
Abstract
We report the case of a 31-year-old man with a history of migraine with aura who was admitted to our emergency department because of a sudden onset of severe bilateral facial pain radiating bilaterally into the medial cervical region after defecation. The pain was accompanied by scotomas in the right visual field and hypaesthesia in both upper limbs. Imaging of the aorta and supra-aortic vessels revealed a type A aortic dissection. Subsequently, the patient received an aortic valve replacement and an aortic tube graft.
After the surgery he experienced recurring visual disturbances with a sudden onset mimicking his migraine aura. Due to a new onset of atrial fibrillation, he was put on oral anticoagulants. At follow-up after 10 months he still reported episodic and mostly isolated visual auras with a gradual onset.
Keywords
Introduction
It is commonly known that arterial hypertension, atherosclerosis and previous cardiac surgery predispose for aortic dissection. Younger patients with this disease are more likely to have Marfan syndrome, a bicuspid aortic valve or a history of aortic surgery (1). Migraine is associated with an increased risk for cervical artery dissection (CAD) (2). Although the mechanisms behind this relationship are unclear, it is likely that vessel pathologies are linking factors (3).
Previously, type A aortic dissection has only been reported in two patients with a history of migraine (4,5). In both patients severe bifrontal headache without accompanying migrainous features or an aura was either preceded or followed by anterior chest pain.
Our case report of a young man with severe facial pain and a sudden onset of scotomas and hypaesthesia of the upper limbs broadens the spectrum of patients with aortic dissection and atypical presentation.
Case report
In February 2011 a 31-year-old man was admitted to our emergency department due to severe bilateral facial pain confined to the infraorbital and mental region and radiating bilaterally into the medial cervical region. The pain had started abruptly upon rising from the toilet seat after defecation. The pain did not worsen during speaking or chewing and was accompanied by scotomas (i.e. dark spots with spikes around their borders) in the right visual field and bilateral hypaesthesia in the upper limbs, more prominent on the right side. On admission the visual symptoms remitted after 2 hours, but the patient still reported hypaesthesia of the left upper limb, which subsided after a total of 4.5 hours. After initial evaluation by a specialist in internal medicine, including an ECG, routine blood tests and an unremarkable oral surgery consultation, the patient was referred to the neurologist on call at the emergency department. In addition to the symptoms mentioned above, the patient specified that scotomas as well as hypaesthesia had started abruptly and he reported severe nausea and photophobia. The patient reported a history of migraine with aura with a mean attack frequency of three per month since 19 years of age. The migraine attacks consisted of severe pulsating headache over the right temporoparietal region, nausea, photo- and phonophobia. The attacks were always accompanied – and never preceded – by scotomas in the right visual field and numbness of the right half of the patient’s face developing slowly over 5 to 10 minutes. The aura symptoms usually lasted between 20 and 30 minutes. Family history was positive for migraine without aura in the patient’s father. Both grandfathers suffered from cardiac disease. The patient could not report any sudden (unexplained) deaths in his family. There were no other vascular disorders in his family.
Neurological examination revealed painful exits of both infraorbital nerves and hypaesthesia of the left upper limb without any other focal deficits.
Determination of the D-dimer level was ordered and showed an elevated D-dimer level of 0.99 µg/mL. Computed tomography of the brain (CCT) did not reveal ischaemia or intracranial bleeding (Figure 1A). Computed tomography angiography (CTA) of the aorta and supra-aortic vessels showed a type A aortic dissection reaching up to the left common carotid artery (Figure 1B). Interestingly, both carotid arteries were markedly elongated and kinked (Figure 1C). Doppler sonography showed evidence of a moderate-to-severe stenosis of the left subclavian artery caused by the dissection as confirmed by CTA. Subsequently, the patient underwent a root reconstruction, aortic valve replacement and implantation of a supracoronary graft extending to the aortic arch. Histological preparations of the dissected aorta showed mucoid degeneration of the vessel wall and massive loss of elastic fibres. Five days after surgery the patient was examined by one of the authors (S.S.) and did not show any focal neurological deficits. He reported light transient right occipital headaches lasting for several minutes without any accompanying symptoms. Five hours after this examination the patient again developed scotomas in the right visual field in a supine position during duplex sonography. CCT and CTA were performed, but did not detect a new dissection or bleeding. The patient was put on 7500 IE low-molecular heparin administered subcutaneously b.i.d. The scotomas resolved completely within an hour.
