
Abstract
Background: In the literature there are few data about the prevalence of primary headaches, including migraine, in the Italian general population. The PACE study (PArma CEfalea, or ‘Headache in Parma’) is an observational study aimed at detecting the prevalence and clinical features of primary headaches in the city of Parma’s adult general population.
Materials and methods: A total of 904 subjects representative of Parma’s adult general population were interviewed face-to-face by a physician from the Parma Headache Centre. They were given a specially designed and validated questionnaire for the diagnosis of primary headaches according to the ICHD-II criteria.
Results: Past-year adjusted prevalence of definite migraine, including migraine with and without aura and chronic migraine, was 24.7% (95% CI 21.9 to 27.5); 13% (95% CI 9.7 to 16.4) were men and 32.9% (95% CI 28.8 to 37.0) were women. Past-year prevalence of probable migraine was 5.1% (95% CI 3.6 to 6.5): 5.2% (95% CI 3.0 to 7.4) in men and 5% (95% CI 3.1 to 6.9) in women.
Conclusions: The high prevalence of definite migraine is the major difference between our results and the literature data. Such a difference in results may be due to the use of a different investigational approach compared with the other epidemiological studies. However, an actual higher frequency of migraine in the Italian general population cannot be excluded given the lack of studies on this topic.
Keywords
Introduction
Primary headaches represent a major problem for public health systems because they are widely distributed throughout the world, have a high prevalence, and affect people in all age groups. Many studies have been conducted in various countries, mostly in North America and Western Europe (1), to determine the prevalence of primary headaches.
In Italy, the prevalence and features of primary headaches in the general population have been little studied to date. There are few Italian studies, and they present at least one of the following limitations: they either concern only a segment of the adult general population, notably people in the most advanced age groups (2–4), or apply the diagnostic criteria set by the Ad Hoc Committee on Classification of Headache in 1962 (5,6) or by the International Headache Society (IHS) in 1988 (2,3,7) and therefore preceded publication of the International Classification of Headache Disorders, second edition (ICHD-II) in 2004 (8). We deemed it useful to conduct an observational study, called PACE (PArma CEfalea, or ‘Headache in Parma’), aimed at detecting the prevalence and clinical features of primary headaches in the city of Parma’s adult general population. In this article we report data about the prevalence of migraine, including probable migraine. Additional data will be presented in future articles.
Materials and methods
Gender and age distribution of Parma’s general population, of the initial sample and of responders
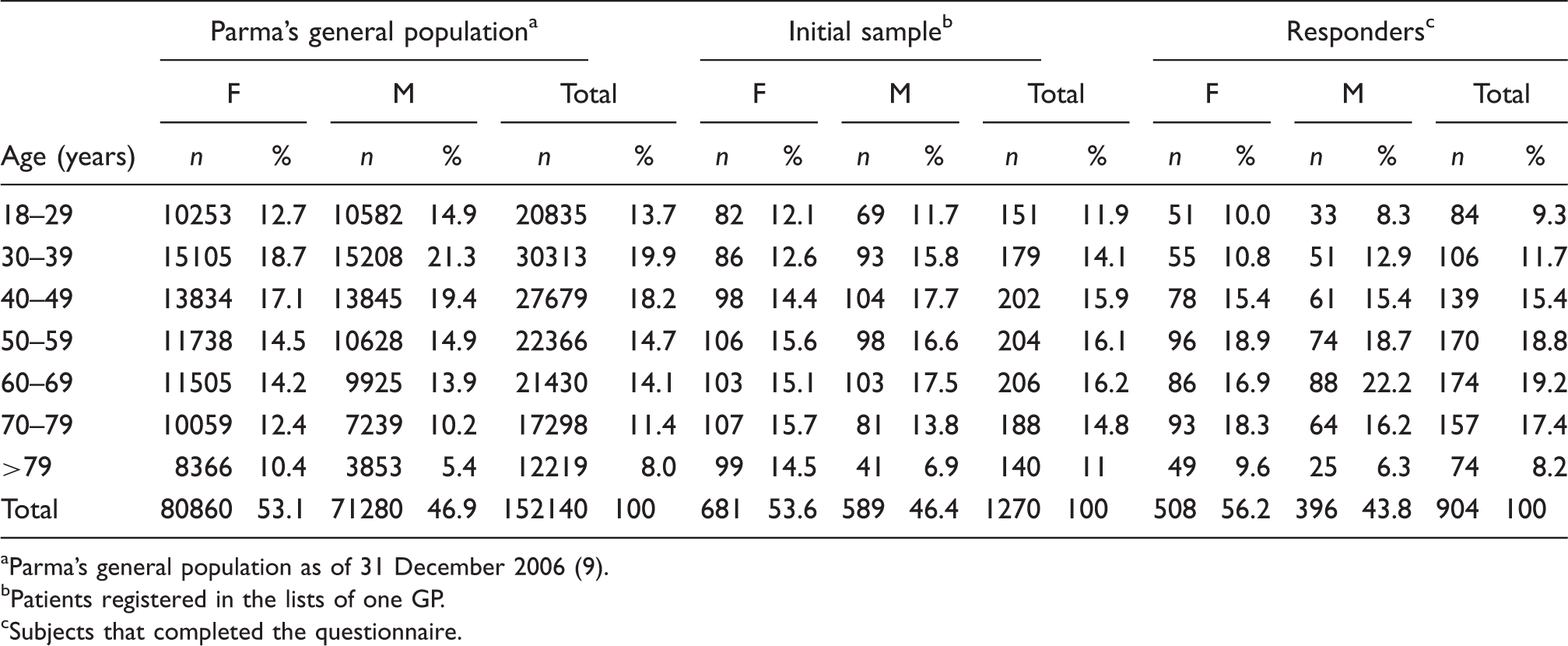
Parma’s general population as of 31 December 2006 (9).
Patients registered in the lists of one GP.
Subjects that completed the questionnaire.
Sampling
Our initial study sample consisted of all residents registered with a GP in downtown Parma. Electronic patient records for each GP practice (as of 1 January 2007) were officially provided by the Parma local healthcare agency of Italy’s National Health Service (NHS).
