
Abstract
A randomly selected sample of 1668 individuals (782 women and 886 men) aged 18–74 years was interviewed by telephone using a standardized questionnaire including the International Headache Society (IHS) criteria for migraine. The survey was performed by SIFO, the national public opinion poll agency. The results obtained demonstrate that 21% of the Swedish population had suffered from severe headaches during the past year. A majority of these headache sufferers (61%) fulfilled the IHS-criteria for migraine. The 1-year prevalence of migraine in Sweden was found to be 13.2 ± 1.9% (16.7% among women and 9.5% among men). The prevalence of migraine in this Swedish population did not differ between the northern, middle and southern part of Sweden, or between urban and rural areas or different income groups. Only about half (49%) of the migraineurs had been diagnosed by a physician. Among the individuals who fulfilled the IHS criteria for migraine the mean attack-frequency was 1.3 per month and the mean attack-duration was 19 h. If the duration of the attack was disregarded as a strict criterion for migraine (attacks < 4 h and > 72 h were included), the prevalence increased to 17.0 ± 1.9% without affecting the sex distribution. With this amendment, 92% of those who considered their headaches to be migraine or migraine-like in fact fulfilled the alternative criteria for migraine. However, only 76% of those who believed that they had migraine or migraine-like headaches fulfilled the strict IHS criteria for migraine. An extension of the time window from 4 to 72 h may be reasonable both from a pragmatic and from a rational clinical point of view.
Background
Migraine is a common disorder, which to a great extent disables the individual sufferer. Information about the prevalence and impact of this condition in the population is essential from both clinical and public health perspectives (1–4). A considerable number of studies have dealt with the issue of migraine prevalence, which has been reviewed recently (2, 4). The results vary considerably and the interpretation of the published reports is complicated, mainly due to differences in case definitions and in the age and sex distribution of study populations. Most studies have been performed in selected groups of patients without application of the explicit diagnostic criteria for migraine proposed by the International Headache Society (IHS) in 1988 (5). During the last decade significant methodological advances have been made, resulting in more congruent figures. However, there is still a general need for additional descriptive and analytical population-based epidmiological studies (2). In Sweden three studies of migraine prevalence were performed before the advent of the IHS criteria, one in a large group of women visiting a birth control clinic (6) and two in selected groups of children and adolescents (7, 8). The aim of our investigation was to present the first available data on the prevalence and characteristics of migraine in the general Swedish community.
Methods
Sampling
From March to May 1997 sampling was performed by SIFO AB, a national public opinion poll agency, by a method of randomised clustering in two major steps.
The basis for selection was the current 28 volumes of the national telephone catalogue. These were divided into the 70 different labour market regions in Sweden specified by the public statistics. The data-base of ‘Folk-och Bostadsräkningsdata’ provided further information on the number of households in each region. This was the foundation for deciding how many individuals were included from each catalogue. Households without a telephone were not included in the sample. A computer program randomly chose the page, column and line in the catalogues. Numbers belonging to a company or a public authority were replaced by the closest following number. For every accepted number, nine additional numbers are generated by adding 1–9 to the last digit. Ex-directory phone numbers were thus picked up by this procedure. The result was an adequate amount of bundles of 10 consecutive numbers from the same area code. The interviewer started with the top number in a bundle. If there was no answer, if it led to a company or a public authority, or if there was an unobtainable tone, the next number in the bundle was chosen. Numbers without reply were left in the bundle. This was repeated until an answer was received from a household. If there was no answer in a bundle, a spare bundle was chosen with the same area code.
When the interviewer came into contact with a household, he or she initially collected information on the number of Swedish-speaking household members aged 18–74. These were written down on consecutive lines in order of descending age. On every line, there was a random number deciding who should be interviewed.
The integrity of the selected persons was respected. All had a right to decline participation. If the chosen person was not at home, he or she was replaced by the youngest male in the first place, the youngest female in the second place or another member of the household in the last place. The reason for this was that men and young individuals are more difficult to reach by phone.
