
Abstract
We set out to examine selected clinical characteristics of migraine patients referred to neurologists specializing in headache in Canada, and to document their pharmacological therapy both before and after consultation with the neurologist. Demographic, clinical and pharmacotherapy data were collected at the time of consultation for 606 patients referred to five headache clinics and who were given a migraine diagnosis by the neurologist. Data were analysed as part of the Canadian Headache Outpatient Registry and Database (CHORD) Project. The mean age of the migraine patients was 39.7 years; and 82.5% were female. The majority of patients suffered severe impact from their headaches. Prior to consultation, 48.7% were taking a triptan; after consultation, 97.2% were on a triptan. Before consultation, 30.9% were on a prophylactic drug; after consultation, 70.4% were. 20.8% of patients were medication overusers. Of these medication overusers, 42.4% were overusing an opiate, usually in combination with other analgesics; 21.6% were overusing a triptan. Medication changes made by the neurologists at consultation included a large increase in the use of both triptans and prophylactic medications. Medication overuse, particularly opiate overuse, remains a significant problem in patients with migraine in Canada.
Introduction
Headache is the most common reason for referral to a neurologist (1–4). Migraine in turn is the most common headache type resulting in patient referral to specialized headache clinics (5–8). This is probably because migraine is very common and can cause severe headache with significant disability. A Canadian population-based survey has determined that approximately 7% of adult males and 22% of adult females suffer from migraine (9). From a disability perspective, migraine can have a significant impact on the patient's work and lifestyle (10–12) and result in a significant reduction in patient quality of life (13).
Despite the significant burden imposed by migraine, many migraine sufferers do not seek help from a physician for their headaches (14, 15). For those patients in Canada who choose to see a physician regarding their headaches, most initially see their primary care or family physician, as a physician referral is required to see a specialist. If necessary, primary care physicians can refer migraine patients to a specialist physician for additional help with regard to diagnosis and treatment. Neurologists are the specialty group to which patients in Canada with headache are most commonly referred (16).
In an assessment of migraine care, several features of the Canadian healthcare system are relevant. First, physician visits, both to primary care physicians and to specialists, are covered by provincial medicare systems and are free of charge to the patient. Second, many but not all patients have insurance covering the costs of medications, as most provinces do not have universal pharmacare plans. Third, combination analgesics containing up to 8 mg of codeine per tablet are available to patients in pharmacies ‘over the counter’ without the need for a prescription from a physician.
As is the case in many countries, Canadian physicians have a substantial armamentarium of effective medications with which to treat migraine, including both symptomatic and prophylactic agents. Canadian migraine treatment guidelines have been published (17) to assist physicians in treating their migraine patients. More recently, American migraine treatment guidelines have also been published (18, 19).
In order to investigate the nature of the pharmacological treatment provided to migraine patients in Canada, we studied a sample of 606 patients with migraine referred to five neurology out-patient facilities which were known in their geographical areas to have a special interest and expertise in headache. This migraine patient population provided the opportunity to review the nature of the pharmacological therapy provided by the referring physicians, primarily primary care physicians, and also the medication changes made or recommended by the neurologist consultant. The purpose of this study was to evaluate headache treatment in migraine patients before (i.e. initiated by primary care physicians) and after consultation with a headache neurologist. We also determined the proportion of migraine patients seen by headache neurologists who were overusing symptomatic medications. Although not a population-based study, this study nevertheless provides valuable insights into the demographics and clinical characteristics of those patients at the more severe end of the migraine spectrum who are referred to neurologists specializing in headache in Canada, and the pharmacological treatment that these patients receive.
Patients and methods
Subjects
Data were prospectively collected as part of the Canadian Outpatient Registry and Database (CHORD) project for new patients referred to one of five neurologist out-patient practices in Canada. All neurologists involved were known in their geographical area to have a special interest in the diagnosis and management of headache. The five clinics involved in this study were in Calgary, Hamilton, Ottawa, Toronto and Greater Vancouver. With the exception of the Calgary centre, where patients saw one of two neurologists, all practices were staffed by a single neurologist. Ethical approval for the study was obtained at each centre. All neurologists involved worked as consultants, seeing patients upon referral. The great majority of the patients seen (84%) were referred by family physicians. In Canada, there are no specific criteria for referral of a patient with headache to a specialist, and the decision to refer is a clinical decision made by the referring physician in conjunction with the patient.
