
Abstract
Background: Current textbook knowledge states that patients with chronic migraine and medication overuse should be withdrawn from acute medication before initiating preventive drug therapy.
Overview: This recommendation is based on the clinical impression that patients with chronic migraine and medication overuse are refractory to preventive therapy. Recently, however, four randomised trials, two with topiramate and two with onabotulinum toxin A, showed that about half of patients with chronic migraine and medication overuse will respond to these treatments and show both a reduction in migraine days and intake of acute medication.
Conclusions: Therefore, we propose to educate patients on the mechanisms of medication overuse and motivate them to reduce intake frequency. Patients who fail should be offered either topiramate or onabotulinum toxin A in combination with behavioural therapy and regular exercise. If this approach fails, patients should be offered withdrawal therapy.
Introduction
Frequent or regular use of certain medications (e.g. barbiturates, opioids and triptans) used for the treatment of acute episodes of primary headache (migraine, episodic tension-type headache) can lead to deterioration of the pre-existing headache. This form of headache is called medication overuse headache (1). Medication overuse headache is a frequent problem in tertiary headache centres, especially in patients with chronic migraine. Textbook recommendations and non-evidence-based guidelines postulate that the initiation of headache prevention in patients with migraine is ineffective unless the overused medication(s) is stopped (1–3). Furthermore, others believe that headache prophylaxis is unnecessary, because simply stopping the overused medication will obviate the need to begin a daily preventive medication (4). Therefore, detoxification has been recommended before preventive treatment with drugs or non-drug treatment approaches are initiated (5). I will argue that new scientific evidence exists from recently published randomised trials that detoxification prior to initiation of preventive therapy in all patients with chronic migraine and medication overuse is not necessary. An important aspect has to be kept in mind: excessive use of acute medication (often referred to as medication overuse) is not identical to medication overuse headache, which is a specific secondary headache disorder defined by the International Classification for Headache Disorders (ICHD 8.2) (1). A patient might experience 11 migraine days per month and take triptans on 11 days. This fulfils the criteria for excessive use of medication, and technically also fulfils the ICHD 8.2 criteria for triptan overuse. However, because diagnosis requires judgement by the clinician, in this instance the frequency of headache days most probably is not related to the intake of triptans, but the triptan use is as a result of the consequence of frequent migraine headaches. Another migraine patient may have developed daily headache, some of which fulfil the criteria for migraine. If this patient is also taking triptans or opioids on a daily basis there is a high likelihood that this clinical situation is the result of the medication overuse and that the patient is experiencing secondary medication overuse headache, in addition to migraine. An important differentiating factor with regard to the influence of excessive use of medication is that there should be evidence of regular overuse for > 3 months of one or more acute treatment drugs and that the headache has developed or markedly worsened during the period of medication overuse. In my clinical experience, triptan overuse is the most common reason that patients with migraine develop medication overuse headache.
As agreed during the debate, every patient who is excessively overusing acute medications should be counselled on the importance of reducing medication intakes and that there is a role for detoxification in the treatment of medication overuse headache. Furthermore, there was agreement that there is a role for preventive treatment being prescribed while sorting out the influence of medication overuse for individual patients. Where I believe that my opponent and I disagree is that I do not support the position that an aggressive detoxification programme is required as a first step for all patients with evidence of excessive use of medication before the initiation of preventive medication. Availability of new scientific evidence of the effectiveness of topiramate and onabotulinum toxin A in patients with chronic migraine and medication overuse has persuaded me to revise my clinical treatment approach in these patients. As a result, I have observed improved clinical outcomes for these difficult-to-treat patients. Additionally, an aggressive detoxification programme may not be optimal for a number of practical reasons that should not be ignored. First, these programmes are expensive, particularly because rising healthcare costs are major economic concerns. Secondly, the programme by nature is disruptive to a patient’s daily life and it may be difficult or not feasible for many patients to take 5 days off work, particularly because these patients have already missed a substantial amount of work due to their headaches. Finally, detoxification can be uncomfortable and may cause unwarranted anxiety.
The topiramate experience
During the development programme of topiramate for the prophylaxis of migraine, two trials were initiated investigating topiramate versus placebo for the treatment of chronic migraine (6,7). The European trial allowed excessive use of acute medication for the treatment of migraine attacks (8). Most patients in this trial overused medication (78%), but a confirmatory diagnosis of medication overuse headache was not made. The majority overused triptans (Figure 1). In the US trial medication overuse was an exclusion criterion, but overuse was defined not according to ICHD-II, but as 4 days or more per week of acute medication use. Therefore, using the protocol definition, 37% of patients recorded medication overuse (mostly triptans) during baseline (Table 1) (8).
