
Abstract
Persistent visual aura without infarction is rare. Its pathogenic mechanism is unknown, and the response to migraine prophylactic agents varies. A systematic analysis of 29 patients (23 from the literature and six in the present report; 6M/23F, mean age 37.6 years) was carried out in terms of demographics, headache and visual symptom profiles, treatment regimens and outcomes. Patterns of visual disturbances (VDs) were re-assessed with the Visual Aura Rating Scale (VARS, score 0-10). Even though the majority of patients had headache improvement, only eight (27.6±) had complete resolution of persistent VD, without definite relevance to any specific agent. Patients with complete resolution of VD tended to have scotoma (50.0± vs. 0±;
Introduction
Migraine aura is defined as a ‘recurrent disorder manifesting in attacks of reversible focal neurologic symptoms that usually develop gradually over 5–20 min and last for less than 60 min’ according to the second edition of the International Classification of Headache Disorders (ICHD-II) (1). Aura symptoms persisting for > 60 min are unusual and may actually represent complications of migraine. Migrainous infarction (code 1.5.4) is diagnosed if relevant ischaemic lesions are demonstrated on neuroimaging studies, whereas aura symptoms persisting for > 1 week without radiographic evidence of infarction are classified as persistent aura without infarction (code 1.5.3). Another group of patients have very frequent but separate auras over a prolonged period of time, and may be classified as having migraine aura status (code A1.2.7), which is defined as ‘at least 2 auras per day for ≥ 5 consecutive days’ on ICHD-II (1). These migraine complications are rare, and reports were anecdotal.
Persistent visual aura without infarction is rare, and its pathogenic mechanisms are unknown. Visual manifestations in some patients are similar to typical migrainous visual auras (MVAs) (2, 3), whereas others bear little resemblance to typical MVAs. For example, a widespread visual disturbance (VD) consisting of diffuse particles or granules has been described under the terms ‘persistent positive visual phenomena’ (4) or ‘primary persistent visual disturbance’ (5). The response to migraine prophylactic and abortive agents or other medications is variable, and the outcome is unpredictable.
Herein we report on six cases experiencing persistent VD, with special emphasis on their clinical presentations and treatment responses. We also conducted a systematic literature search on PubMed for reports describing patients with persistent VD. VD patterns were re-assessed with the Visual Aura Rating Scale (VARS). This scale was developed by Eriksen et al. to differentiate migraine visual aura and non-aura VD with a high sensitivity and a high specificity (6). By analysing the VD patterns, as well as other demographic data and headache profiles, this may provide some clues in predicting the prognosis of patients with persistent VDs.
Methods
Patient recruitment
Headache patients reporting persistent VDs lasting for ≥ 7 days were recruited from the Headache Clinic of Taipei Veterans General Hospital. None of these patients had a history of substance abuse or major head trauma. All included patients had received a thorough neurological examination, ophthalmological consultation, blood tests for cell counts and chemistries, brain magnetic resonance imaging (MRI) and electroencephalography (EEG) to rule out other relevant pathologies.
Literature review
In order to identify cases with persistent VD, we conducted a search on PubMed (from 1966 to January 2008) for relevant articles with the keywords ‘persistent migraine aura’, ‘persistent visual aura’, ‘persistent positive visual phenomena’ and ‘primary persistent visual disturbance’, limiting results to studies on humans and those reported in English. The reference lists of all identified relevant articles were also searched to minimize the possibility of missing pertinent cases.
The inclusion criteria of articles for this review were as follows: (i) occurrence of persistent VD lasting for > 7 days in patients with headache/migraine or migraine equivalents; (ii) absence of relevant lesions on brain MRI or other relevant pathologies; (iii) availability of descriptions of VD; and (iv) absence of motor symptoms/signs. Articles were excluded if: (i) the patients described their VD as frequent but not persistent, such as patients with migraine aura status (code A1.2.7, see above) (1); and (ii) the patterns of VDs were not provided. All eligible articles were reviewed, and the full texts were evaluated in conformity with the inclusion and exclusion criteria.