To avoid selection bias, consecutive new patients seen by the consultant were entered into the database. In some centres, data collection was interrupted for periods of time for logistical and resource reasons. At one centre (which entered 38 patients), because of limited resources and high patient volumes, patients were entered in a semirandom manner as time permitted. Some degree of selection bias in this small patient contribution cannot be ruled out. Overall, data collection occurred over a period of just over 2 years from September 2001 to January 2004. The exact period of data collection varied somewhat from centre to centre, as additional centres were added over time.
Data collection
Pre-specified data including basic demographic information, diagnosis and other clinical characteristics were collected by the neurologist with the aid of a paper form and the data were later entered into the database. Demographic information collected included age, gender, marital status and employment status. Diagnoses were made according to International Headache Society (IHS) criteria of 1988 (20), with the exception that patients with chronic daily headache (headache on ≥15 days a month) were diagnosed according to Silberstein et al. (21). If patients received more than one headache diagnosis, the one considered most responsible for the referral was listed first and this was the diagnosis used in data analysis. A determination as to whether or not symptomatic medication overuse was present was also made by the neurologist according to the criteria of Silberstein et al. (22), and the type of medication overused was noted. Criteria for overuse included the use of simple analgesics [i.e. acetylsalicylic acid (ASA), acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs)] on more than 5 days a week, opiates or ergotamines on more than 2 days a week, or non-opiate-containing combination analgesics on more than 3 days a week. Overuse was considered present whether these medications were being taken for headache or for another reason. Although the actual reason for taking the medication was not recorded, it would seem likely that the great majority of overused medications were being taken for headache. Patients were asked to estimate the number of headache days they had per month at the time of the consultation. This was done with the assistance of headache diaries if these were available. At the time of the consultation, patients also completed several measures of headache-related disability, including the Headache Impact Test (HIT-6) (23, 24) and the Migraine Disability Questionnaire (MIDAS) (25–27).
Information on the use of medications for headache at intake was obtained from a detailed patient history and medication use information included in the referral letter written by the referring physician. Headache medications, both prescribed and recommended by the specialist, were carefully recorded as well and entered into the database. This included both symptomatic and prophylactic pharmacotherapy.
Symptomatic medications were classified as follows: triptans, single acetaminophen or a NSAID, acetaminophen/NSAID combination drugs, antinauseants, single opiates, opiate/analgesic combination drugs, ergotamines, barbiturate/opiate/analgesic combination drugs, and steroids.
Data analysis
All information collected was entered into the CHORD computer database which was specifically designed to collect data from patients with headache disorders. All data were stripped of specific patient identifiers before they left each of the five headache clinics, and analysed centrally. Descriptive statistical analyses were performed using SAS for Windows (release 8.02; SAS Institute Inc., Cary, NC, USA; 1999–2001).
Results
Data were collected on 865 patients seen in the five headache centres. Of these patients, 606 received either a migraine diagnosis according to IHS diagnostic criteria (20) or a diagnosis of transformed migraine (21). The data from these 606 patients were analysed separately and form the basis of this report. The number of migraine patients (and data collection periods) for each of the five centres were as follows: Centre 1: 254 patients (November 2001 to February 2003); Centre 2: 170 patients (December 2002 to January 2004); Centre 3: 97 patients (September 2001 to October 2003); Centre 4: 53 patients (May 2003 to December 2003); Centre 5: 32 patients (June 2002 to January 2004).
Demographic and clinical features
Demographic and clinical characteristics of the migraine patient population are reported in Tables 1 and 2. The ages of the migraine patients in the sample ranged from 5 to 82 years, while the mean age was 39.7 years (SD ± 12.9). Approximately half of the patients were between the ages of 30 and 49 years (Table 1). The majority of migraine patients in the sample were female (n = 500; 82.5%) and approximately half were married or living common law (n = 341; 56.3%). More than half of the migraine patients were employed outside of the home (n = 365; 60.2%), either full time (47%), or part time (13.2%). A further 12% (n = 72) identified themselves as full-time homemakers. Only 3% (n = 18) of the patients were receiving disability benefits because of their migraines, but an additional 5.3% (n = 32) were receiving a disability pension for other reasons. Only 6.8% (n = 41) gave their work status as unemployed.
Demographic characteristics of migraine patients (n = 606)

Clinical characteristics of migraine patients (n = 606)

Percent of total patients with a migraine diagnosis.
Most patients were not subclassified beyond two digits (Migraine With Aura 1.2).