Our study population can be considered representative of the Italian adult general population, because in Italy primary care must be provided by a physician free of charge to each citizen from birth. The maximum number of patients per GP is 1500, but if the GP so requests, this number can be reduced to less than 1500. Italy’s NHS keeps official records with names and personal data of patients in the practice of each primary care provider. Trust is crucial in the relationship between patients and their family doctors. For primary care providers to best fulfil their role, patients must be free to make their choice with no geographic, administrative or economic constraints. Every citizen may then decide at any time to change their primary care provider by simply addressing a request to the local NHS healthcare agency. The GP’s direct involvement was crucial to our study design. Our choice of the initial study sample was influenced by the number of patients in his practice (n = 1300), as well as by the successful results of past cooperation between our team and the GP (10). The GP did not receive any economic incentive to participate in the study. We removed from the GP’s patient list all subjects aged below 18 years. Our initial study sample consisted of 1270 subjects, 681 women and 589 men.
The study participants were recruited by the GP, who presented them with an overview of the study and arranged for an appointment to interview them at his office or at our Headache Centre. Those who were interested in participating in the study, but said they were unable to reach the appointment venue, were interviewed by phone.
Interview and case definition
The interview was conducted face-to-face by one of the physicians from the Parma Headache Centre and consisted of the administration of a specially designed 13-section questionnaire for the diagnosis of primary headaches in the general population (11), followed by a neurological examination. The questionnaire included a screening question: ‘Have you had a headache in the last year?’ to detect subjects with past-year headache. Through questions in the section about aura and headache, it was possible to diagnose the primary headache types that each subject was suffering from. The diagnosis was based on the ICHD-II criteria. The questionnaire had already proved valid for the diagnosis of primary headaches in the same geographical area (11). The questionnaire versus the clinical interview had shown an excellent concordance rate (K value of 0.96, 95% CI 0.88 to 1.00); if more than one headache type were reported, for the second diagnosis the concordance rate was good (K value 0.61, 95% CI 0.47 to 0.74). Sensitivity for migraine without aura, migraine with aura, chronic migraine, and probable migraine was 100%. Specificity was 100%, except for migraine without aura (93.3%, 95% CI 86 to 100), for typical aura without migraine and probable migraine (97.8%, 95% CI 94 to 100) (11). The subjects considered affected by definite migraine (DM) were those with a headache that fulfilled the ICHD-II criteria for the diagnosis of migraine without aura (ICHD-II code 1.1), migraine with aura (ICHD-II codes 1.2.1, 1.2.2 and 1.2.3), and chronic migraine (ICHD-II code 1.5.1). Probable migraine (PM) cases (ICHD-II codes 1.6.1, 1.6.2 and 1.6.5) were considered both alone and in combination with DM cases (all migraine, AM). Subjects with only one headache attack in the last year were included if they had had the number of attacks required by their respective diagnostic criteria in their lifetime.
