult decreased slightly with increasing migraine-related disability (from 87% for subjects in MIDAS grade I to 68% for those in MIDAS grade IV). Migraine sufferers declared to effectively control only four attacks out of 10 after the first intake of the usual treatment. Only 6% of subjects in the survey received a prophylactic treatment for migraine whereas 22% were in MIDAS grade III or IV. These data show that the burden of migraine does not result from a deficit in diagnosis but instead from a deficit in patient information on the proper use of current effective treatments of migraine.
Introduction
Population-based epidemiological surveys offer the advantage of providing a comprehensive overview of a common ailment, as opposed to the rare or serious aspects which are frequently focused on in specialized health care facilities. Moreover, such surveys are really suited to the study of migraine because a large proportion of migraine patients do not consult with a physician about their disease. The first nation-wide, population-based epidemiological survey of migraine in France was performed in 1989 by the GRIM Group, demonstrating its high prevalence and important personal impact (1). A second epidemiological survey carried out in France 10 years later by the same group showed stability of migraine prevalence and confirmed the high level of patient disability associated with migraine (2).
FRAMIG 1999 and FRAMIG 2000 are two population-based surveys also carried out in France in 1999 and 2000 which aimed to investigate some specific areas not covered by the aforementioned epidemiological studies, notably the extent of health care use by migraine sufferers, the therapeutic management of migraine attacks, and the course of migraine attacks after treatment. FRAMIG 1999 highlighted the widespread inadequate therapeutic management of migraine attacks by migraine sufferers, characterized by exceedingly high level of analgesic use (at the expense of specific treatments such as triptans) and underuse of prophylactic treatments (3). FRAMIG 2000, which is the subject of this article, aimed to provide a picture of medical and therapeutic management of migraine in a sample of French migraine sufferers, especially in relation to migraine-related functional status.
Materials and methods
General design of the survey
FRAMIG 2000 is a population-based telephone survey performed from December 12th to December 28th, 2000.
The survey sample of migraine patients was drawn in two phases from a telecommunication sample frame (∼20 000 subjects) matching the regional distribution of the French population, by the IPSOS public opinion poll institute. From this frame, subjects to be contacted were first identified by random digit dialing of computer-selected numbers. Up to 10 attempts were made to contact each individual. If the person called was absent or unwilling to respond or the line was engaged, calls were reiterated according to an automated dialing algorithm designed to handle all cases until the phone calls effectively resulted in making a contact or any attempt was abandoned.
In the first phase, respondents were screened and recruited while keeping predefined quotas (see below) (4). An eligible respondent was 18–65 years of age (for concerns about reliability of responses from too young or old subjects, and because assessing the use of triptans was one of the objectives of the survey), male or female, and had French as his/her mother tongue. No specific gifts or incentives were offered to the respondents. The number of respondents to be recruited (∼5000) was predetermined on the basis of the estimated frequency of migraine (defined according to the IHS criteria) in the French general population (∼8%) (1), a target being set of ∼400 migraine sufferers completing the whole interview. The group of respondents to be recruited for the survey matched the French general population aged 18–65 years for five quota systems: gender (two categories), age (five categories), socio-professional status (seven categories), region of residence (nine regions) and size of community (five categories), using as a reference the Employment Survey carried out yearly by the French Institut National des Statistiques et des Etudes Economiques (INSEE) (5).
In a second phase, respondents were administered a 123-item questionnaire intending first to identify migraine sufferers, next to collect information about features of migraine attacks, migraine-related disability, therapeutic management of migraine, migraine course after treatment, and migraine sufferers’ consultation behaviour and feelings about their disease. The questionnaire was administered by trained interviewers, using the Computer-Assisted Telephone Interview (CATI) technique. Such telephone interviews have been used in previous migraine epidemiological surveys with similar results to face-to-face interviews and surveys using postal questionnaires (6–9).
Identification and description of migraine sufferers
The first part of the questionnaire aimed to identify migraine sufferers. It was based on the migraine diagnosis criteria defined according to the first edition of the International Headache Society (IHS) classification for migraine without and with aura (categories 1.1 and 1.2) (10, 11). It comprised 11 questions administered according to a validated algorithm (12). Respondents were identified as migraine sufferers if they reported headaches manifesting in attacks and had had more than four attacks of headache in their lifetime exhibiting the following features: duration of 4–72 h without treatment, at least two of the four typical migraine characteristics (unilateral location, pulsatile quality, aggravation by routine physical activities, disruption of normal activities by necessitating cessation or lying down), and association with nausea and/or vomiting and/or with photo/phonophobia. Sensitivity and specificity of the questionnaire used for detection of migraine have been estimated at 95% and 78%, respectively (12). The occurrence of auras was not looked for, because aura visual disturbances are not easily distinguished from photophobia by migraine sufferers, and this did not adversely impact on survey objectives: therefore, subjects included might suffer from migraine without aura (category 1.1 of the 1st-edition IHS classification) or from migraine with aura (category 1.2 of the 1st-edition IHS classification) if their aura was followed by a headache with the features of migraine without aura. Subjects identified as migraine sufferers according to the preceding criteria were then asked about self-awareness of their disease, i.e. whether they had had previous knowledge that their headaches in reality were migraine attacks. Finally, only the subjects fulfilling all IHS diagnostic criteria for migraine with/without aura who, in addition, had experienced at least one attack during the last three months (owing to the concurrent use of MIDAS disability scale [see below] and to avoid recollection bias) were considered in the subsequent parts of the survey (subjects with ‘active migraine’).