Twenty-two patients had missing HIT-6 scores; percent is out of 584 patients.
Twenty-five patients had missing MIDAS scores; percent is out of 581 patients.
The majority of patients referred to the headache specialists in our study were given a migraine diagnosis (n = 606; 70%). Within the subgroups of migraine diagnoses, migraine without aura was the most common diagnostic category represented in the sample (n = 284; 46.9%), followed by transformed migraine with/without medication overuse (n = 216; 35.6%) (Table 2).
Nearly half of the migraine patients reported experiencing headache on ≥15 days per month (n = 278; 45.9%). Approximately 21% of patients (n = 125; 20.8%) were identified by the neurologists as symptomatic medication overusers.
Headache-related disability was substantial among the migraine patients in this sample. Eighty-two percent (n = 477; 81.7%) of patients had HIT-6 scores of ≥60, which corresponds to severe disability. Three hundred and fifty patients (n = 350; 60.2%) had MIDAS scores ≥21, indicating severe disability for that disability scale also.
Symptomatic medication use
Symptomatic medication use is summarized in Table 3. Some patients took two or more medication types and therefore the percentages add up to more than 100%. The percentage of patients taking each medication type is calculated as a percentage of the entire migraine population (606 patients) even though 18% of patients were taking no symptomatic medication before consultation. After consultation, 2.2% still were not taking a symptomatic medication.
Symptomatic drug use for migraine patients before and after initial consultation with a headache neurologist (n = 606)

Other single NSAIDS: Asa/caff, celecoxib, diclofenac, mefenamic acid; other antinauseants: domperidone, promethazine; other opiate/analgesic comb.: Asa/cod/propox, Asa/oxycodone; other single opiates: butorphanol, codeine, pentazocine; other ergotamines: Ergot/caff/bell/pento, Ergot/caff/dimenhydrate, Ergot/caff/diphenhydram, Ergotamine; other steroids: dexamethasone, prednisone.
The great majority (82%) of patients were taking some form of symptomatic medication prior to consultation. Most patients were taking simple analgesics (acetaminophen) or NSAIDs (n = 357; 58.9%) prior to consultation (Table 3). Triptans were used by a somewhat smaller patient group (n = 295; 48.7%). The third largest patient group (n = 147; 24.3%) was taking opiate-containing combination analgesics, usually with codeine. In addition, 8.7% of patients used opiate preparations which were not part of combination analgesics, and a further 4.6% used codeine-containing combination analgesics which also contained barbiturates.
After consultation with a headache neurologist, 97.8% (n = 592) of patients had a symptomatic medication for their headaches continued from before consultation, prescribed, or recommended. At consultation, virtually all patients either had their triptans continued, or a new one prescribed. Over 97% of patients were on a triptan after consultation, compared with 48.7% before consultation. After consultation, simple acetaminophen/NSAID formulations was the second most common category of symptomatic medications used; 61.9% (n = 375) of patients. The consultants more than doubled the use of antinauseant drugs, with almost 20% (n = 114) of patients taking antinauseant drugs after consultation compared with 7.6% (n = 46) before consultation. The percentage of patients taking opiates/analgesic combination drugs decreased to 17.3% (n = 105) after consultation with a headache neurologist from 24.3% (n = 147) before consultation.
Prophylactic drug use
Prophylactic drug use markedly increased after consultation with the headache neurologist (Table 4). Prior to consultation, only 30.9% (n = 187) of migraine patients were taking prophylactic medications for their headaches, whereas after consultation this increased to 70.4% (n = 427). Amitriptyline was by far the most common prophylactic medication used prior to consultation, with almost three times as many patients receiving amitriptyline as were receiving propranolol, the next most widely used prophylactic drug prior to consultation. At consultation, another 21% of patients were given amitriptyline, while only a few (2.7%) had their amitriptyline discontinued. Thus, after consultation, amitriptyline remained the most frequently used prophylactic for migraineurs (n = 196; 32.3%). Topiramate, a relatively new medication for the prophylactic treatment of migraine, was used by only 2.3% of patients prior to referral. After consultation, it was the second most commonly used prophylactic with 72 (11.9%) patients on topiramate. Nortriptyline use was very low prior to consultation (1.7%), but after consultation many more patients (n = 67; 11%) were treated with nortriptyline.
Prophylactic drug use for migraine patients before and after initial consultation with a headache neurologist (n = 606)

Percents based on 606 patients. Patients may be on more than one prophylactic.