Sample size
The estimated prevalence of migraine with aura (1) was assumed as expected prevalence because migraine with aura has the lowest prevalence in the adult general population among the primary headaches under study. The accuracy level was between 0.01 and 0.02.
Statistics
Crude prevalence was the number of cases every 100 inhabitants. Crude prevalence was standardised by sex and age in Parma’s general population aged 18 or over according to the 2006 census (9). We used the chi-square test for frequencies difference and Student’s t-test for means comparison. The 95% CIs of prevalence were calculated assuming that the number of migraineurs followed a binomial distribution; we used the method suggested by Schoenberg (12). Statistical analyses were performed using SPSS version 17.0 for Windows.
Ethics
The study was approved by the University of Parma Ethics Board on 13 February 2007. All subjects gave their informed consent.
Results
Responders and representativeness
The 904 responders (71.2% of the initial study sample) included 508 women (56.2%; mean age 55.9 years, SD 17.2 years, max. 92 years) and 396 men (43.8%; mean age 55.0 years, SD 18.2 years, max. 91 years). In 89 cases (48 men and 41 women) the interview was conducted by phone. No statistically significant differences emerged in gender and age distribution between Parma’s general population, the initial study sample and responders. The only exception was the 18–29 years age group, which showed a difference between responders and the general population (p = 0.046) (Table 1).
Non-responders
A total of 366 subjects (173 women, 47.3%, and 193 men, 52.7%) could not be recruited to the study for a variety of reasons (Figure 1). There were significantly fewer women than men (p = 0.005), especially in the 40–49 (p = 0.002) and 50–59 (p = 0.007) age groups. Mean age was 55.5 years (SD 17.8 years, max. 92 years) for responders and 51.9 years (SD 17.6 years, max. 89 years) for non-responders (p = 0.001).