Migraine impact on subject functioning was assessed by the five questions of the French version of the Migraine Disability Assessment Scale (MIDAS) (13) which focus on lost time (lost days and days with significantly reduced productivity) that occurred over the previous three months in three domains: school work or work for paid, household work or chores, and family, social and leisure activities. The sum of the scores at the five questions allowed assignment of one of the four MIDAS grades (score 0–5: grade I, minimal disability; score 6–10: grade II, mild disability; score 11–20: grade III, moderate disability; score 21 or greater: grade IV, severe disability) (14).
The following core interview involved a number of branching questions directed to features of migraine attacks (frequency, number of days with headache, intensity of headache scored on a numerical scale of 0 (no pain at all) to 10 (pain as bad as it can be), associated symptoms), therapeutic management of attacks (treatments used, time duration before the first treatment intake), migraine course after treatment (see below), recurrence of migraine headache (i.e. worsening of headache subsequent to initial partial relief) or relapse (i.e. return of headache after a patient was pain-free), recourse to medical assistance (physician consulted, or reasons for not seeking medical attention), and personal feelings about how migraine attacks are handled (feeling of enduring or controlling migraine attacks) and about the possibilities of migraine therapeutic management (feeling of resignation or confidence).
Regarding the course of migraine attacks after treatment, subjects’ responses to the question ‘After a first intake of your usual medication to treat a migraine attack, what is the development of your headaches?’ were classified according to the reported occurrence of four possible patterns of development: ‘absence of relief’ (i.e. no change in the course of the attacks after the first treatment as compared to no treatment), ‘no substantial relief’ (i.e. partial relief with no appreciable improvement in the general condition), ‘substantial but incomplete relief’ (i.e. partial relief with clear-cut improvement in the general condition), and ‘complete relief’ (suppression of all migraine-related symptoms). One individual subject might report several possible patterns of development of his migraine attacks if he/she usually experienced more than one, depending on the attacks treated. For further analysis, in order to reduce recollection bias, subsequent questions regarding development of attacks after treatment were about the last 10 attacks.
Data analysis
Categorical variables were summarized by the corresponding percentages in the relevant subject groups. Between-groups differences were evaluated using the Pearson χ2 test. Contingency tables involving ordinal scales (e.g. MIDAS grade) were analysed by the test of Yates. Migraine headaches scored more than 7 on the scale of 0–10 were considered of high intensity. Since migraine sufferers might experience headaches of varied intensity across successive attacks, the proportion of patients with average headache intensity ≤ 6 who also reported occasional headaches of high intensity (>7) was determined. Continuous variables were summarized by descriptive statistics (mean and standard deviation (SD), and/or median and range). Where appropriate, between-groups differences were compared by the Student t-test (if the size of the groups to be compared was > 30). Statistical significance was considered at P < 0.05.
Results
Development of the survey
A total of 18 259 phone numbers were called, of which 8401 (46.0%) were not retained for the survey owing to no response/recorded message (3762, 20.6%), false number/busy line/telecopy (1169, 6.4%), inability of respondent to answer the questions for any reason (language, unavailability, or other reason, 621, 3.4%), subject falling outside quotas (2683, 14.7%), or end of survey (166, 0.9%). Finally, 5169 subjects (28.3% of phone calls) refused to participate (4568 at once, 25.0%; 601 during the interview, 3.3%), and 4689 (25.7%) eligible respondents completed the whole interview.
The first part of the questionnaire made it possible to identify 383 migraine sufferers (categories 1.1 & 1.2 of the 1st-edition IHS classification: 8.2% of eligible respondents), of whom 312 (6.7% of eligible respondents) had ‘active migraine’ (categories 1.1 & 1.2 of the 1st-edition IHS classification, and at least one migraine attack during the last three months). Of these, 248 (79.5%) were self-aware of their migrainous state while 64 subjects (20.5%) were unaware.
Demographic characteristics of the respondent and migraine-suffering subject samples
The demographic characteristics of the sample of 4689 respondents are provided in Table 1 and compared to those of the French general population (5).
Demographic characteristics of the 4689 participants in the FRAMIG 2000 survey compared to those of the French general population of subjects aged 18–65 years

initial sample of 4689 subjects significantly different from the French general population (P < 0.001).
The initial sample of 4689 respondents was representative of the French general population aged 18–65 years for the quotas of gender, age distribution, region of residence, and size of community. However, subject distribution across socio-professional categories was significantly different (P < 0.001), due to slightly lower proportions of subjects in the craftsmen/shopkeepers and workers categories and a slightly higher proportion of subjects in the middle executives category, as compared to the French general population (Table 1).
The sample of 312 migraine sufferers was characterized by a predominance of female subjects (female/male sex ratio: 2.67/1) and a majority of subjects in the age class 30–49 years (56.1%).