Survey
A large group of lay interviewers above the age of 18, who were regularly engaged by SIFO and had all undergone a special training-course, administered a questionnaire by telephone. By way of introduction, the objective of the study and estimated consumption of time was presented to the individual. Verbal informed consent was obtained. The person was then asked a series of questions by means of a structured interview. The interviewers read their questions on a display. All questions had to be answered with yes or no, and the answers were fed directly into a computer. Successive questions were only visualized if motivated by earlier answers. On average, 7 min was required to complete each interview. Spot tests were performed, in which around 10% of the subjects were contacted by telephone again later on to check on the household data, the performance of the interviewer and if the questionnaire had been applied correctly.
At the end of the telephone interview, those who had reported migraine or migraine-like headache were asked about participation in an enlarged postal study. Outside the epidemiological survey, further contacts were made by telephone in order to gather more individuals with migraine or migraine-like headache for the same reason.
Measures
The initial question related to headache in the telephone survey was whether or not people ever had a headache. They were then asked if they had experienced a severe headache that could be considered very troublesome during the last year, whether or not they thought they had migraine or migraine-like headache, and if they had received a diagnosis of migraine from a physician.
Detailed questions were then asked about their most severe type of headache (if present) during the last year. Prodromes were sought by asking if they could predict if an attack is on the way. They were asked outright about aura-symptoms (for example flashes of light lasting 5 to 60 min). No information was collected about the specific nature of aura disturbances. Specific symptoms associated with headaches including unilaterality, throbbing headache aggravated by physical exertion, sensitivity to light, sensitivity to sound and nausea and/or vomiting were registered.
From the postal survey, which was comprehensive, results are only reported here for the following questions: For how long have you had migraine? How often do you have migraine? What is the average duration of your attacks, untreated or unsuccessfully treated? Do you recover completely from migraine symptoms between the attacks? Do you have a close relative with migraine?
Case definition
Subjects were diagnosed in accordance with the most severe type of headache experienced in the last year. The diagnosis in each case was reached based on a questionnaire-based algorithm, constructed from the IHS criteria of 1988 (5). Migraine was diagnosed only in those meeting the IHS criteria for migraine with aura and/or migraine without aura. Migraine was thus diagnosed if the person had recurring headaches lasting 4–72 h with at least two of the following characteristics: unilateral pain, pulsating quality, moderate or severe intensity, aggravation by routine physical activity, and at least one of the following: nausea and/or vomiting, phono- and photophobia.
Analysis
A so-called post-stratification was performed before production of the final results. This procedure counterbalances fluctuations in the sample and reduces the risk of distortion in the results considering that all selected individuals did not agree to be interviewed. All interviewed participants in the sample are divided into cells according to age and sex. Each cell is compared with its counterpart in an ideal selection. Discrepancies are then counter-balanced. In the report consisting of computer-written tables, the number of interviews both before and after weighting is shown. Percentages are always balanced.
All data were processed using the computerized, flexible crossorting-program Diana® at SIFO in Stockholm,
Further analysis was based on the distributions of the migraineurs according to the IHS criteria arranged according to sex, urban/rural areas and the northern/middle/southern thirds of the country.
We studied how many regarded themselves as having migraine but who did not strictly fulfil the diagnostic IHS criteria for migraine and the opposite situation. Finally, we examined the impact on migraine prevalence of the strict time-span for attacks that is postulated.
A special formula has been used when calculating the margins of unreliability, which are larger close to the middle of the percentage scale. For 1600 interviews (with a response rate of 15–20% of the initially selected population), SIFO states the deviation from a studied population of 7 million to be ± 1.8–1.9% units with 95% confidence.
Results
Response rate and representativeness of the samples
Since the sampling was performed by the method of substitution (the interviewer took a new number if there was no reply, in the case of technical obstacles or if a person not appropriate for inclusion answered), the total number of telephone calls was not documented. The number of other non-contacts, such as persons not registered in the population data, is unknown. The exclusion of households without a telephone is not considered a bias worthy of note, since the coverage of telephones is very high in Sweden (68% of the inhabitants or 1.36 per household). Individuals with mental handicap or deafness were excluded. Drop-out, defined as individuals contacted and asked about inclusion but not interviewed due to refusal, unavailability or lack of interest, was 14.1%.