Study population flow chart. Eligible sample, non-participants (with respective reasons), and final sample.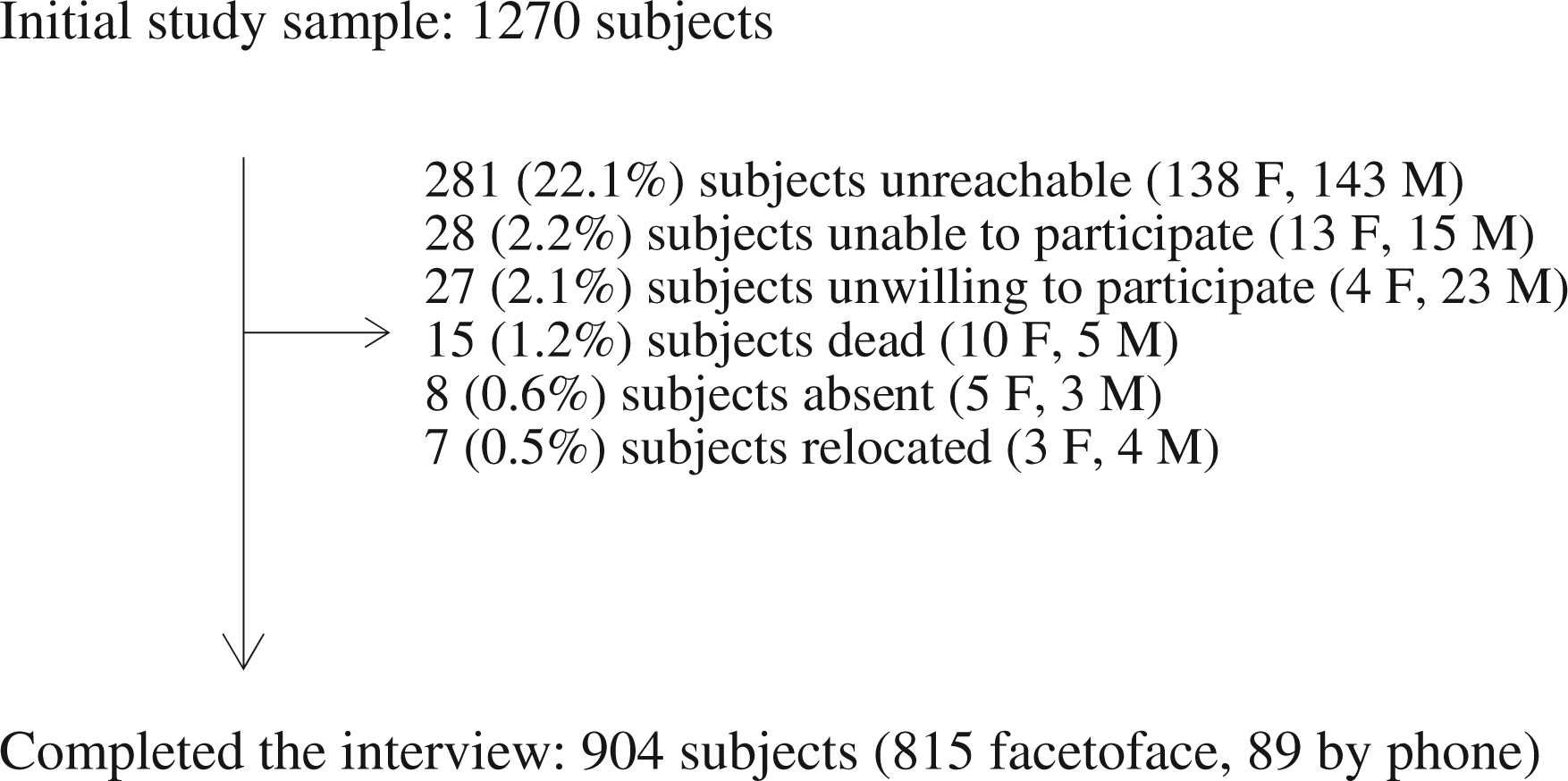
Crude and adjusted prevalence
Crude prevalence by gender and age for DM, PM and AM is reported in Table 2. A total of 196 subjects (21.7%, 95% CI 19.0 to 24.4) had DM, 151 women (29.7%, 95% CI 25.7 to 33.7) and 45 men (11.4%, 95% CI 8.2 to 14.5). The female-to-male (F : M) ratio was 2.6 : 1. Age distribution showed a prevalence peak in the fifth decade, both in women (51.3%, 95% CI 40.2 to 62.4) and in men (21.3%, 95% CI 11.0 to 31.6). Women showed an additional prevalence peak between 18 and 29 years (51%, 95% CI 37.3 to 64.7; Figure 2A).
Past-year crude prevalence of definite migraine (A), probable migraine (B), and all migraine types (C) by age and gender. *1 = 18–29; 2 = 30–39; 3 = 40–49; 4 = 50–59; 5 = 60–69; 6 = 70–79; 7 ≥ 80 years. Past-year crude prevalence of migraine by age and gender All migraine represents the sum of definite migraine and probable migraine.

Thirty-eight subjects (4.2%, 95% CI 2.9 to 5.5) had PM: 23 (4.5%, 95% CI 2.7 to 6.3) were women and 15 were men (3.8%, 95% CI 1.9 to 5.7) (F : M 1.2 : 1). Men had a first prevalence peak between 18 and 29 years (9.1%, 95% CI 0.0 to 18.9) and a second, lower peak in the fifth decade (8.2%, 95% CI 1.3 to 15.1). Women had one peak in the fifth decade (9.0%, 95% CI 2.6 to 15.3; Figure 2B).
Crude prevalence for AM was 25.9% (95% CI 23.0 to 28.7), 34.3% (95% CI 30.1 to 38.4) in women and 15.2% (95% CI 11.6 to 18.7) in men (F : M 2.3 : 1). Both men and women showed a prevalence peak in the fifth decade (29.5%, 95% CI 18.1 to 41.0, and 60.3%, 95% CI 49.4 to 71.1, respectively). Women also showed a first peak between 18 and 29 years (56.9%, 95% CI 43.3 to 70.5; Figure 2C).