Main characteristics of migraine
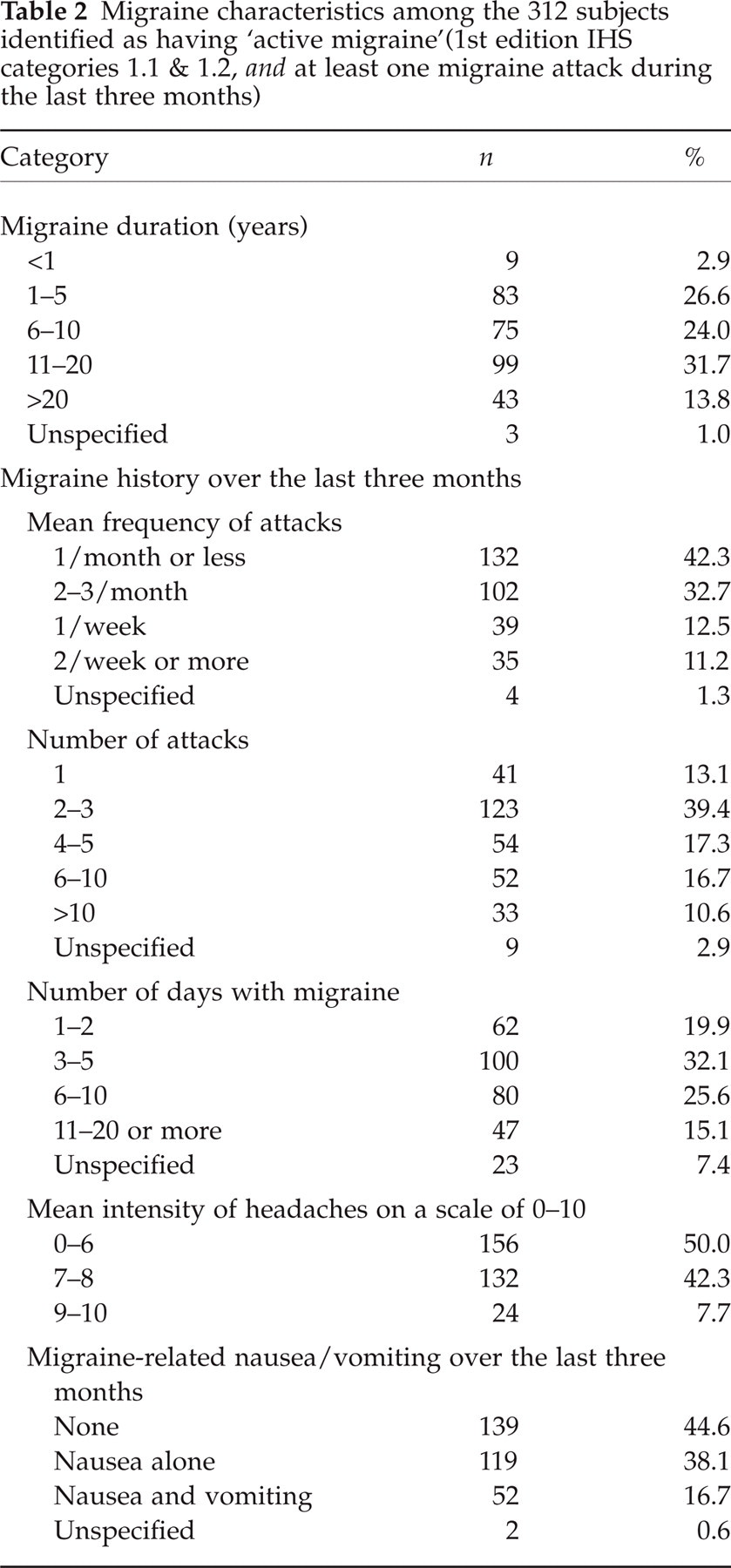
Characteristics of migraine in the sample of 312 migraine sufferers are displayed in Table 2. Migraine history duration (mean: 12.6 ± 9.3 years) ranged evenly between one and 20 years for the greatest part of the subject sample (82.3% of migraine sufferers). The frequency of attacks over the last three months was one per month or less in next to half subjects (42.3%), and two or three per month in one third (32.7%). Half of migraine subjects (56.7%) had had two to five attacks. Attacks had lasted for a total of three to 10 days (57.7% of subjects). One tenth of subjects had had two or more attacks per week (11.2%) and a total of more than 10 attacks over the last three months (10.6%). Mean number of attacks and mean number of days with migraine headache during the last three months were 5.5 ± 6.6 and 6.9 ± 6.8, respectively, showing that the average duration of an attack was more than one day. Migraine headache intensity was usually 7 or greater on the 0–10 scale for 50% of subjects (mean value for the whole subject sample: 6.5 ± 1.6). For more than half of subjects (54.8%), migraine attacks were associated with nausea alone or nausea and vomiting. Worthy of note, some migraine sufferers reported two types of migraine headaches: one third (36%) of those subjects who declared migraine headache average intensity ≤ 6 had also experienced occasional attacks with headache intensity > 7 during the last three months. In fact, 44% of migraine sufferers admitted that they were unable, at the start of a migraine attack, to predict whether it was going to be of mild or severe intensity.
Migraine characteristics among the 312 subjects identified as having ‘active migraine’(1st edition IHS categories 1.1 & 1.2, and at least one migraine attack during the last three months)
Migraine-related disability
Of the 312 subjects with ‘active migraine’, 284 (91.0%) could be assigned a MIDAS grade (the remaining subjects failed to give a precise answer to one or several of the five questions of the MIDAS scale). For these subjects, mean MIDAS score was 8.3 ± 12.3 and distribution by MIDAS grade was as follows: 222 (78.2%) subjects had grade I (minimal) or II (mild) disability, whereas 62 (21.8%) had grade III (moderate) or IV (severe) disability (Table 3).
Characteristics of migraine attacks, drug intakes, consultation rate, migraine sufferers’ feelings about management and therapy of migraine attacks, as a function of MIDAS disability grade

All value are given as no. of patients (%) except where marked otherwise.
P < 0.01 vs. grade I;
P < 0.05 vs. grade II;,
on a scale of 0–10;
n = 305;
n = 158;
n = 58;
several responses allowed.