Data extraction
Extraction of data from the articles was carried out with a prespecified form, which included patient age, gender, age of migraine/headache onset, age of persistent VD onset, persistent VD pattern, duration of persistent VD, duration of previous headache history before the onset of persistent VD, treatment regimen and outcome. The patterns of persistent VD were re-assessed by two reviewers (Y-F.W. and J-L.F.) independently with the VARS, and the results were labelled present only if the original descriptions contained exact terms or clues for discernment. The VARS includes five items: duration 5–60 min (3 points), develops gradually ≥ 5 min (2 points), scotoma (2 points), zigzag lines (2 points) and unilateral/homonymous (1 point); with the weighted sum as the VARS score (range 0–10 points) (6). Disagreement between the reviewers was settled through discussion. The prognoses were categorized into two groups: ‘with’ or ‘without’ complete (or almost complete) resolution (CR), i.e. sustained freedom from persistent VD. Those with ‘partial resolution’ were not regarded as a separate group because of the fluctuating nature of persistent VD.
Statistical analysis
Statistical analyses were carried out with SPSS version 11.5 (SPSS Inc., Chicago, IL, USA) for Windows. As regards their relations to outcome, categorical variables (patient gender, and presence/absence of each item of the VARS) were assessed with χ2 or Fisher's exact tests, and continuous or ordinal variables (patient age, age of migraine/headache onset, age of persistent VD onset, duration of persistent VD, duration of previous headache history before persistent VD onset and the VARS score) were analysed with the Mann–Whitney
Results
Patients
Six patients in total from the Headache Clinic of Taipei Veterans General Hospital were eligible for analysis, and their demographic data, clinical presentation and treatment regimens are summarized in Table 1. The brief histories of three selected cases are presented below.
Demographic data, clinical presentations and treatment regimens of the patients

VD, visual disturbance.
Case 1
A 26-year-old woman had suffered from migraine since age 15 years, and her mother, all of her four maternal aunts and maternal grandmother were also migraineurs. Migraine occurred about once a week, and each attack would last for hours to days. Some of her headache attacks were preceded by MVAs (bright zigzag flashes) and were accompanied by unilateral facial numbness. She had also had a persistent VD for about 11 years. It was described as countless tiny black and white dots scattered throughout the entire visual field, with the density somewhat in proportion to headache severity, and was likened to ‘TV static’. Her headache transformed into an everyday headache with episodic exacerbations, and she had been overusing ergotamine/caffeine for 7 years prior to her presentation. The frequency and severity of her headache attacks improved with propranolol, amitriptyline and lamotrigine, but the ‘TV static’ visual symptom persisted.
Case 3
A 56-year-old woman had suffered from migraine since the age of 6 or 7 years. It transformed into a daily headache in her 20s, and incapacitating exacerbations occurred several times a month. She reported having seen ‘comets’ persistently since her 30s. These ‘comets’ were mostly sapphire, or sometimes yellowish, in colour, thumbnail-sized and non-scintillating, and appeared as if they were moving forward from behind. She developed episodic MVAs (episodic ‘sapphire lightning’ emerging from the right upper quadrant in the visual field and extending inferiorly and laterally; initially unilateral and later unilateral or bilateral) 15 months prior to presentation, which were usually followed by major attacks within 10 min. The ‘sapphire comets’ persisted, and their numbers sometimes lessened in the presence of ‘sapphire lightning’. Propranolol and topiramate were effective for headache, and with the addition of lamotrigine the frequency and severity of both types of VD and headache improved. She had a headache every 1–2 weeks and still experienced these visual phenomena frequently, yet discretely.
Case 4
A 41-year-old woman presented with migraine since her late 20s. She had been constantly seeing a flashing bright oval spot, about half of a fingerprint in size, staying at the temporal edge of her right eye beginning 6 months prior to presentation. It was visible even with her eyes closed, but did not interfere with her vision. The brightness paralleled headache intensity to a certain extent, and other factors that could exacerbate the VD included poor sleep, fatigue, concentrating on a computer monitor for a prolonged period of time, and menses. Her headache responded to propranolol and flunarizine, but the persistent VD remained until the second month of treatment with lamotrigine and topiramate. The effects were not immediate, and regression of persistent VD was slow and incomplete. Several months after she stopped taking most of her preventive medications, the constant bright spot not only returned but also became bilateral. She began taking lamotrigine and topiramate again, albeit irregularly. There was some improvement, but the VD still occurred very frequently, making it difficult to assess whether the medications worked or not.