Past-year prevalence of definite migraine subtypes by gender
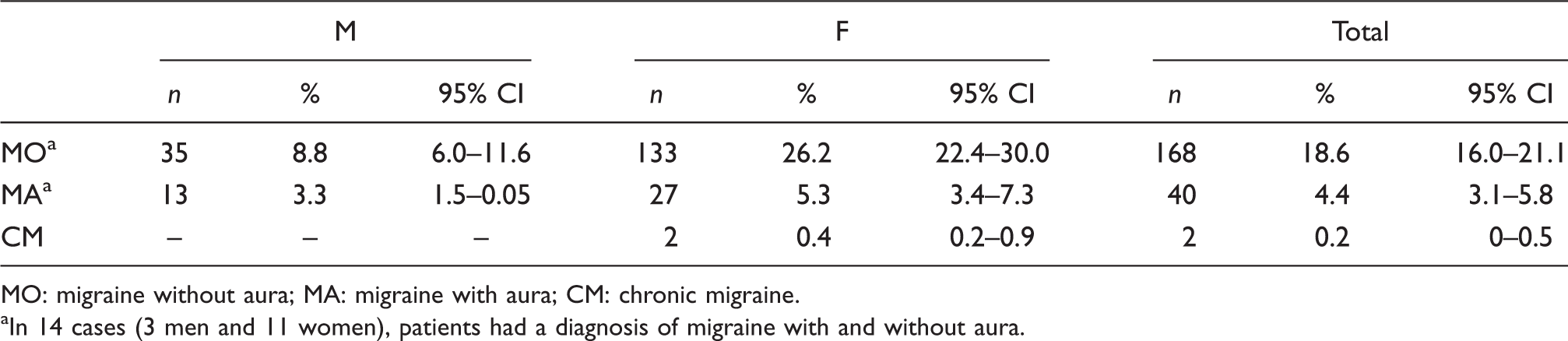
MO: migraine without aura; MA: migraine with aura; CM: chronic migraine.
In 14 cases (3 men and 11 women), patients had a diagnosis of migraine with and without aura.
Discussion
In our study the past-year DM prevalence (29.7% in women and 11.4% in men) is at the upper limits of the ranges reported in the literature (1).
The DM gender ratio varies between 1.7 (13) and 3.3 (14) in the European Union, and between 2.2 (15) and 3.1 (16) in North America. Our data (F : M 2.6) agree with those reported for Western countries.
The DM prevalence pick in Western countries is between 30 and 49 years, for both men and women (1). Our study showed a comparable pattern: we found the highest peak between 40 and 49 years in both genders. The first peak between 18 and 29 years in our female study sample confirmed similar observations by the authors of the 2001 Swedish study (13) and of the 2003 British study (17). The decrease in prevalence after age 50 in both genders was also observed in other studies published in the literature (1).
In our study population, PM past-year prevalence was 4.2% (3.8% in men and 4.5% in women) with a gender ratio of 1.2. In the literature there are few data about PM. Katsarava et al. reported in the Republic of Georgia a 9.2% PM prevalence (18), while a recent Spanish study reported a 4.2% estimate (19), as well as several studies conducted in the USA (20–22). Additional data published in 2002 from the American Migraine Study II (23) indicate a PM prevalence of 2.6% (20), while the American Migraine Prevalence and Prevention Study reported a 4.5% prevalence (3.9% in men and 5.1% in women) (22). The US study, conducted on people involved in a health plan who had sought medical treatment at least once for any reason in the preceding 24 months, shows a prevalence of 14.5% (19.6% in women and 13.1% in men) (21). Lifetime prevalence of the migrainous disorder coded to 1.7 in the IHS classification is 9.1% in France (24) and 16.2% in Germany (25).
Chronic migraine (CM) prevalence in our study was 0.2% (95% CI 0.0 to 0.5). A recent systematic review reports a 0–5.1% global prevalence of CM (26). Of all the studies considered, only three European studies defined CM as migraine that occurred on ≥15 days per month (or an equivalent yearly rate) according to IHS criteria (7,26). Prevalence estimates using this stringent criterion were relatively low and ranged from 0 to 0.7% (25,27,28).
The high prevalence for DM is the major difference between our results and the literature data. Some considerations can be offered. The methodological approaches to epidemiological studies may determine a difference of up to 30% in results (29,30). As regard the diagnostic criteria, only few authors applied the ICHD-II (19,21,31–34) as we did in our study, but we can reasonably exclude that the use of the ICHD-I in many of previous surveys may have significantly biased results because criteria for the migraine types under study are basically no different.
The published migraine prevalence studies appear also to differ with respect to the age groups considered. Some studies define a minimum inclusion age of 12 (16,23,33), 13 (34), 15 (35) and 16 years (17,18,32), i.e. the prevalence estimate is also based on data from adolescents. Similarly, other studies don’t consider elderly patients (14,17,36–38), such as the 2004 US study, which was conducted on people aged up to 55 years (21). Finally, there are countless other studies that estimate prevalence only in limited age groups (1). Our study population was an adult population aged 18 years or over, with no upper age limits and advanced mean age (around 55 years). However, if we consider that migraine prevalence tends to decrease progressively in old age, not even the age factor can explain our high DM prevalence.