MIDAS grade did not show any directional trend with migraine history duration but increased with the mean number of attacks over three months and with the mean number of days with migraine headache. In addition, MIDAS grade was loosely related to migraine headache intensity, and also related to the number of drug units taken to treat a single migraine attack. Finally, the proportion of patients free from nausea and vomiting decreased from the subsets of subjects in MIDAS grades I and II (53.4% and 44.3%, respectively) to those of subjects in grades III and IV (23.5% and 25.0%, respectively) (Table 3).
Medical consultation and follow-up, personal feelings about the disease
Migraine subjects’ consultation status is provided in Table 4. Eighty-two percent of migraine sufferers had no medical follow-up for migraine: 23% had never got on this subject with a physician during a consultation, while 59% had consulted previously for migraine but had lapsed consulting (i.e. gave up thinking of consulting) and had remained without any follow-up for a mean of 2.8 ± 3.1 years (median: 1.3; range: 0.08–15).
Characteristics of migraine sufferers (age, sex ratio) and medical follow-up, along with reasons for not consulting/lapsing consulting, according to the consultation status
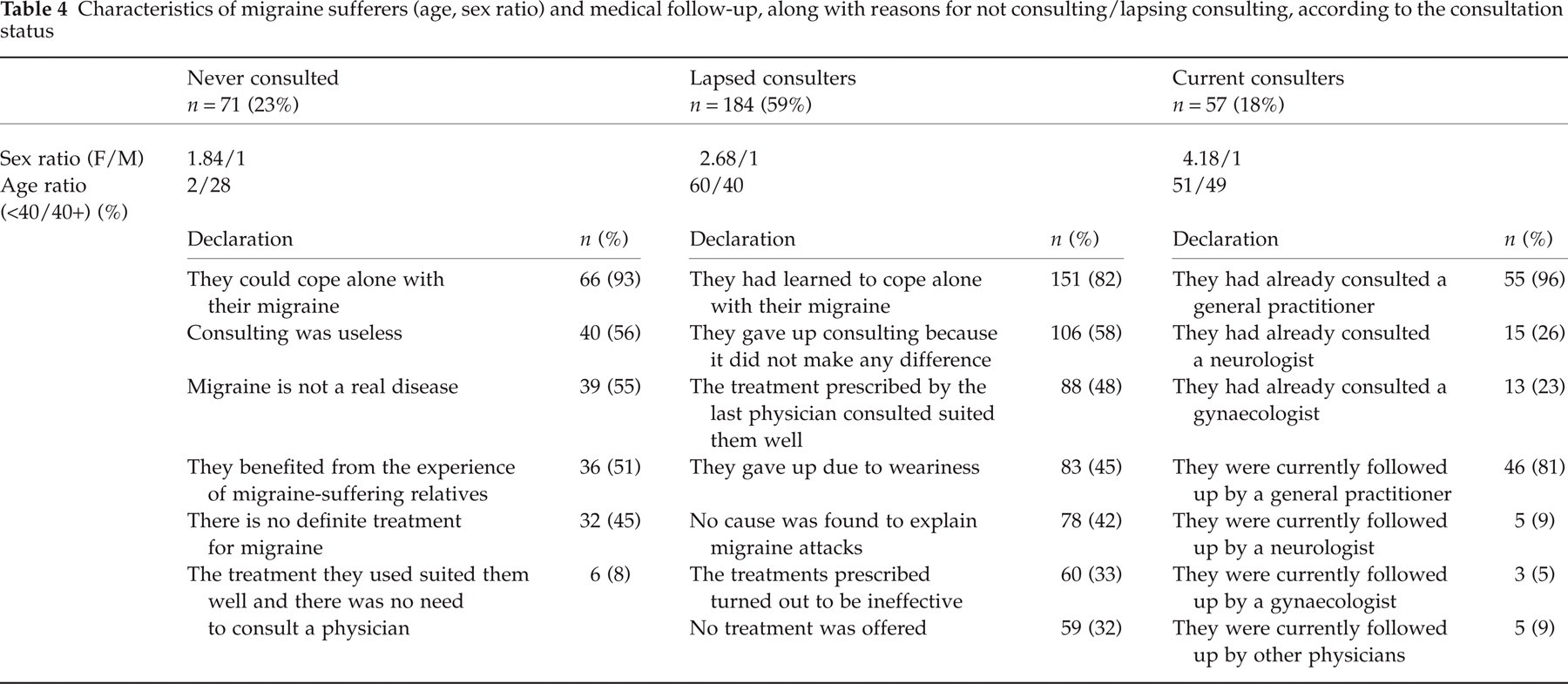
Among migraine subjects who had never consulted for migraine, there were more men (female/male sex ratio of 1.84/1 as compared to 2.67/1 in the whole sample of migraine subjects) and more young subjects (72% aged < 40 years as compared to 61% in the whole sample). Approximately half (56%) migraine subjects who had never consulted considered that consulting with a physician was useless, or that there was no definite treatment for migraine (45%). Most subjects (93% of subjects who had never consulted) thought that they could cope alone with their migraine (Table 4).
Approximately half (58%) migraine subjects who had lapsed from consulting for migraine considered that consulting with a physician made no difference. Forty-eight percent of subjects had lapsed because the treatment recommended by the last physician consulted (either a nonprescription drug or a drug subsequently prescribed in other circumstances) suited them well. Other reasons for lapsing included weariness, no cause found for migraine attacks, inefficacy of treatments prescribed and/or no treatment offered. Most subjects (82%) who had lapsed from consulting declared that they had learned to cope alone with their migraine (Table 4). Migraine sufferers who had lapsed consulting had previously consulted with a mean number of 2.4 ± 2.9 physicians (not more than three physicians for 86% of them), mostly general practitioners (93%), gynaecologists (20%) and neurologists (6%), with no appreciable differences between migraine subjects self-aware of their disease and those not aware. Among migraine sufferers self-aware of their disease, 81% had previously consulted for migraine but only 20% were followed up medically at the time of the survey.