Literature search and patient selection
The literature search resulted in eight articles, and review of the reference lists yielded another three. After excluding two articles for discreteness of visual symptoms (which were actually not persistent) (7)and for not providing the clinical features (8), only nine articles (2–5, 9–13) were eligible for further analysis. One of the 24 cases reported in the above-mentioned articles was excluded for insufficient duration of persistent VD (case 2 of Rozen et al.) (3). Including the six patients mentioned above, 29 patients (6 males, 23 females) altogether were analysed (Table 2). The majority of patients (79.3%) were female with mean age 37.6 years (range 9–67). None of the patients had a family history of persistent VD.
Identified cases with persistent visual disturbance eligible for analysis

Spontaneous resolution.
Discrepancy in treatment response.
N, absence; Y, presence; VARS, Visual Aura Rating Scale.
Headache profiles and characteristics of persistent visual disturbance
Thirteen patients (44.8%) were specified as having headache worsening during persistent VD, 11 of whom had daily or very frequent headache. The onset of persistent VD was preceded by a particularly severe or prolonged headache in five patients. Persistent VDs in five patients had an ambiguous temporal relation with headache severity or frequency, and they usually described a simultaneous increment of brightness or density of their persistent VD contents with headache exacerbations.
The mean age of onset of persistent VD was 33.9 years (range 9–67), and the mean duration of persistent VD was 46.4 months (range 11 days to > 20 years). The characteristics of VD are shown in Table 2. Scotoma was present in five patients, zig-zag lines in one, and seven reported their persistent VD as unilateral/homonymous. The VARS score was 5 points for one patient (3.4%), 3 points for two (6.9%), 2 points for one (3.4%), 1 point for four (13.8%), and 0 points for 21 (72.4%). Sixteen patients (55.2%) reported fluctuations in their VD, such as chromatic changes, shifting between discreteness and persistence, etc. Six patients (20.7%) had superimposed episodic MVAs in addition to their baseline persistent VD.
Prognosis
Seventeen patients reported headache improvement after treatment, including 12 of the 13 patients with headache worsening, and none reported deterioration or recalcitrance. Discrepancies in treatment response between headache and persistent VD were reported in 12 patients (41.4%). In 10 of them, headache improved with treatment despite persistence of VD, and in the other two, CR of persistent VD lagged behind headache improvement.
Overall, only eight patients (27.6%) had CR of persistent VD. The response to reportedly effective agents was not consistent: two with CR out of eight for lamotrigine ((9, 11); cases 1, 2, 3, 4 and 6), two out of five for divalproex sodium/valproic acid/sodium valproate ((2, 3, 13); case 5), one out of one for intravenous furosemide (3) and one out of two for nimodipine (10–12). The time between initiation of treatment and CR varied from several hours to 2 months, and generally fell in the range of 2–4 weeks, except for one report, in which the patient who received intravenous furosemide administration responded within several hours (3). CR probably occurred spontaneously for two patients, and their VD persisted for 5 and 7 months, respectively. The persistent VD in the latter patient had also been treated with lamotrigine, but the authors concluded that ‘the benefit of lamotrigine is difficult to demonstrate since visual symptoms were long-lasting and very slow to resolve’ (11).