An absolute number of 1668 persons (782 women and 886 men) in the age range 18–74 years old were included and interviewed by telephone. The corresponding weighted figure after post-stratification (see Analysis above) is 1661 persons. This final sample was representative of the 1997 population (approximately 7 million persons in the studied ages) of Sweden with regard to sex and age.
Before the postal survey approximately 5400 telephone calls were made in order to reach 754 individuals reporting themselves as having migraine or migraine-like headache. Out of these, 709 agreed to participate and received a comprehensive postal questionnaire. After 70% (495 persons) had answered the collection of returned forms was stopped for reasons of time. Those who now had answered ‘no’ or ‘uncertain’ to the question if they had migraine or migraine-like headache were excluded. The analysis of the extensive postal survey was based on the remaining 444 persons. However, in the results presented here, only those 97% (n = 423) who after analysis of symptoms proved to fulfil the IHS migraine criteria (apart from the strict duration of 4–72 h, which was deliberately disregarded, see Discussion) are taken into account.
Prevalence of recurrent headaches and migraine
In the telephone survey 1036 out of 1661 (62%) respondents, 441 (43%) men and 595 (57%) women reported recurrent headaches in the past year. Out of these, 356 individuals (21% of the total 1661), 141 (40%) men and 215 (60%) women, graded the intensity of the recurrent headaches in the past year as severe.
A total of 218 persons in the telephone survey considered themselves to have migraine or migraine-like headaches, representing 61% of those 356 with severe headaches. Seventy-six per cent of these individuals were confirmed as fulfilling the diagnosis of migraine according to the IHS criteria. Among those with severe headaches who in fact fulfilled the strict IHS criteria for migraine, as many as 24% (52/219, weighted) did not consider themselves to have migraine or migraine-like headache. Furthermore, only about half (49%) of the individuals had received a physician's diagnosis of migraine. Ninety-four per cent of those who previously had been diagnosed as migraineurs were found to meet the IHS criteria for migraine by the method used in this study.
A crude total of 212 out of 1668 respondents met case definitions of migraine according to the strict criteria of the IHS. This corresponds to 219 out of 1661 persons after post-stratification, resulting in a 1-year prevalence of 13.2 ± 1.9%, 16.7 ± 1.9% among women and 9.5 ± 1.9% among men. The female to male ratio was 1.8:1. (Fig. 1a). The prevalence was similar for the northern, middle and southern part of Sweden, and for people living in urban vs. rural areas, as well as for those in different income groups.

(a) Total and gender specific 1-year prevalence of migraine according to IHS criteria in an adult (18–74 years) epidemiological Swedish sample. Data are presented in age classes of 10 years with the exception (6 years) for the youngest group (18–24 years). (b) Total and gender specific 1-year prevalence of migraine according to IHS criteria but disregarding attack duration (attacks < 4 h and > 72 h were included) in an adult (18–74 years) epidemiological Swedish sample. □ Migraine prevalence; ▪ Female; (dotted square) Male.
However, if attack duration was excluded as a pivotal criteria for migraine diagnosis, the prevalence of migraine increased significantly from 13.2% to 17.0% (Fig. 1b).
Clinical characteristics of the migraine attacks
The frequencies of specific symptoms appearing in connection with the headache attacks were analysed in the subgroup of the telephone survey fulfilling the IHS criteria for migraine (n = 212, absolute). Only the persons who had migraine attacks with severe headache and a duration of 4–72 h were analysed concerning these characteristics.
Ability to predict attacks (interpreted as prodromes) was reported by 61%. Aura was experienced by 26%. The pain was unilateral in 82% of the group. It was throbbing and aggravated by physical effort in 80%. Nausea and/or vomiting were associated with attacks of migraine in 68%. Photo- or phonophobia was usually present (95%) (Fig. 2).