Another, and probably more important, methodological difference concerns the procedures followed for the interview. A primary headache diagnosis is based on officially recognised and well-established diagnostic criteria. From the practical point of view, it must rely on an in-depth discussion with the patient to compensate for the absence of any laboratory or instrumental markers. In epidemiological studies, the interviewer and the interview mode that ideally reproduce the best investigational ‘clinical setting’ are represented by a physician experienced in headache disorders performing a face-to-face interview and a neurological examination as we did. This is undoubtedly a procedure that carries the disadvantage of being very time-consuming and requiring highly specialised personnel. As a result, it is hardly applicable in very large populations.
The Danish study (36) was performed by a face-to-face interview and the authors reported a lower DM prevalence (10%) than ours. However, only one study doesn’t allow a conclusive evaluation. Other interview modes, less accurate but more suitable to investigating large patient samples, are the structured self-administered questionnaire (14,16,23,33,34,39,40), the personal interview conducted by trained non-medical personnel (15,31) and, especially in Anglo-Saxon countries, computer-assisted telephone interviewing (CATI) (17,19,21,37,38).
We know that often interviewees will not answer in such an unequivocal way as the diagnostic criteria of international classifications would require them to. Instead, they tend to use adverbs or circumlocutions that render their answers ambiguous. The interviewers may differ widely, depending on whether he/she is a headache specialist or a lay interviewer: the former will try to clarify the answer by asking more questions based on his/her clinical skills; by contrast the latter, unable to use clinical reasoning, will be forced to translate the interviewee’s vague answer into a kind of answer that is accurate but obviously arbitrary. Eventually, the medical expert and the lay interviewer may interpret the interviewee’s answer in an entirely opposite way and their diagnoses will be completely different.
Having the interview conducted by physicians with proven experience in headache disorders enabled us first to perform a ‘generic’ screening of headache patients (‘Have you had a headache in the last year?’) and then to establish a possible diagnosis of migraine thanks to the accurate evaluation of all headache clinical features detected by the questionnaire.
This procedure also avoided a screening method based on such headache features as severity, frequency, the use of anti-migraine drugs, etc. A criterion often used to screen migraine is headache severity. While that criterion is helpful when investigators evaluate the social burden of migraine, it can easily lead to prevalence underestimation. It is in fact possible to make a migraine diagnosis that entirely fulfils the ICHD-II criteria even when the headache occurs with a less than ‘strong’ severity. Different epidemiological studies in the USA and Europe have used headache severity as a screening criterion for migraine (15,16,21,23,31,37,38). The detected cases were then investigated further in order to establish a diagnosis and migraine prevalence was estimated at 8.5% (15) to 14.7% (21).
A further explanation for the high DM prevalence found in our study might be that we also identified as DM cases those subjects who had had only one attack in the year preceding the study, and we judged that the A criterion (‘at least five attacks fulfilling criteria B–D’) set by the ICHD-II for migraine without aura diagnosis had been fulfilled even though four of the five attacks had occurred before the study year. Instead, if we had considered the A criterion fulfilled only in those subjects with at least five attacks in the year preceding the study, clearly past-year prevalence would have been lower than we reported. Unfortunately, the other epidemiological studies in the literature do not provide any clear indications in this respect and so we cannot determine how and to what extent our choice may have affected disparities between data. We expect to find some explanation through a future distribution analysis of our DM patients based on frequency of attacks and number of days of headache.
These two parameters are of great importance not only for systematic description and classification purposes (41), but also for epidemiological studies, as was indirectly confirmed by Katsarava et al. (42), which reported data from the population-based survey of the German Headache Consortium. This survey was conducted on 9350 subjects aged 18–65 years through a validated questionnaire. The prevalence of high-frequency episodic migraine (9–14 days of migraine per month) – which was present in 228 subjects – and of low-frequency episodic migraine (≤8 days of migraine per month) – which occurred in as many as 2356 subjects, was 27.6%, higher than the one found in our study.
In conclusion, our study results indicate a migraine prevalence at the upper limits of the data ranges currently available for the European Union and North America. It is likely that different methodological approaches led to data disparities between the different studies published in the literature. However, an actual higher frequency of migraine in the Italian general population cannot be excluded.
Footnotes
Funding
This study received financial support from Merck Sharp & Dohme Italia [grant number DR n 69 del 28.01.2009].
Conflict of interest
None declared.