Acute medication overuse in the US and EU trials, within the topiramate- and placebo-treatment groups. In both trials, ergots were not overused in either of the treatment groups. ‘Any combination’ refers to any combination of triptants, opioids and analgesics. Key differences between US and European Union trial patient populations Some subjects could be classified as having medication overuse headache via the current International Classification of Headache Disorders, second edition (ICHD-II) definition.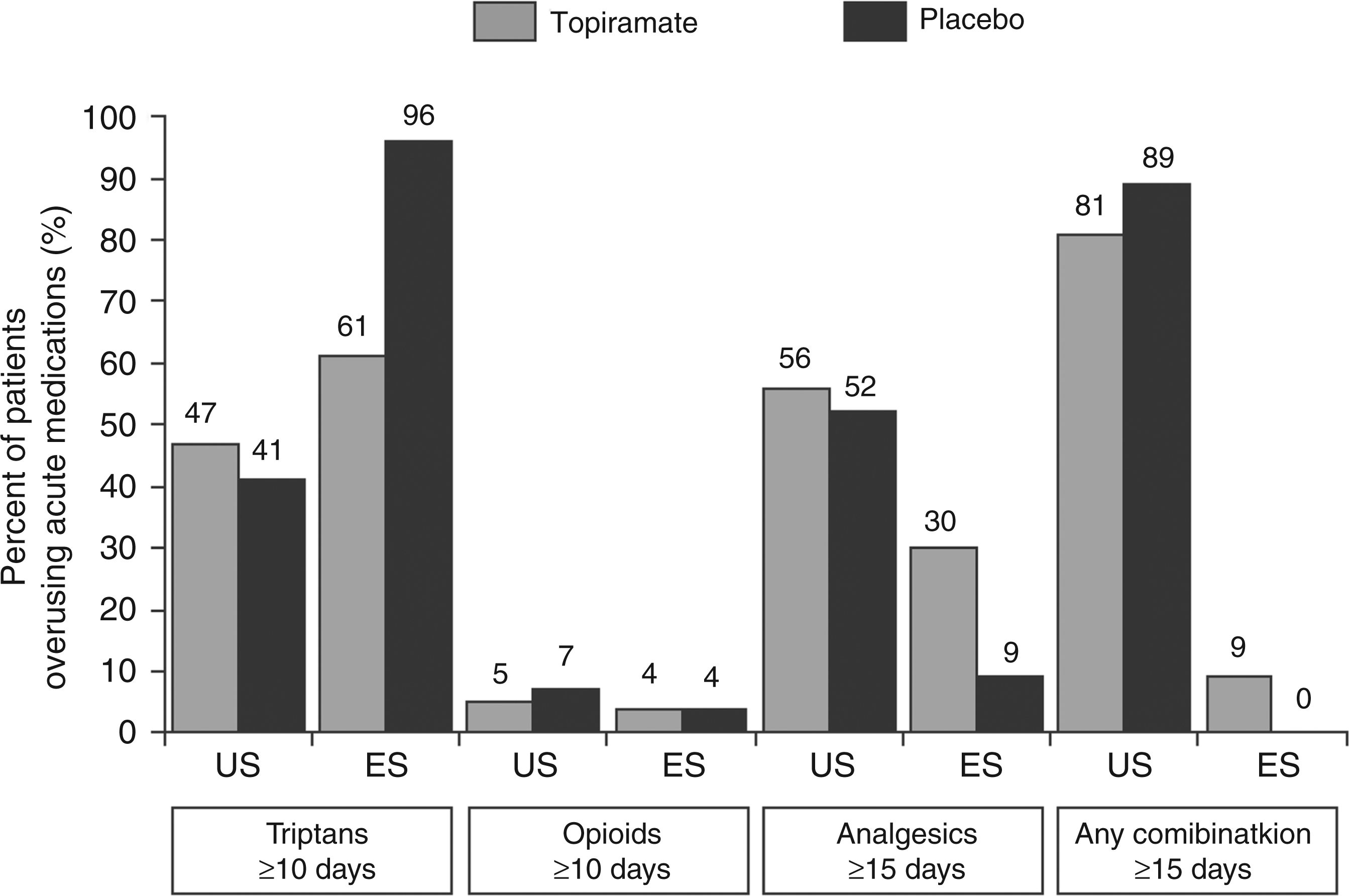

The US trial consisted of 306 patients, whereas the EU trial recruited 59 patients. Taking all patients together, both trials showed a significant reduction in migraine/migrainous days for topiramate versus placebo. A post hoc analysis in patients with medication overuse in the US trial showed a strong trend in favour of topiramate (p < 0.059). In the EU trial, patients with medication overuse achieved a significant reduction in the mean number of migraine days with topiramate versus placebo (p < 0.03). In the EU trial, 63% of patients in the topiramate group fulfilled the criteria for medication overuse at baseline, but only 17% at week 16.