Outcome predictors for complete resolution of persistent visual disturbance
Patients with CR were more likely to have scotoma (50.0% vs. 0%;
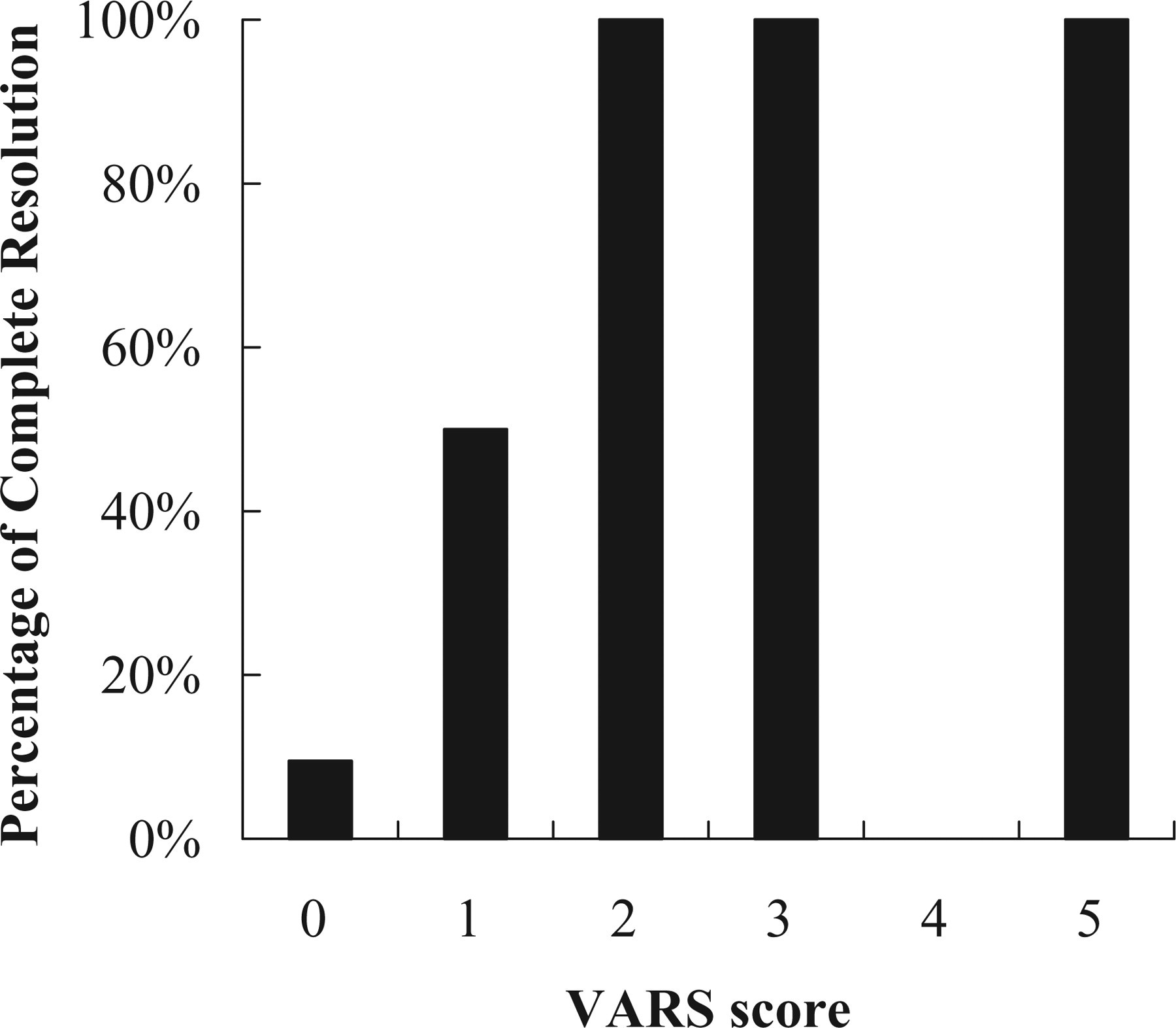
The relationship between Visual Aura Rating Scale (VARS) score and complete resolution of persistent visual disturbance. The VARS score is positively correlated to the percentage of complete resolution (CR). The probability of CR was 9.5% (2/21) for those with a VARS score of 0, 50% (2/4) for 1 point, 100% (1/1) for 2 points, 100% (2/2) for 3 points and 100% (1/1) for 5 points. None of the 29 patients scored 4.