(A) Computed tomography (CT) of the patient’s brain. (B) CT with contrast showing the aortic dissection (white arrow). (C) CT angiogram showing the kinking of the cervical vessels (white arrow).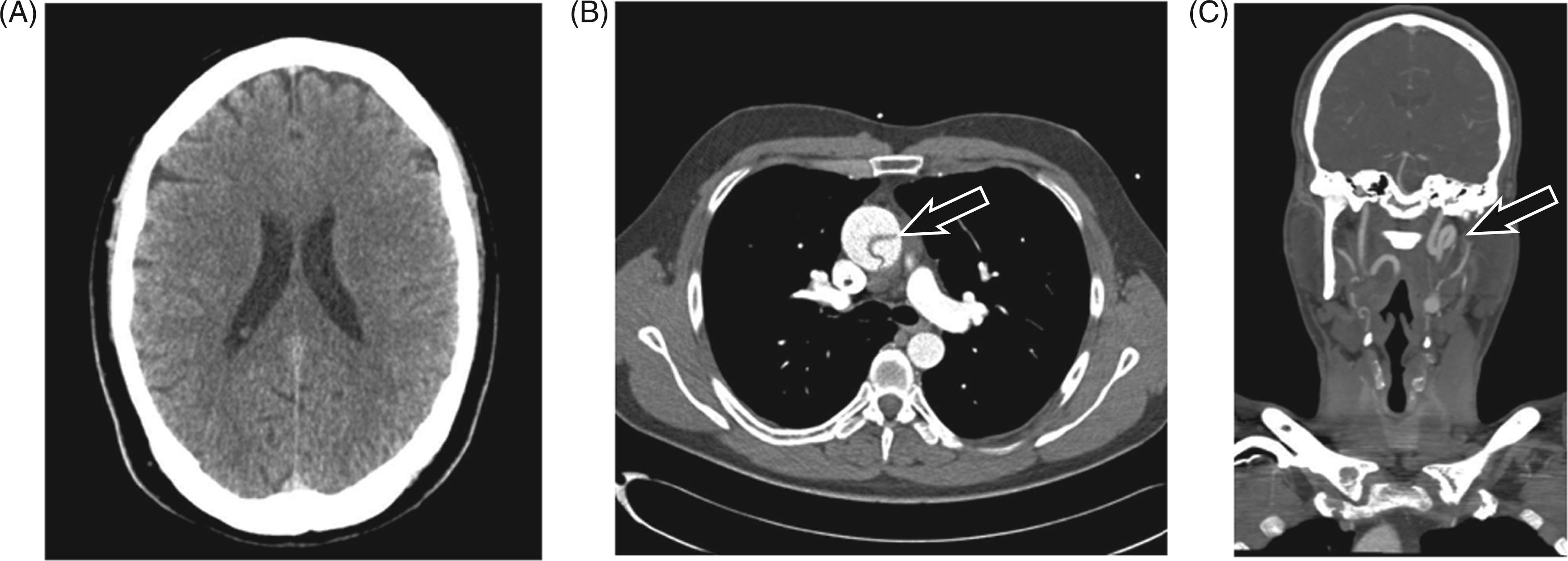
Seventeen days after the first admission the patient was admitted to the hospital once again, for he had experienced a sudden onset of tachycardic atrial fibrillation on a visit to his GP. This was followed by right occipital headache radiating to his right ear and jaw. The headache was accompanied by numbness of the right upper extremity and visual disturbance, both starting abruptly and lasting approximately 30 minutes. The patient reported that the faces of surrounding people appeared as if they had been cut apart vertically and one half remained vertically dislocated. He also said that he could not see the lower half of faces because they were hidden behind a white spot. These visual symptoms were definitely new and had never occurred during one of his migraine attacks. Upon admission the ECG revealed tachycardic atrial fibrillation. The patient also underwent an EEG which remained unremarkable.
Ten months after the acute event the patient was contacted by phone by one of the authors (S.S.) and reported that he had been put on oral anticoagulants and antihypertensive medication. He still experienced his (mostly isolated) visual auras with gradual onset after strenuous activity (e.g. carrying a box, climbing several flights of stairs). These visual disturbances consisted of a dark spot in the middle of his visual field gradually growing larger with spikes around its border and lasted 20 minutes. They were rarely followed by light headaches. He had not experienced any sudden-onset focal neurological symptoms (visual, motor or sensory) after the anticoagulation had been established.
Discussion
Our case stands out for two reasons: First, in the literature, headache as a presenting symptom of type A aortic dissection has only been reported in two patients with a history of migraine (4,5). In both patients the dissection also involved the cervical arteries (4,5). Second, the accompanying focal neurological symptoms resembled the patient’s migraine aura, but differed in two important points. First of all, the visual symptoms and hypaesthesia started abruptly and did not evolve gradually as previously experienced by the patient during his migraine attacks. Second, the sensory deficit (i.e. numbness of the left upper extremity) persisted for more than 60 minutes, thus exceeding the upper time limit for typical migraine aura according to ICHD-II (6).
We may not be able to present a definite pathophysiological mechanism for the development of the focal neurological deficits reported by the patient. Still, two details of the case history deserve a closer look: (i) The sudden onset of the patient’s focal neurological deficits mimicking his migrainous aura points towards cerebral microemboli caused by the acute vascular disease and subsequent platelet activation and/or altered levels of ANP (7). Most recently, Nozari et al. have reported that microemboli trigger cortical spreading depression and thus may lead to the development of a migraine aura (8). It has also been shown that about 20% of auras may start abruptly (9). In our patient, the temporal relationship between the dissection and the occurrence of focal symptoms with a sudden onset strongly suggest that the patient’s ‘sudden-onset aura’ was caused by the vascular pathology. (ii) The patient stopped experiencing sudden-onset visual symptoms and exclusively reported his typical visual auras after anticoagulation had been established. Although the evidence regarding the effect of anticoagulants on microemboli is conflicting (10), our patient may have benefited from this treatment.
Finally, our case raises a question about the pathophysiological relationship between the aortic dissection and migraine with aura. The association between CAD and migraine with aura has been well researched (11). Our case is the third to report a type A aortic dissection in a patient with migraine and the first to report a visual and sensory aura during a type A aortic dissection. To us it seems logical that the well-known altered vascular reactivity in patients with migraine with aura (11) may also predispose these individuals for dissection of larger vessels like the aorta.
In summary, this case report is important in two ways. First, it shows that a change of aura characteristics in migraineurs can alert us to a potentially fatal disease and second, that migraineurs with aura may carry an elevated risk for dissection of large vessels. The latter needs to be confirmed in a larger case-control study.