Among migraine subjects who still consulted for migraine at the time of the survey, there were more women (female/male ratio of 4.18/1 as compared to 2.67/1 in the whole sample of migraine subjects) and more subjects aged 50 years and greater (25% as compared to 16% in the whole sample). Migraine sufferers still medically followed up had previously consulted mainly with a general practitioner (96% of subjects), a gynaecologist (23%) or a neurologist (26%). However, only 9% of subjects were still followed up by a neurologist and 5% by a gynaecologist (Table 4). Eighty-one percent of them were followed up by a general practitioner, and the mean duration of follow-up had been 5.5 ± 5.1 years.
As MIDAS grade increases, migraine sufferers’ consultation rate increases (from 13.0% for subjects in MIDAS grade I to 32.1% for those in grade IV) and the rate of no medical follow-up (subjects who never consulted or had lapsed consulting for migraine) slightly decreases (from 87.0% for subjects in MIDAS grade I to 67.9% for those in grade IV) (Table 3) (Yates test: P < 0.05).
Fifty-three percent of all 312 migraine sufferers had a feeling of enduring their migraine attacks or of resignation towards the possibilities of migraine medical management, whereas 43% and 46%, respectively, had a feeling of control over the attacks or of confidence in treatments. More subjects still consulting had feelings of enduring the attacks and of resignation as compared to subjects who had never consulted (feeling of enduring the attacks: 63% vs. 38%, P < 0.01; feeling of resignation: 65% vs. 41%, P < 0.01). As expected, the negative feelings of enduring the attacks and resignation increased with MIDAS grade while the positive feelings of controlling the attacks and absence of resignation tended to decrease (Table 3).
Therapeutic management of migraine attacks
Of the 32 (10%) migraine subjects who said they took a prophylactic treatment for migraine, only 19 (6%) actually took a true prophylactic treatment, while 13 (4%) mistakenly considered the analgesics they took daily as prophylactic treatments.
Conversely, nearly all (97%) migraine sufferers treated most or all migraine attacks:
44% systematically, right from the beginning of the attack;
31% after headache had been persisting for some time: treatment was then taken after a mean time-lag of 6.4 ± 11.9 h;
22% after headache intensity had strengthened: treatment was then taken after a mean time-lag of 5.1 ± 8.9 h.
Medications that migraine sufferers reported to take usually for the acute treatment of migraine comprised paracetamol which was used by a majority (60%) of subjects, followed by aspirin (29%), nonsteroidal anti-inflammatory drugs (NSAIDs) (28%) and opiates (23%) (Fig. 1). Triptans were used by only 8% of migraine subjects, of whom two thirds took them as single or first-line therapy.

Drugs used by migraine sufferers for the acute treatment of migraine, including the proportions of subjects who cited each individual drug and who took one (▪), two (), three or more (□) units of the drug for the treatment of a single attack; unspecified ( ). An individual migraine sufferer might cite several drugs. Top of columns: proportion (%) of subjects (n = 312) who cited each drug Inside columns: proportion (%) of subjects who cited drugs from only one pharmacological class (n = 157) and who used one, two, and three or more units of each individual drug for the treatment of a single migraine attack.
). An individual migraine sufferer might cite several drugs. Top of columns: proportion (%) of subjects (n = 312) who cited each drug Inside columns: proportion (%) of subjects who cited drugs from only one pharmacological class (n = 157) and who used one, two, and three or more units of each individual drug for the treatment of a single migraine attack.
More than one third of migraine subjects (38%) usually took a second and 17% a third type of medication to treat a single attack; 4% took four and 2% five or more different drugs in a single attack. Nearly half (48%) subjects used drugs from at least two different pharmacological classes, of whom 11% took drugs from three classes and 2% from four classes. Overall, 60% of subjects took four or more drug units, and 39% six or more units (Fig. 2), giving a mean number of drug units per attack of 5.8 ± 5.4. Migraine-related disability did not appear to influence markedly the number of drug units taken in one attack by subjects in MIDAS grades I to III, but subjects in MIDAS grade IV took six or more drug units more frequently (64% of subjects) (Fig. 2). The proportions of subjects who cited drugs from only one pharmacological class (157 subjects) and used one, two, and three or more drug units for the treatment of a single migraine attack are displayed by pharmacological class in Fig. 1. Triptans differentiate from other therapeutic classes by the high proportion of migraine sufferers (87%) who usually took only one drug unit during a single migraine attack: median numbers of drug units and corresponding ranges were 1.0 (1–3) for triptans, 1.7 (1–12) for NSAIDs, 2.5 (1–8) for aspirin, 2.5 (1–36) for opiates, and 2.8 (1–24) for paracetamol.
Proportions of migraine sufferers who reported to take one (▪), two or three (), four or five (), or six or more (□) medication units for the treatment of a single attack of migraine, in the whole group of migraine subjects and as a function of MIDAS disability grade.
Treatments taken by subjects who had never consulted for migraine (nonprescription drugs) were recommended by close relations (41% of subjects) or by a pharmacist (25%), or bought according to advertisements (8%). Treatments taken by subjects who had lapsed from consulting for migraine (either nonprescription drugs or drugs subsequently prescribed in other circumstances) were mainly those recommended by the last physician consulted (44%), or by close relations (22%) or a pharmacist (15%).