Discussion
Persistent VD is a clinical rarity, and < 40 cases had been reported in the English literature. The clinical presentations of our patients did not differ from those of previous cases. A substantial proportion of patients (44.8%) had headache worsening, although the vast majority reported improvement after treatment. Such was not the case for persistent VD, and only 27.6% of patients had CR. Fluctuation of VD was not uncommon, and it was thus doubted if ‘improvement’ of VD in some patients, i.e. those with partial resolution, was just part of its fluctuation. It also raised the question whether migraine aura status and persistent aura without infarction could be different entities or merely represent different severity of a common disease process.
Based upon our findings, the VARS appeared to be a useful prognosticator for patients with persistent VD, and, more specifically, the configuration of persistent VD was an important factor in predicting CR, whether attributed to a specific treatment regimen or not. Of the three items concerning VD configuration suggested by the VARS, the presence of scotoma and unilateral/homonymous involvement were related to CR. The presence or absence of zigzag lines (fortification) was not a significant predictor for outcome, as only one patient was labelled present. As for the other two variables concerning temporal profiles, the duration definitely exceeded 60 min by definition, and the details of the onset were not documented in most patients. In other words, for persistent VD the likelihood of CR was reflected by its likeness to typical MVAs. The association between shorter durations of illness and better outcomes could be interpreted in two ways. First, early intervention might alter the clinical course and offer the patients a better chance of recovery. Second, for patients with a potential for CR, it would occur early in the course, whereas those without such a potential would have their VD persisting indefinitely. The latter explanation might be more conceivable for three reasons: (i) not everyone receiving early intervention had a good outcome; (ii) CR was not related to any specific regimen; and (iii) none of the patients reported a gain or loss of MVA features either spontaneously or with treatment.
Our study suggested that there was a spectrum of clinical presentations in patients with persistent VD. At one end, patients had typical MVA-like VDs and ended up with a better prognosis. Persistent visual aura seems to be an appropriate term for their visual symptoms. At the other end, patients had persistent VDs with fewer features of typical MVAs, and the outcome was less favourable. ‘Persistent VD’ rather than ‘persistent visual aura’ might be a more neutral term for their visual symptoms. It has been proposed that MVAs may be attributed to cortical spreading depression (CSD) (14), and it has also been hypothesized that persistent VDs could result from sustained reverberating waves of CSD (2). Such a theory might be plausible for patients with persistent visual aura. At the other end of the spectrum, persistent VD lacked a moving quality, and consisted solely of positive phenomena. It is questionable whether persistent VDs in these patients could also result from reverberating waves of CSD or could be just a manifestation of sustained cortical neuronal dysfunction. A unitary hypothesis could be proposed that reverberating CSD waves initiated the event, and in the process of reverberation, CSD waves might shatter and disorganize. ‘Typical’ and ‘atypical’ VDs reflected formed and unformed CSD waves, and the positive phenomena could be a reflection of the preceding hyperactivity of CSD. Some alterations became permanent with time, and thus accounted for the intractability in some patients. Available imaging and EEG studies have, however, failed to provide any solid evidence for or against such a hypothesis. Further efforts are needed to delineate the nature of these phenomena.
There are several limitations to this study. First, the conclusions inferred from observations of the limited number of patients should be treated with caution, and further cases are needed to prove or disprove our findings. Second, assessment of VD patterns of the patients reported in the literature was retrospective, and interpretation rested mainly on the descriptions of previous reports. Although endeavours were made to extract the characteristics of the VD as accurately as possible, some inaccuracies or misinterpretations were possible. Third, the literature search was limited to the English language, and articles published in other languages could have been missed.
In conclusion, we suggest that persistent VD is not a homogeneous condition. The VARS serves as a good clinical tool in risk stratification and outcome prediction, and those patients with higher scores tended to do better, especially those with scores of ≥ 2. For patients with a potential for CR, improvement would occur early in the course, whether attributed to treatment or not.
Acknowledgement
This study was supported in part by a grant from Taipei Veterans General Hospital (V97C1-133).