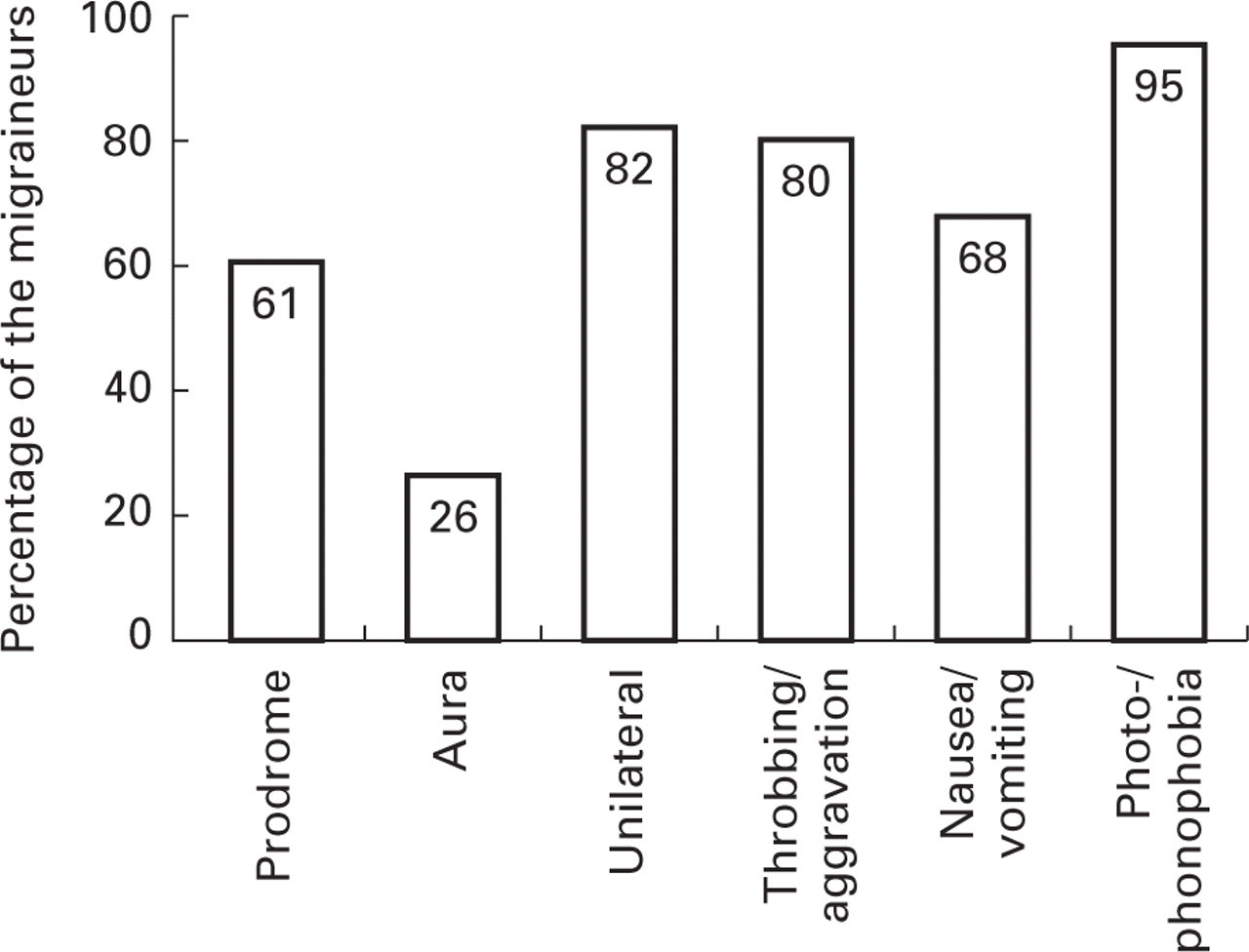
Clinical characteristics of migraine attacks with duration of 4–72 h in a Swedish epidemiological sample (n = 212).
Additional information from the postal survey
When analysing the attack duration in the postal survey, it was found that 15.8% of the attacks had a duration shorter than 4 h and 6.4% longer than 72 h. Thus, an alternative prevalence figure was calculated without taking the duration of the migraine attack into account but considering the other customary parameters of the IHS criteria. The prevalence then increased by about 4% to 17.0 ± 1.9% without affecting the sex distribution or that of any of the other parameters addressed.