Other: naproxen, methysergide, metoprolol, clonidine, celecoxib, desipramine, diltiazem.
Before consultation: 187 (30.9%) patients were taking a prophylactic. After consultation: 427 (70.4%) patients were taking a prophylactic.
At consultation, a large number of patients who were not on prophylaxis at the time of consultation were started on prophylaxis (n = 249; 41.1%) (Table 5). Of patients in our sample, however, 28% (n = 170; 28.1%) were not on a prophylactic at the time of consultation, and were also not started on one by the consultant. Among the remaining patients, most patients either were instructed to continue taking the prophylactic medication that had been prescribed prior to consultation (n = 96; 15.8%) or had a new prophylactic medication added to their previous one (n = 48; 7.9%).
Summary of prophylactic use in migraine patients after consultation (n = 606)

Symptomatic medication overuse
One hundred and twenty-five patients (n = 125; 20.6%) were identified by the headache neurologists as medication overusers at consultation. Table 6 shows the types of medications that were overused by these patients. Although acetaminophen and NSAID overuse was common, this overuse usually occurred along with overuse of other medications, often in combination analgesic form. Opiates, usually in combination with other medications, were overused by over 40% of medication overusers. Isolated triptan overuse occurred in 12.8% of overusers and another 8.8% overused triptans along with another medication. Overall, the majority of patients who overused symptomatic medications were overusing more than one type of medication.
Summary of types of medications overused among migraine patients identified by headache neurologists as medication overusers (n = 125)∗
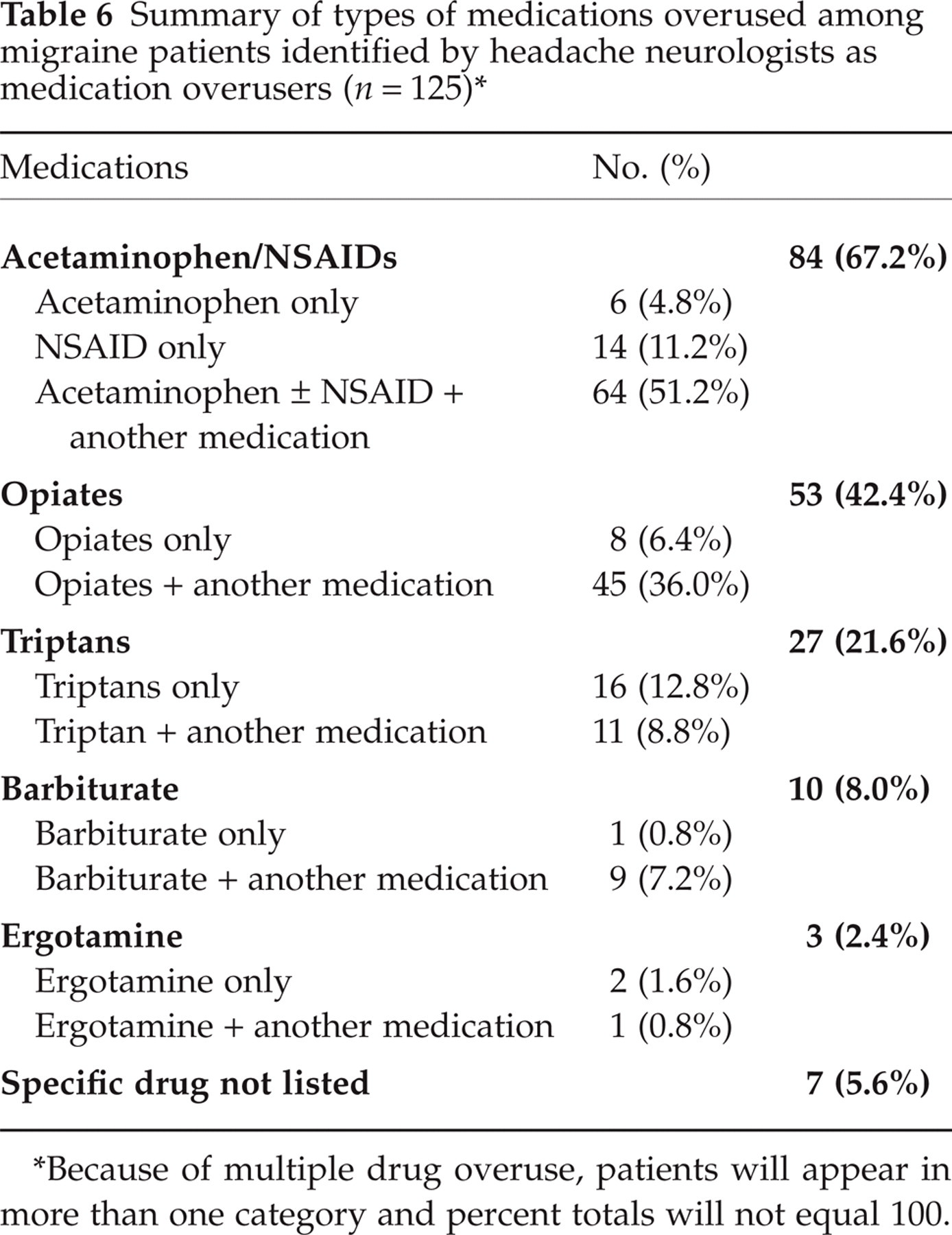
Because of multiple drug overuse, patients will appear in more than one category and percent totals will not equal 100.
