
Abstract
Background
Occipital nerve stimulation (ONS) has been proposed to treat chronic medically-intractable cluster headache (iCCH) in small series of cases without evaluation of its functional and emotional impacts.
Methods
We report the multidimensional outcome of a large observational study of iCCH patients, treated by ONS within a nationwide multidisciplinary network (https://clinicaltrials.gov NCT01842763), with a one-year follow-up. Prospective evaluation was performed before surgery, then three and 12 months after.
Results
One year after ONS, the attack frequency per week was decreased >30% in 64% and >50% in 59% of the 44 patients. Mean (Standard Deviation) weekly attack frequency decreased from 21.5 (16.3) to 10.7 (13.8) (p = 0.0002). About 70% of the patients responded to ONS, 47.8% being excellent responders. Prophylactic treatments could be decreased in 40% of patients. Functional (HIT-6 and MIDAS scales) and emotional (HAD scale) impacts were significantly improved, as well as the health-related quality of life (EQ-5D). The mean (SD) EQ-5D visual analogic scale score increased from 35.2 (23.6) to 51.9 (25.7) (p = 0.0037). Surgical minor complications were observed in 33% of the patients.
Conclusion
ONS significantly reduced the attack frequency per week, as well as the functional and emotional headache impacts in iCCH patients, and dramatically improved the health-related quality of life of responders.
Introduction
Cluster headache is a primary headache belonging to the group of the trigeminal autonomic cephalalgias, and is characterised by strictly unilateral short-lasting pain attacks associated with prominent parasympathetic features (1). Chronic cluster headache is diagnosed after one year without remission or with remission periods lasting less than one month. Once the chronic cluster syndrome is established, the prophylactic medical treatment (verapamil, lithium) often fails to prevent the attack occurrence. Medically-intractable chronic cluster headache (iCCH) is one of the most painful conditions in humans, often referred to as “suicidal headache”, justifying surgical solutions such as deep brain stimulation, occipital nerve stimulation (ONS) or stimulation of the spheno-palatine ganglion (2).
Occipital nerve stimulation (ONS) was initially proposed to control occipital neuralgia (3) and has been used since 2007 to treat severe iCCH (4,5). However, only a few data are available, extracted from small open trials. These series reported an overall success rate (usually defined by attack frequency decrease >50 %) of about 60–70%, but the evaluation was limited to the attack frequency and global impression of change, without data concerning the functional and emotional impacts of the headache and the quality of life of the patients. We report here the multidimensional outcome of a large series of iCCH patients treated by ONS within a French and Swiss multidisciplinary network involved in treatment of primary headache by ONS.
Methods
Patients
All the patients were included in the French database of occipital nerve stimulation in the treatment of refractory chronic headache disorders (https://clinicaltrials.gov, identifier NCT01842763), a multi-centric registry collecting prospective data for chronic headache patients undergoing ONS. All the patients signed an informed consent for data collection and the registry obtained all the required legal and ethical approvals. Inclusion criteria for the current study were: diagnosis of chronic cluster headache according to ICHD-II criteria (6), duration of over three years, daily attacks, resistance to more than two pharmacological prophylactic treatments with adequate trials including verapamil up to 960 mg/day, lithium with plasma level from 0.6 to 1 mEq/l and association of both, in the absence of adverse events (7,8), treatment by ONS, with follow-up superior to one year.
The surgical ONS implantation technique and hardware (Genesis, ST Jude Medical or Prime Advanced, Medtronic) varied across the participating centres but followed key recommendations: permanent, bilateral, stimulation inducing paresthesias in the occipital region, via subcutaneously implanted electrodes connected to a generator.
Stimulation was considered as effective when it induced perceptible paresthesias in the occipital region. Other situations were considered as hardware dysfunctions. Stimulation parameters were individually adjusted to induce comfortable and well-tolerated paresthesias, in the widest possible occipital area. Consequently, the stimulation parameters varied widely across the patients (amplitude 1.5–9 V; frequency 30–100 Hz) and could be changed with time. Most of the patients used continuous permanent stimulation, but a few of them switched off the stimulation during the night because the perception of paresthesias hampered their falling asleep.
Data collected
Data were prospectively collected within the network database, before the surgery and three (M3) and 12 (M12) months after ONS implantation. Data extracted for this study were collected by 10 centres and included socio-demographic characteristics (sex, age, and professional status); weekly attack frequency (assessed by a prospective attack diary), mean attack duration (estimated in minutes), mean attack intensity (assessed by a numeric scale from 0 to 10) and medication related to cluster headache (considering both prophylactic and abortive treatments).