Possible patterns of development of migraine attacks after the first treatment intake
Three hundred and one migraine subjects who used a medication to treat their migraine attacks reported at least one of the four possible patterns of development of migraine attacks (‘absence of relief’, ‘no substantial relief’, ‘substantial but incomplete relief’, ‘complete relief’) after the first intake of the usual medication: 48.5% mentioned only one possible development, 23.9% two, 15.6% three, and 12.0% four possible developments (mean number of possible developments cited by migraine subjects: 1.9 ± 1.1). The pattern of development most frequently cited was ‘no substantial relief’ (65.8% of subjects).
Migraine sufferers self-aware of their disease cited ‘complete relief’ and ‘substantial but incomplete relief’ less frequently (32% and 42%, respectively) than those who were unaware (45% and 63%, respectively, P < 0.05 and P < 0.01). Increase in the degree of disability as assessed by MIDAS grade was associated with increasing numbers of subjects reporting ‘absence of relief’ among those in MIDAS grades II and III(61% and 58%, respectively, vs. 35% for those in MIDAS grade I, P < 0.01 and P < 0.05). Conversely, increase in disability grade tended to reduce (although not significantly) the number of subjects reporting ‘complete relief’(21% of patients in MIDAS grade IV vs. 41% of those in grade I).
The majority of migraine sufferers reporting ‘absence of relief’ or ‘no substantial relief’ after the first treatment took a second treatment (66% and 59%, respectively), most often the same as the first one (77% in both cases).
After a successful first treatment, 21.6% of migraine sufferers (65/301) mentioned either recurrence of migraine headache after initial ‘substantial but incomplete relief’ (28 subjects, 9.3%) or headache relapse after initial ‘complete relief’ (37, 12.3%). The majority of these subjects (75% and 76%, respectively) took a second treatment, most often the same as the first one (86% and 89%, respectively).
Patterns of development of migraine attacks after the first treatment, as reported by migraine sufferers across the last ten migraine attacks
Migraine sufferers gave an estimation of the proportion out of 10 of their migraine attacks which pertained to each of the four patterns of development. The proportion was 1.7 ± 3.2 attacks/10 for ‘complete relief’, 2.3 ± 3.3 attacks/10 for ‘substantial but incomplete relief’, 3.7 ± 3.8 attacks/10 for ‘no substantial relief’, and 2.3 ± 3.3 attacks/10 for ‘absence of relief’. As a result, effective control of migraine attacks was reported to occur in only four out of 10 migraine attacks after the first intake of the usual treatment.
Here again, migraine sufferers self-aware of their disease showed a lower rate of ‘substantial but incomplete relief’ (2.0 ± 3.2 attacks/10 as compared to 3.4 ± 3.8 attacks/10 for subjects unaware, P < 0.01). Increase in MIDAS disability grade was associated with increasing mean numbers of attacks with ‘absence of relief’ (P < 0.01 vs. grade I for subjects with disability grades II and III), and with decreasing mean numbers of attacks with either ‘substantial but incomplete relief’ or ‘complete relief’ (P < 0.05 vs. grade I for ‘complete relief’ in subjects with grade III disability) (Fig. 3).
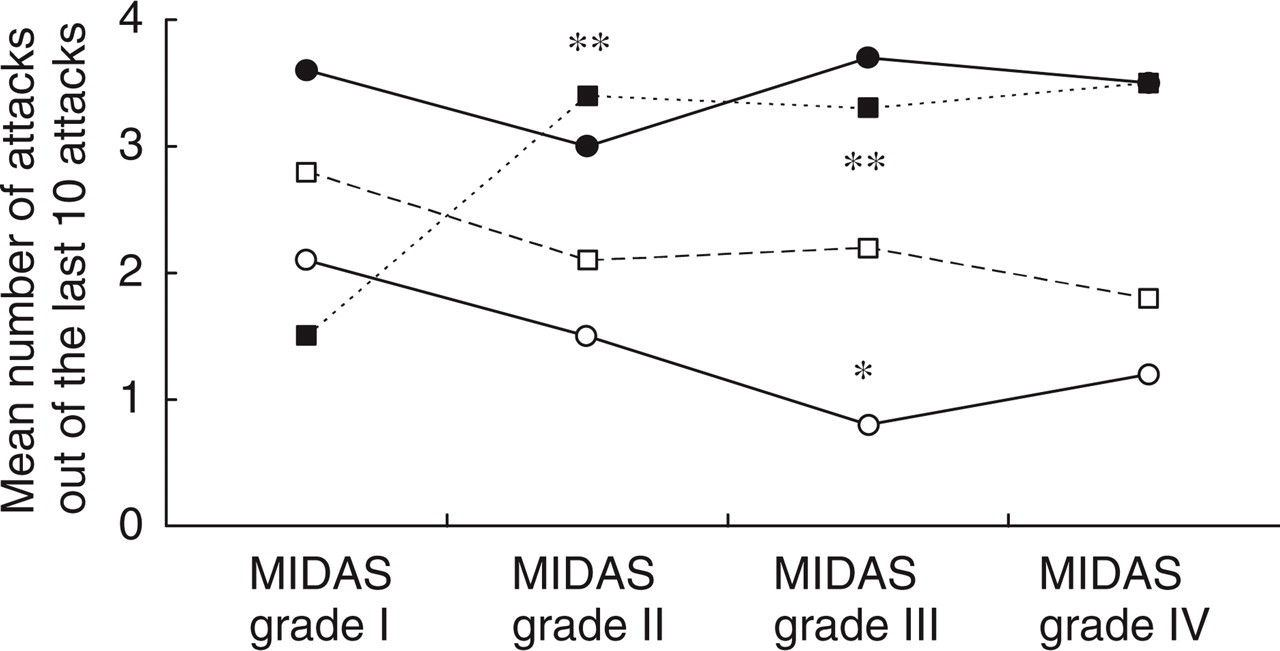
Possible patterns of development of migraine attacks after the first intake of the usual acute treatment of migraine, as estimated across 10 attacks by 274 migraine sufferers with assessable MIDAS grade, in terms of MIDAS disability grade. ▪ absence of relief; • no substantial relief; □ substantial but incomplete relief; ○ complete relief. ∗P < 0.05, ∗∗P < 0.01 versus grade 1.