Discussion
Our study has confirmed that the majority of patients with headache referred to neurologists with a special interest in headache in Canada have migraine. These migraine sufferers are for the most part (72%) between the ages of 20 and 50 and are still working outside the home (60%). Another 12% were full-time homemakers. The migraine patients referred to headache specialists in Canada do, however, as a group experience major disability as a result of their headaches. Over three-quarters of them indicated severe impact of headache on their lives on the Headache Impact Test questionnaire, and well over half scored in the severe disability range on the MIDAS questionnaire which is designed to measure the effect of headache on work and other aspects of a patient's life. Three percent of the patients with migraine were already on disability pensions for headache at the time of consultation. Headache frequency is very high in this referred migraine patient population, with almost half of them reporting headache on ≥15 days a month. At the same time, medication overuse is a big issue in this patient population. Over 20% of the patients with migraine had symptomatic medication overuse.
Although ideal migraine therapy includes many non-pharmacological approaches, such as lifestyle changes and headache trigger avoidance, pharmacological therapy also has a very large role, particularly in the more severely affected segment of the migraine population. A number of migraine treatment guidelines have been published (17–19, 28) to provide guidance for pharmacological therapy of migraine. These stress the importance of providing the best symptomatic medication possible for the control of individual migraine attacks, of providing prophylactic medications to reduce migraine headache frequency where appropriate, and of avoiding symptomatic medication overuse. Generally accepted limits for the frequency of use of the various migraine symptomatic medications have been published (20, 22).
Quality of care for migraine patients is problematic in at least four areas. Previous studies have indicated that migraine treatment deviates from published guidelines in that one of the most effective symptomatic migraine classes, the triptans, are underutilized, and that too few patients are on migraine prophylactic drugs (14, 29–31). In addition, migraine tends to be underdiagnosed in the general population (12, 32), and medication overuse remains a problem (33–35).
Our study of a patient population referred to neurologist headache specialists in Canada confirms that most of these remain a problem in this segment of the migraine population which is likely to be at the severe end of the migraine spectrum. We cannot comment on whether underdiagnosis by the referring physicians is a problem, as many referral letters do not include a diagnosis. However, the fact that so many of the patients diagnosed with migraine by the specialist (>50%) were not taking a triptan despite disability severe enough to warrant referral would suggest that underdiagnosis may still be a problem even in this severely affected patient population. There are other barriers, including financial ones, to using triptans, but after discussion with the patient, the headache specialist prescribed or recommended a triptan for virtually every one of the migraine patients seen (97.2%).
Clearly, triptans are greatly underutilized by patients with severe migraine in Canada. This is despite their proven ability to increase workplace productivity and to improve quality of life in patients with migraine (36, 37). Similarly, prophylactic medications were also underutilized in the care of these patients prior to referral. Before consultation, less than one-third of this patient population was taking a prophylactic drug, although a number of these may have taken some in the past. Based upon the prescribing of the headache specialist, it would appear that prophylaxis was in fact appropriate for over 70% of this patient population.
Medication overuse as a potential exacerbating factor in migraine has been discussed for decades (38–40) and the benefits of stopping medication use in many migraine sufferers have been documented (38, 41). Nevertheless, fully 20% of the patients referred to the headache specialists in our study were felt to meet standard criteria for medication overuse. Although the precise extent of the role of medication overuse as an exacerbating factor in frequent migraine is still debated (12, 42), it seems likely that it plays a negative role in the management of a significant proportion of the patients referred to headache specialists in Canada. It is important to recognize, however, that medication overuse is not the only factor underlying high headache frequency in patients with migraine. Of migraine patients in our patient population, 46% had headache on ≥15 days a month, but only 21% of our patient population was felt to overuse symptomatic medication by the headache specialist.