The functional impact of cluster headache was assessed using the French version (9) of the short version Headache Impact Test (HIT-6) (10). HIT-6 considers a broader spectrum of the measurement of headache impact, including social-role functioning, pain, emotional distress and well-being, cognitive, functioning and vitality . It quantifies the headache impact by a score from 36 to 78, a score over 60 indicating a very severe impact (11).
Emotional impact was assessed by the French version (12) of the Hospital Anxiety Depression Scale (HADS). HADS considers seven anxiety items alternating with seven depression items, final sub-scores for both anxiety and depression ranging from 0 to 21. Anxiety and depression impairment are commonly defined by anxiety (HAD-A) and depression (HAD-D) sub-scores > 7.
Disability was assessed by the French version (13) of the Migraine Disability Assessment (MIDAS) questionnaire (14), which focuses on lost days and days with reduced productivity over the last three months. The score allowed assignment of patients to one of the four MIDAS grades (0–5, grade I, no disability; 6–10, grade II, some disability; 11–20, grade III, significant disability; >21, grade IV, severe disability).
Health-related quality of life was assessed by the French version of the EQ-5D health questionnaire (15,16). The EQ-5D provides a simple descriptive profile and a single index value for health status. We used the EQ-5D-3L version that associates the EQ-5D-3L descriptive system and the EQ visual analogue scale (EQ VAS). The EQ-5D descriptive system considers five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The EQ VAS records the respondent’s self-rated health on a visual analogue scale where the endpoints are labeled ‘best imaginable health state’ and ‘worst imaginable health state’.
Patient’s global impression of change (PGIC) was used as a patient-related outcome for each post-implantation evaluation, considering seven items: very improved, improved, slightly improved, unchanged, slightly worsened, worsened, very worsened.
Evaluation
ONS efficacy was evaluated by changes occurring after three and 12 months of stimulation compared to baseline and by the patient’s global impression of change (PGIC).
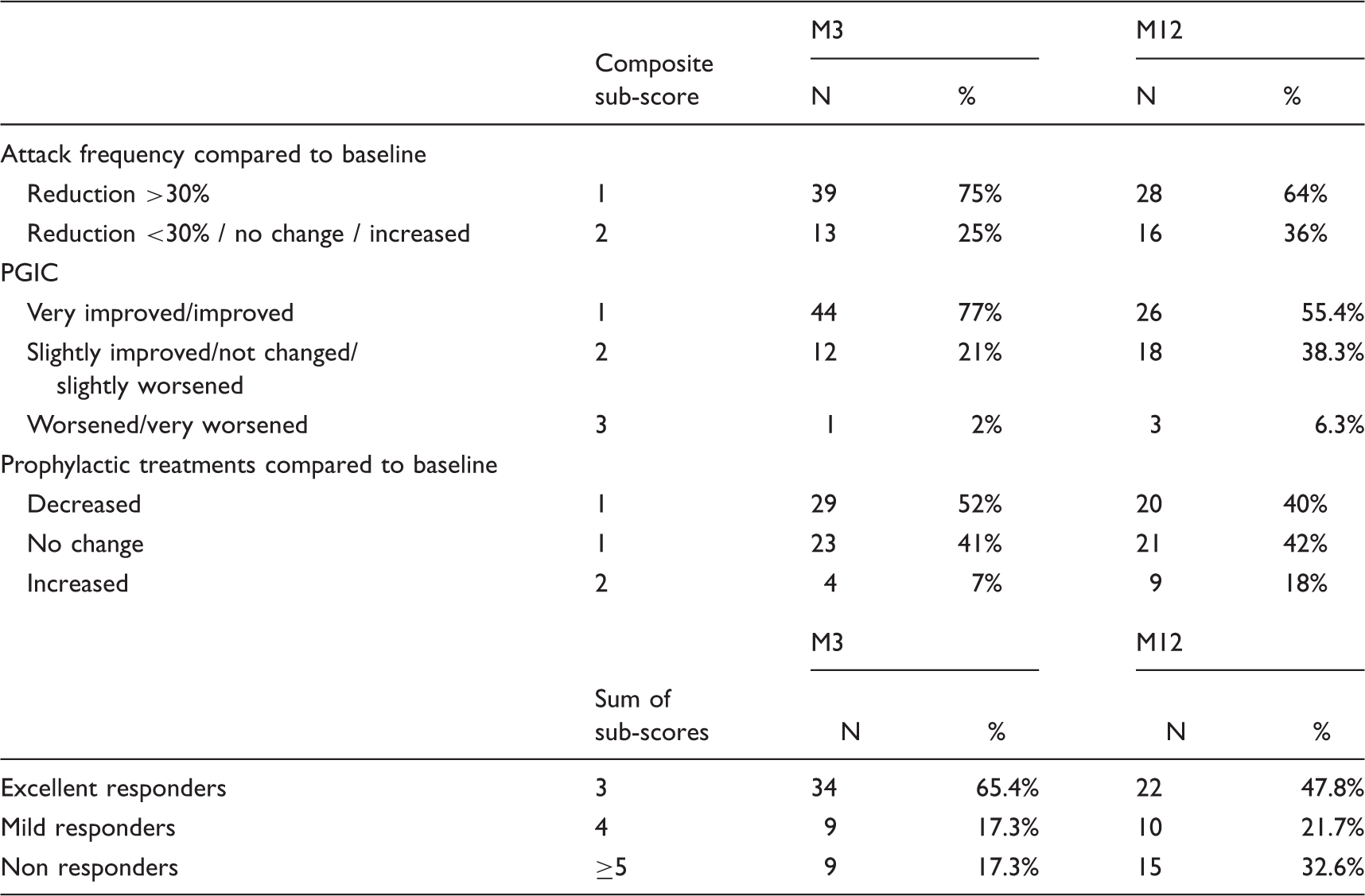
Global outcome of rCCH patients treated by ONS after three and 12 months. Classification of patients into excellent, mild and non-responder groups used a composite score. This composite score considered three criteria: PGIC, reduction of attack frequency and prophylactic treatment changes. A sub-score ranging from 1 to 3 was attributed to each criterion. The final score (obtained by the sum of these sub-scores) allowed classification of the patients as excellent responders (score equal to 3), mild responders (score equal to 4) and non-responders (score equal to 5, 6 or 7).