In conclusion, in these well-controlled trials, topiramate was shown to be effective in the prophylaxis of chronic migraine, both in patients with and without medication overuse.
The onabotulinum toxin A experience
Onabotulinum toxin A was investigated in patients with chronic migraine in two placebo-controlled trials (9,10). Each study had a 28-day baseline screening period, a 24-week double-blind phase with two injection cycles (every 12 weeks), and a 32-week open-label phase with three injection cycles. Patients had to have ≥15 headache days per month, of which ≥50% were migraine or probable migraine days. Allergan prospectively stratified patients who were excessively using acute medications or not (labelling these subgroups as ‘medication overuse yes/no’) based on patient-reported frequency of acute medication use during the 28-day baseline period and not based on a diagnosis of medication overuse headache (ICHD-II 8.2). A modified definition that was similar to the criteria defined in ICHD-II 8.2 (1), but required evidence of regular use on ≥2 days per week (which is not a requirement per ICHD), was used for stratification. Headache experts served as the investigators for these Phase 3 trials and per protocol they were to recruit patients who had a primary migraine headache disorder and they were to exclude patients who had a secondary headache disorder. The PREEMPT 1 study missed its primary endpoint (headache episodes), but was significantly in favour of onabotulinum toxin A for most secondary endpoints (9). The PREEMPT II study was positive for all endpoints (10). The pooled analysis (11) showed significant improvements compared to placebo in multiple headache symptom measures and significantly reduced headache-related disability and improved functioning and quality of life.
At the AAN congress in 2010, Silberstein et al. presented the results of a subgroup analysis in patients with medication overuse in the two PREEMPT trials (12). Of 1384 patients 65.3% (n = 904) were assigned to the ‘medication overuse-yes’ stratum. Most of the patients overused triptans or combination analgesics; very few (1.7%) overused opioids.
Efficacy on OnabotulinumtoxinA in Migraine Patines with Baseline Medication Overuse

HIT = Headache Impact Test
HIT-6 scores of 36-49 indicates little or no impact; 50-55, moderate impact; 56-59, substantial impact; 60-78, severe impact.
In conclusion
The analysis of the subgroup of patients with baseline medication overuse in the PREEMPT studies shows that onabotulinum toxin A is effective, resulting in clinically meaningful improvements for multiple headache symptom measures and significantly reducing headache-related disability and improved functioning and quality of life.
Practical consequences
The new information learned from these recent scientific studies reporting results of the topiramate and onabotulinum toxin A studies in patients with chronic migraine and medication overuse has changed my approach to this complex patient group. Until two years ago, I insisted on performing detoxification before initiating preventive therapy for all patients overusing acute medications. Now we follow a new approach:
Patients are counselled about the consequences of too frequent intake of medication to treat acute migraine attacks and encouraged to reduce the intake to <15 days per month for simple analgesics and <10 days per month for triptans and combination analgesics (opioids are not used in Europe for the treatment of migraine). About 50% of patients will achieve this goal by themselves. All patients should be offered a non-drug treatment and in the majority, additional preventive drug therapy. Taking evidence from randomised controlled trials into consideration, topiramate or onabotulinum toxin A should be offered as a treatment for this condition. About 50% of patients with chronic migraine and medication overuse will respond and show a significant reduction in headache days. Unfortunately we do not have enough evidence on whether other drugs usually recommended for the prevention of episodic migraine are effective in chronic migraine with medication overuse. Small underpowered trials suggest possible efficacy for amitriptyline (13,14), gabapentin (15) or valproate (16,17). The remaining patients probably really have medication overuse headache, and thus are admitted to a rigorous detoxification programme, which is executed in a day-care setting for 5 days, including behavioural therapy and an exercise programme. Migraine prophylaxis is not prescribed to these patients unless indicated after they complete the detoxification programme.
Conclusion
As new scientific evidence has emerged, we have changed our approach to patient care. Using our new approach to treat patients with chronic migraine and migraine overuse headache we were able to reduce the percentage of patients who need detoxification to 25%.
The ICHD 8.2 medication overuse criteria were published in 2005, before the new scientific information discussed above was available. Some of the guidance provided in the criteria is now outdated and inaccurate (e.g. document states: “patients rarely respond to preventative medications whilst overusing acute medications”). Because the ICHD are undergoing revision, it is suggested that guidance pertaining to preventative medications for patients with chronic migraine and migraine overuse headache should be revised.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.