The pattern of medication overuse in our patient population is of some interest when compared with that reported by Bigal et al. (34) from a large American headache centre. In that study, 48% of medication overusers were overusing butalbital-containing compounds, in contrast to only 8% of medication overusers in our patients. Canadian physicians have clearly become very cautious in their use of these drugs for migraine. On the other hand, they may have compensated by using more opiate-containing analgesics without barbiturates. In our medication overuser population, 42.4% overused an opiate-containing analgesic, compared with 32.8% in the study by Bigal et al. (34). The percentage of overusers overusing triptans was remarkably similar in the two studies: 21.6% in our study and 17.8% in the American study.
To summarize, our data would suggest room for improvement in migraine care in Canada on at least three levels: tripan use, prophylactic use and prevention of medication overuse.
Our study quantifies to some degree the medication changes made when neurologist headache specialists in Canada evaluate patients referred for the most part by primary care physicians. Several general principles stand out. First, the use of triptans as symptomatic migraine medication is greatly increased. Second, the use of prophylactic medications is greatly increased in that it was more than doubled. Third, the use of antinauseants, in particular the use of metoclopramide, is more than doubled. Fourth, the use of codeine-containing combination analgesics is modestly reduced, from use by 24.3% of patients to 17.3% of patients, although whether the advice to discontinue them by the specialist is actually carried out in practice cannot be ascertained from our data.
The medication changes made by the headache specialists in our study are in some ways very similar to those reported from an Italian headache centre (31). In that study, medication use was compared in patients presenting for the first time to an Italian headache referral centre, with another patient population seen for a follow-up visit in the same centre. Although the follow-up population may have been somewhat selected, the findings were that the use of triptans was more than tripled by the headache specialists from 9.1% in the patients referred to 31.8% in the patients seen in follow-up. Also similar to our study, the use of prophylactics was greatly increased by the specialists. At referral in the Italian study, only 16.8% were taking a prophylactic, compared with 58.2% at the follow-up visit. Interestingly, in the Italian study there appears to have been very little opiate consumption by patients, both before and after the consultation, in sharp contrast to the opiate use observed in our patient population.
A number of other observations can be made from our data. Ergotamines were little used either by the primary care physicians or by the specialists, although the specialists did use dihydroergotamine to a small extent. Barbiturate-containing analgesics were not widely used, although almost 6% of patients were taking these prior to the consultation. Surprisingly, this percentage did not change significantly after the consultation. This observation is interesting in light of the controversy surrounding these drugs and their potential for abuse. Among NSAIDs, ibuprofen was by far the most widely used prior to consultation. Its use as a single drug significantly exceeded that of acetaminophen, consistent with evidence that ibuprofen is more effective in migraine (43). In general, the consultants reduced the use of acetaminophen, while NSAIDs were widely used by both consultants and primary care physicians. Codeine-containing combination analgesics were widely used, especially prior to consultation. Our analysis cannot distinguish, however, between over-the-counter preparations and preparations prescribed by the primary care physicians. Specialists prescribed injectable sumatriptan five times as often as family physicians. After consultation, almost 6% of patients in this difficult migraine population were receiving injectable sumatriptan. Nasal triptan formulations were little used, both by primary care physicians and by specialists.
Although the specialists greatly increased the use of prophylactic medications, it is of interest to note that for both physician groups, amitriptyline was by far the most commonly used prophylactic. This probably reflects the severe nature of the migraine suffered by this patient population, and the high prevalence of comorbidities, including sleep disturbances and depression. β-Blockers were used much less in this patient population, with relatively similar usage by both physician groups. Not surprisingly, the specialists made much more use of newer prophylactics such as topiramate. Topiramate was in fact the second most frequently used prophylactic by specialists, consistent with the large evidence base supporting its use (44–47). The use of other anticonvulsants, including valproate and gabapentin, for migraine prophylaxis was much less. Surprisingly, nortriptyline was the third most commonly used prophylactic by the specialists. There is little evidence base for its use, aside from its chemical similarity to amitriptyline. The use of nortriptyline by the headache specialists is consistent, however, with the American Academy of Neurology treatment guidelines, where, despite only Class C evidence supporting its use, it is listed as very effective in terms of the clinical impressions of the experts preparing the guidelines. NSAIDS were used very little for migraine prophylaxis in our patient population.