A majority (52%) reported having suffered from migraine for more than 10 years. The mean attack frequency according to the strict IHS criteria for migraine was 1.3 per month. The frequency was equal for the loose criteria. Most individuals (60%) had an attack frequency of at least once per month. Twenty-seven per cent of the migraine sufferers had 68% of all attacks (Fig. 3).

Distribution of the total number of migraine attacks and attack frequency per year in a Swedish epidemiological sample (n = 423). The results are presented as percentage of the total number of attacks per given mean attack frequency. Mean attack frequency in the total sample is 1.3 attacks per month. The calculated percentages of migraineurs represented in each of the frequency groups are given within brackets. Twenty-seven (9% + 18%) per cent of the migraine sufferers had 68% of all attacks (32% + 36%).
The mean attack duration was 19 h. Almost half of the group (47%) had an attack duration of 4–12 h (Fig. 4).

Distribution of migraine attack duration in a Swedish epidemiological sample (n = 423). Mean attack duration in the sample is 19.0 h.
A group of individuals (9%) did not consider themselves to recover completely from migraine symptoms between the attacks. Of the others, an equal number answered ‘Yes’ and ‘Yes, more or less’ to this question.
Out of the individuals with migraine, 64% reported also having a close relative with migraine.
Discussion
Most epidemiological studies have been based on material from general or specialist clinics, leading to a skewed selection since only about 50% of the individuals with migraine seek medical care at all. In clinic-based studies, factors leading to consultation can be falsely interpreted as an attribute of the disease (1). The studied sample in an epidemiological study must be representative of the source population, which is often the population of a country in headache studies. One way is to perform a randomized selection from the general population (9), as in this case.
A headache diagnosis should preferably be based on anamnestic data, physical examination and in some cases laboratory investigation to exclude symptomatic headache. Ideally, this is performed by an experienced clinician in a face-to-face interview and/or by using a semistructured questionnaire. Unfortunately, this is seldom possible in larger epidemiological studies for reasons of geography and cost. It has been demonstrated, however, that the method of applying structured telephone interviews based on the IHS criteria is a sensitive and valid way of diagnosing migraine. The technique has been used in several other recent and well-designed epidemiological studies and is in our opinion of very high scientific value (2). The method used in this study is partly validated by the fact that 94% of those who previously had been diagnosed as migraineurs where found to meet the IHS criteria for migraine. A review of the literature reveals that every second (six out of 12) current epidemiological study in the Western world has used lay interviewers and every third (four out of 12) has been telephone based (2). Accordingly, a telephone interview was a good compromise, since the studied sample by definition was spread all over the country, and for obvious reasons a face-to-face diagnostic clinical interview was never an option. Further, we have not been able to exclude symptomatic headaches with certainty. It is comforting, however, that secondary headaches are very rare in the general population (9).
Since the potential participant was initially informed about the relatively short time required for the interview, the drop-out rate was reduced in comparison with a more time-consuming study. The number who declined is dependent upon how much effort is put into getting a desired interview by the institute. With this vital factor of time in mind, we chose beforehand to combine two key symptoms into one question, ‘throbbing and aggravated by physical effort’, as a trade-off.
Our results have been balanced by post-stratification to compensate for difficulties in reaching certain groups. When analysing the material from a spot test survey like this one, it is nevertheless essential to keep in mind that the percentages are rough estimates. One should also be aware that the results are based on how the respondents interpret the questions and that the questions have been posed by lay interviewers. Counter-questions have not been answered. Minor differences in the formulation of the questions can affect the result markedly (9, 10). After meta-analysing a large number of studies on migraine prevalence, it has been concluded that the major variations are a result of differences in sex and age in the selected group (1, 4, 11). Another complicating factor is the variation in the clinical manifestations of the individual over time (1). It is therefore very important to define the studied interval of time (2, 9). It is generally considered that the 1-year prevalence – defined as individuals who have ever had two attacks of migraine with aura or five attacks of migraine without aura and who have experienced at least one attack in the last year – is an important parameter (11). A theoretical weakness of our method of diagnosis is that the persons have not been asked directly if they have had at least two attacks of migraine with aura or five attacks of migraine without aura. However, the data on attack frequency in the more detailed postal survey support the conclusion that this was so in the studied persons.