Analysis of patients’ outcomes across the whole series after three and 12 months. *Wilcoxon signed rank test.

Statistical analysis
Results are presented as means (SD) for quantitative variables and relative frequencies for categorical variables. The score comparisons between baseline and visits (M3, M12) were performed using the Wilcoxon signed rank test. This analysis was repeated according to composite score group (excellent responders, mild responders, non-responders) and according to centres’ surgical experience (experienced centres with >10 inclusions, and less experienced centres). Analysis at M12 was repeated in “intention-to-treat” by using the LOCF (last observation carried forward) method. All tests were two-sided and the significance level was set at 5%. Statistical analyses were performed using SAS Enterprise Guide 5.1 (Copyright (c) 1999-2006 by SAS Institute Inc., Cary, NC, USA).
Results
Sixty-seven patients fulfilled the inclusion criteria. Due to partially missing data, 58 patients were analysed for safety, 52 and 44 could be analysed for the primary efficacy endpoint at M3 and M12 respectively (see flow chart in Figure 1). An additional two patients were explanted before M12 due to lack of efficacy and were considered as non-responders. The mean age was 43.1 years (range 23–70). Mean disease duration and attack frequency at baseline (n = 57) were respectively 6.8 years and 21.63 (± 16.86) attacks per week.
Flowchart of the observational study.
Efficacy
Three months after ONS, 75% of the patients had experienced a significant decrease of CH attack frequency (Table 1). At M12, the reduction of attack frequency was >30% in 64% and >50% in 59% of patients. Most significantly improved, and prophylactic treatments could be decreased in 40%, although this improvement declined at M12 compared to M3. About 69.5% of the patients responded to ONS (Table 1), 47.8% being excellent responders. At M12, 15 patients (including the two explanted patients) were considered as non-responders. Ten out of these non-responders never experienced any degree of improvement after ONS. Five patients considered as non responders at M12 were actually not optimally stimulated at the time of evaluation for technical reasons (battery depletion, hardware dysfunction, etc.), but had experienced some degree of improvement earlier or later.