Discussion
FRAMIG 2000 is a cross-sectional survey which was carried out in France as an extension of FRAMIG 1999, and aimed to go deeper into the analysis of medical and therapeutic management of migraine, especially in relation to patient migraine-related functional status.
Results show that more than half migraine subjects interviewed in FRAMIG 2000 had a frequency of migraine attacks of two per month or greater, and that half had a mean headache intensity of 7 or greater on a 0–10 scale, characterizing attacks mainly of fairly great intensity. Forty-three percent of subjects exhibited mild to severe migraine-related disability as assessed by the MIDAS grade. Nearly 80% of subjects were self-aware of their migrainous state, a proportion comparable to that observed in FRAMIG 1999(73%) (3). Migraine sufferers, mainly female (72.8%) and young subjects, included higher proportions of employees and middle executives and a lower proportion of workers than the French general population aged 18–65 years, as previously reported (1).
Migraine-related disability as evaluated by the MIDAS grade was not found to be influenced by migraine history duration but, as expected, increased with the frequency and number of migraine attacks and the number of days with headache over three months, especially for patients in MIDAS grade IV. The relationship between MIDAS grade and migraine headache intensity was less tight, but was reinforced by the parallel relationships with the number of drug units taken for the treatment of a single attack and with the incidence of nausea and vomiting, two parameters which also reflect the severity of migraine attacks.
One striking feature of FRAMIG 2000 is the high proportion (82%) of migraine sufferers who do not consult for this disease. Migraine sufferers who do not consult for migraine are preferentially young and male, and have more frequently a feeling of control over their attacks, whereas subjects who continue to consult and thus seek medical assistance have more frequently a feeling of enduring the attacks. Only a minority (20%) of subjects self-aware of their disease who have consulted for migraine are medically followed up. Yet, subjects aware of their migrainous state are more often affected by nausea or vomiting, and generally report greater disturbance of their familial, social and professional life (3). FRAMIG 2000 results confirm that migraine-related disability (as assessed by MIDAS grade) reduces only moderately (from 87.0% for subjects in MIDAS grade I to 67.9% for those in grade IV) the proportion of migraine subjects who do not consult (Table 3). Overall, this suggests that the high proportion of migraine sufferers who are not medically followed up does not result from a deficit in diagnosis of the disease, but instead from a deficit in patient information on the current possibilities of migraine medical management. In fact, reasons put forward by migraine sufferers who have never consulted or have lapsed from consulting clearly reflect their opinion that they can manage their migraine by themselves or with the help of close relations, and that consulting is useless. Nonetheless, it is reassuring to note that 25% of migraine subjects who have never consulted for migraine use a treatment recommended by a pharmacist, and that 44% of those who have lapsed from consulting for migraine continue to use the treatment recommended by the last physician consulted (nonprescription drug or drug subsequently prescribed in other circumstances).
An appreciable difference between migraine subjects who had lapsed from consulting and those who were still consulting for migraine concerns the proportion of subjects in each group who had previously consulted with a neurologist: this proportion was 26% among those who were still medically followed up vs. 6% among subjects who have lapsed from consulting. Nevertheless, only a small proportion (9%) of subjects medically followed up for their migraine at the time of the survey were still followed up by such a specialist.
Another fact revealed by the FRAMIG 2000 survey is that subjects lapsing from consulting do so after having consulted with a relatively small number of physicians (2.4 on average in FRAMIG 2000), mostly general practitioners. Furthermore, migraine subjects who are followed up by a general practitioner have been consulting with the same physician for a relatively long time period (5.5 years on average in FRAMIG 2000). These data contradict the belief shared by many people that migraine sufferers are frequently prone to ‘medical wandering’. The small number of physicians consulted before lapsing probably also reflects the known tendency of migraine sufferers for resignation (more than half subjects in FRAMIG 2000), perhaps partly the consequence of the inadequate medical care they were as yet offered for their disease.
The low consulting rate of migraine sufferers may be a consequence of the low rate of success of the treatments they usually use: ‘absence of relief’ or ‘no substantial relief’ is observed in an average of six attacks out of 10. In fact, most migraine sufferers in the survey treated migraine attacks with nonspecific treatments. It is tempting to relate the reported low rate of significant relief of migraine headache to the obvious underuse of specific treatments. Moreover, the way migraine sufferers use treatments is often far from optimal: only a minority (44%) use to take a treatment right from the beginning of the attack, whereas a majority (53%) mistakenly take it after headache has persisted for some time or worsened substantially. As a result, many migraine subjects take their treatment several hours after the start of the attack. This is in contradistinction with the current French recommendations that any type of treatment of migraine attacks should be taken as early as possible, particularly triptans for which some data suggest that undue delay of intake might reduce the rate of complete relief, increase the rate of recurrence/relapse and adverse effects, and prolong migraine-related disability (15). Moreover, most subjects who take a second treatment, for either insufficient effectiveness or recurrence/relapse of migraine headache, use the same drug as for the first intake. These observations reflect the lack of information of migraine sufferers or unwillingness to follow directions for use of acute treatments of migraine since, first, clinical studies showed that most active treatments such as triptans usually afford headache relief in less than two hours (16) and, second, that in case of treatment inefficacy a different second-line treatment must be tried. Furthermore, the use by many migraine sufferers of multiple treatments from different therapeutic classes to treat a single migraine attack is also not in accordance with the current recommendations. First, the combination of several different treatments taken consecutively implies immediate iatrogenic risk. Second, systematic treatment of every headache with multiple nonspecific medications may entail the risk of drug overuse, since nearly half patients (44%) are unable, at the start of a migraine attack, to predict whether headache will be of mild or severe intensity. Careful education of patients is therefore required to promote proper use of specific treatments of migraine attacks, as it appears from FRAMIG 2000 data that in most cases a single intake of a triptan is generally sufficient to effectively control a migraine attack.