An interesting observation is that when good antimigraine drugs were used by the primary care physicians, the specialist usually did not change them. Primary roles of the specialist appear to have been to improve prescribing where it was inadequate, and perhaps to give the patient the benefits of newer drugs. One might conclude that better education of primary care physicians in the care of patients with severe migraine could reduce the need for specialists to improve the drug use of these patients. On the other hand, it should be recognized that given the time constraints in the primary care physicians office, and the broad spectrum of medical conditions which the primary care physician has to deal with, it may not be possible to achieve a high level of care for the patient with severe migraine in that setting.
Symptomatic medication overuse is a particularly difficult problem for the patient with frequent severe migraine and there is much more to be done with regard to this issue in Canada. Opiate-containing drugs are of particular concern, in part because of the addictive potential of opiates, and also because medication-induced headache resolves much more slowly upon drug withdrawal when it results from analgesic overuse than when it results from triptan overuse (41). Over 38% of patients were taking opiate-containing analgesics prior to consultation, mainly in the form of combination analgesics. While opiates can play a useful role in the care of some patients with migraine, their use needs to be carefully controlled in most patients through prescription monitoring, patient diaries and good patient education. In our patient population, almost one in 10 was considered by the specialist to be overusing opiates. This was double the number that was overusing triptans.
Our study has both strengths and weaknesses. The population studied was large, comes from three of Canada's 10 provinces, and probably reflects accurately the headache population referred to neurologists with a special interest in headache in Canada. In terms of the medication data, it reflects the practices of six neurologists rather than a single centre. Participating neurologists did know that one of the objectives of the study was to document the changes made in the management of the patient by the neurologist. It is possible that this may have influenced the treatment recommendations made by the neurologist to some extent, but we consider this unlikely as all neurologists involved were already specialized in the field of headache, and the intent of the study was to publish pooled data. Because of the number of neurologists involved, there are likely to be some individual differences in the way certain aspects of the data were recorded, although this was minimized by the use of a common database and through discussions at investigator meetings. As an example, 45.9% of our migraine patients had ≥15 days of headache per month, but only 35.6% were given a diagnosis of transformed migraine. Going strictly by the diagnostic criteria, all 45.9% might have qualified for a diagnosis of transformed migraine, but clearly for some of these patients it was indicated that the diagnosis of migraine with or without aura was the main reason for the referral. Similarly, although 20.8% of patients were labelled as medication overusers by the neurologist, only 18% of patients received a diagnosis of transformed migraine with medication overuse as the diagnosis most responsible for the referral. A specific structured interview process was not used, and this may have also contributed to some variation between neurologists in data collection. However, to minimize variability and to ensure comprehensive data collection, a standardized data collection form was provided to all centres, although this was modified to some extent at some centres to allow for efficient data collection during the course of the consultation. Another limitation is that our data on patient drug use represent a snapshot at a single point in time when the patient saw the consultant for the first time. For example, patients may have taken a prophylactic in the past, but were no longer taking it when they saw the consultant. These data were not collected. Nevertheless, our conclusions remain valid in the sense that, given their clinical condition at the time of consultation, many patients who were not on a prophylactic at that time apparently should have been, given the decisions made by the specialist. Similarly, some patients had taken a triptan in the past, but were no longer doing so at the time of consultation. Many of the patients referred, however, were indeed triptan naive, as data available on 556 of the patients referred indicated that 203 (36.5%) had never taken a triptan in the past. Despite these limitations, we feel that our data paint a portrait of migraine treatment for this patient population which is not available from other sources and which is robust enough to serve as a basis for decision making to improve the lot of these patients in the future.
In summary, our data provide a window into the patient population referred to headache specialists in Canada. This population is dominated by patients with migraine who are using a large variety of medications in an attempt to control their headache disorder. Prior to specialist referral, this treatment is often suboptimal according to current guidelines (17–19, 28), with underutilization of triptans and of prophylactic medications. Clearly, much remains to be done to improve the treatment of the patient with difficult migraine.
Footnotes
Acknowledgements
The Canadian Headache Outpatient Registry and Database project was funded by a research grant provided by GlaxoSmithKline. The project is carried out under the auspices of the Canadian Headache Society.