We find it important for reasons of completeness to include some results from the more comprehensive postal study of 423 persons with migraine in this presentation. The main part of the data will be presented separately. Persons were recruited on the basis of their own opinion on diagnosis because the lay interviewer's computer during the process of sampling did not indicate whether or not the subject actually fulfilled the IHS migraine criteria. Accordingly, 3% of the collected forms have afterwards been excluded from the presentation, since they did not show migraine according to the IHS criteria.
The results obtained demonstrate that approximately 21% of the Swedish population had suffered from severe headache, which they perceived as very disabling during the past year. The vast majority of these headache sufferers, 61% (219/356, weighted), fulfilled the strict IHS criteria for migraine. When we disregarded the duration of attacks, 79% (283/356, weighted) were migraineurs. Rasmussen and coworkers performed the first study ever on the prevalence of headache in a large material in Copenhagen based on the IHS criteria (1, 12). The 1-year prevalence of migraine was 6% in men and 15% in women (12). On average, approximately 10% of the population were active migraineurs in that study (11). In 1999 a total of four European and four American studies based on the IHS criteria showed rather congruent results (2, 13). The 1-year prevalence of migraine in these was 10–12% (6% for men and 15–18% for women) (2, 13). In the light of this, our results are coherent with the world around. In accordance with other European investigators, we were not able to find a correlation between migraine prevalence and social group, which is contradictory to what has been reported from similar studies performed in the USA (1, 2).
Interestingly, if the attack duration was not allowed to influence the diagnosis of migraine, the prevalence increased significantly from 13.2% to 17.0%, based on the telephone interviews. The same phenomenon was noted in the postal survey. A considerable number of individuals (about 16%) reported attacks shorter than 4 h. One reason for this finding may be the treatment used. In addition, about 6% reported their migraine attacks to be longer than 72 h. It could therefore be warranted from a pragmatic point of view in certain cases to disregard the exact duration of migraine attacks when making the diagnosis in clinical practice. It has been noted before that the duration of pain is of little use in the discrimination of migraine from tension-type headache (14).
A two- to threefold risk of migraine has been reported among first-degree relatives (15). In Rasmussen's study, 56% of migraineurs report migraine in first-degree relatives (parents, siblings, children) (12), which is in the same range as found in the present study (64%). According to a standard headache inventory used at Gothenburg Migraine Clinic, a positive family history of migraine-type headaches is reported by 75% out of 3000 IHS-migraineurs. In 59%, 22% and 19% of the cases, the family history of migraine was on the maternal, paternal and siblings/children, respectively (C. Dahlöf, unpublished observations). In contrast to the IHS migraineurs, only 20% out of 200 patients with episodic tension-type headaches according to the IHS criteria report a positive family history of migraine-type headaches among their first-degree relatives. A similar percentage figure (about 20%) is obtained when spouses are asked about migraine heredity. Similar to the findings in this study, only about half of the migraineurs in the study of Rasmussen had consulted a physician as a result of headaches (12). Several other reports have confirmed the same low frequency of medical consultation (2).
Migraine is not something one assumes one has without good reason. A majority (76%) of those who considered themselves as having migraine or migraine-like headache indeed fulfilled the IHS criteria for migraine. If the duration of attacks is disregarded, this figure is even higher, 92%. If we consider the prevalence of migraine to be 13.2% in an adult population of 6.37 million (year 1997; age range 18–74 years), it can be estimated that in Sweden some 840000 adult persons (female to male ratio 1.8:1) suffer from migraine according to the strict IHS criteria. Of great interest is that an estimated number of 200000 Swedes are unaware of the fact that their headaches are migraine. With a mean attack-frequency of 1.3 per month, the number of attacks per year in Swedish adults is approximately 13 million.
Headaches are a major public health problem in all countries and drain the productivity, the medical services, the public welfare, the individual and his or her family. The financial impact (mainly the indirect costs) and the psychosocial and human suffering are enormous (11, 13, 16–18). We hope the results presented here will be a useful epidemiological basis for measures aimed at improving the situation for migraineurs in Sweden. However, further studies concerning socio-economic factors in connection with migraine are needed.
Footnotes
Acknowledgements
Financial support was received from Zeneca.