One noteworthy fact shown by FRAMIG 2000 is that headache recurrence/relapse does occur not exclusively after treating an attack with a triptan as commonly stated (17), but just as well after using nonspecific analgesics. A wide spread belief is that headache recurrence/relapse occurs more frequently with specific treatments of migraine attacks relative to nonspecific treatments. This opinion is a probable consequence of the fact that recurrence/relapse was mostly assessed in studies performed on recent specific treatments which induce more frequent initial relief (18). In FRAMIG 2000, paracetamol was used by 60% of migraine sufferers, aspirin by 29%, and NSAIDs by 28%, while triptans were used by only 8%. Nevertheless, headache recurrence or relapse was reported by 21.6% of migraine sufferers who reported substantial or complete relief after the first treatment intake of their usual medication. This indicates that headache recurrence/relapse may actually be unrelated to the type of treatment used, but instead be an intrinsic pathophysiological feature of migraine (19).
Only 6% of subjects in the survey were receiving a real prophylactic treatment of migraine. According to the current French recommendations (15), a prophylactic treatment should be prescribed on the basis of frequency, intensity and familial/social/professional disability, when a patient has been taking an acute treatment (even effective) six to eight days per month across the last three months. Considering that, in FRAMIG 2000, 22% of migraine sufferers were in MIDAS grade III or IV (Table 3), on the one hand, and that, on the other hand, a quarter of subjects had one migraine attack per week or more (Table 2) and that half of subjects took two or three types of medications to treat a single attack, surely more than the observed 6% proportion of subjects should have been receiving a prophylactic treatment of migraine. Prophylactic treatment, which aims to reduce the frequency and severity of migraine attacks, might constitute an effective way to prevent overuse of specific or nonspecific treatments of migraine attacks (15) and the development of chronic daily headaches that affect nearly 3% of the French general population (20).
FRAMIG 2000 was performed on a subject sample drawn from a telecommunication sample frame by random digit dialing, and carried out using CATI interviews. The initial sample of 4689 respondents recruited for the survey was representative of the French general population aged 18–65 years for gender, age distribution, region of residence, and community size. However, this initial subject sample differed from the general population with slightly lower proportions of subjects in the categories of workers and craftsmen/shopkeepers, and a slightly higher proportion in the category of middle executives. The method used for subject selection is theoretically the best one, although it may not allow totally optimal response rates, alienating owners of silent numbers (21). Regarding the way the questionnaire was administered, telephone interviews were preferred to postal questionnaires, though less expensive and easier to apply, because of poor response rates, inadequate completion, inapplicability of intricate hierarchical questionnaires, and influence of family members. In addition, with telephone interviews, completion of the questionnaire is not dependent on literacy, items are responded in the right order and there are no missed ones, response reliability is greater due to better anonymity and subject's attention, and the influence of other members of the household can be minimized. The interview appointment may be set to suit the patient, thus helping to prevent selection bias against patients in terms of employment or education (6). Telephone interviews may generate difficulties however, in terms of the complexity of the questions that can be asked, and telephone samples may be significantly higher in residential social status (22, 23). This may account for the slightly lower proportion of subjects in the workers category observed in the FRAMIG 2000 initial sample of 4689 subjects contacted as compared to the French general population. Nonetheless, many studies conclusively showed that results of telephone interviews are well correlated with those of face-to-face interviews or supervised self-administered questionnaires (6–9). Finally, data acquisition and algorithm progress during CATI interviews are made greatly easier by the use of a computer.
Migraine-sufferer sample size was originally fixed at ∼400 since this number provides satisfactory conditions for the study of three or four subject subgroups of convenient size. The frequency of ‘active migraine’ (at least one attack within the last three months) in the general population was expected to be ∼8%, somewhat lower than that determined in FRAMIG 1999 (12.5%) in a similar subject population and using the same methodology, but in which only one attack during the last 12 months was required for recruitment to the survey (3). In reality, the frequency of ‘active migraine’ showed to be slightly lower than expected (6.7%), resulting in a migraine-sufferer sample size of 312 subjects, still compatible with the objectives of the survey.
Conclusion
FRAMIG 2000 survey confirms the persisting low rate of migraine sufferers who consult with a physician for migraine, even among those who are self-aware of their disease and sustain pronounced impact of migraine on their quality of life. This low rate of consulting appears to result both from a lack of information of migraine subjects on the possibilities and proper use of current treatments for migraine, and from a striking resignation that rapidly lead them to lapse from consulting. An important consequence of low rate of medical follow-up is the anarchical use of nonprescription drugs, which can lead to drug overuse and chronic daily headaches, while prophylactic and specific treatments are largely underused.