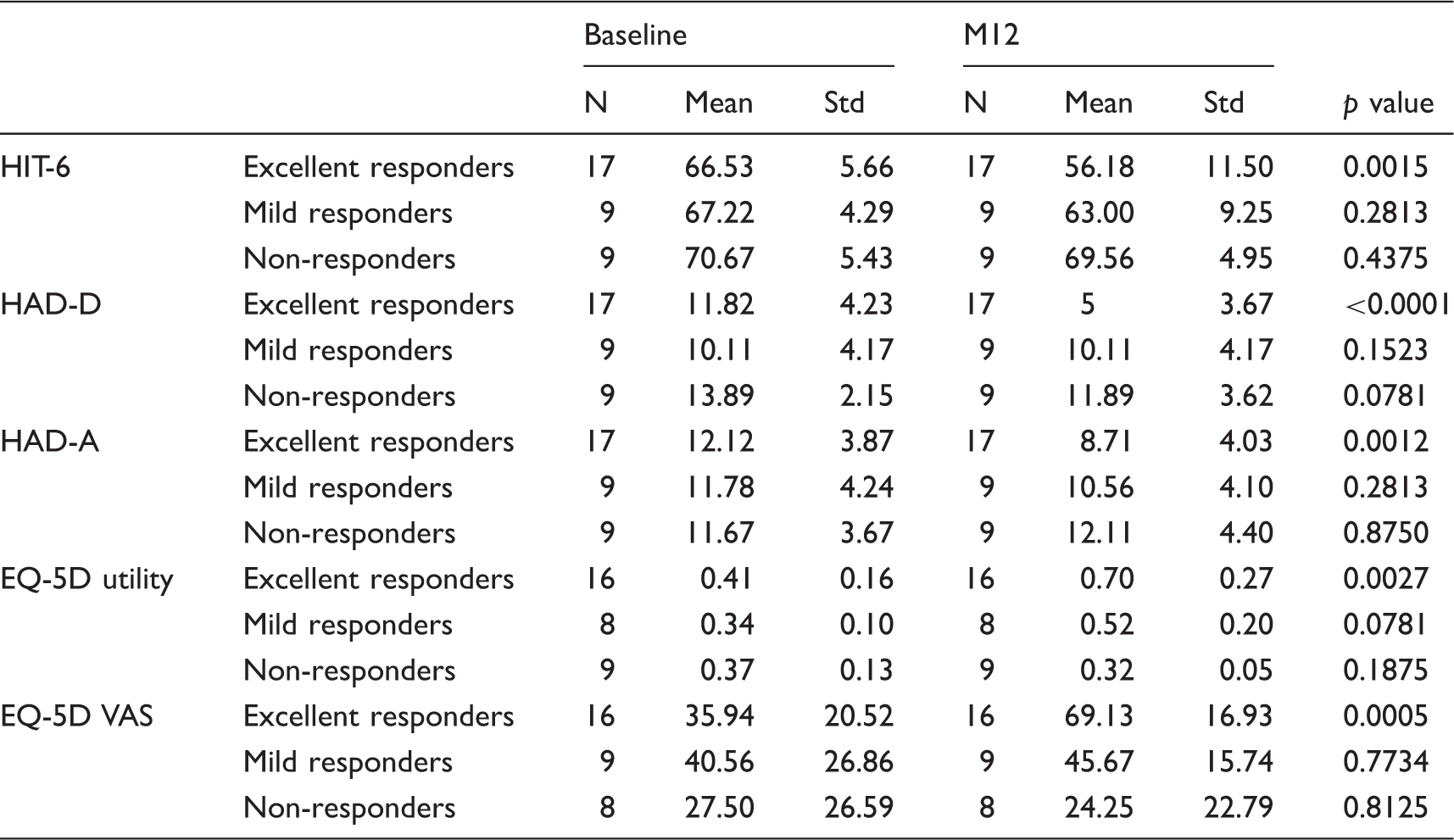
Mean attack frequency, intensity and duration were significantly reduced after ONS compared to baseline (Table 2). Consequently, the functional and emotional impacts of iCCH were significantly improved, as well as the health status (Table 2).
Analysis of ONS impact according to the quality of the patient’s response. *Wilcoxon signed rank test.
Two centres included more than 10 patients, one included eight patients and the other seven centres included one to four patients. We did not observed statistically different outcomes between more experienced and less experienced centres.
Complications
Nineteen out of 58 patients (33%) presented at least one surgical complication during the one-year follow up: hardware infection (1), wound issue (1), electrode migration (2), hardware-related discomfort (2), hardware/stimulation dysfunction (9) and early battery depletion (8) related to high energy consumption. Fifteen (26%) of these complications required an additional surgery, including eight battery replacements. Paresthesias induced by ONS were well tolerated in all the cases.
Discussion
In this cohort of iCCH patients, most of the patients responded to ONS and experienced a significant reduction of the cluster headache attack frequency. In excellent responders (48% of the cases), ONS induced a dramatic improvement of their health-related quality of life. These results are concordant with early and smaller series of iCCH patients treated by ONS (4,5,17–21), reporting that ONS acts as a prophylactic treatment by reducing the attack frequency in about 60–70% of the patients (2). Additionally, our study showed that ONS could also reduce the functional and emotional impacts of iCCH and could improve the health-related quality of life.
Although data were acquired prospectively, some data corresponding to M3 and M12 evaluations were missing in our database for several reasons inherent to such a multi-centric large observational network, reflecting real daily practice. These missing data might have led to an overestimation of the ONS responders’ rate if the nine patients lost were non-responders, but very unlikely that it would have modified the dramatic improvement observed in responders. On the other hand, in five patients, lack of improvement at M12 was very likely related to a transient ONS interruption due to battery depletion or hardware dysfunction. These patients were considered as non-responders although they experienced some degree of improvement later, after the technical issue was solved.
In contrast with previous studies that usually defined a response only as a reduction of attack frequency ≥50%, our definition of response additionally considered the prophylactic treatment, to ensure that improvement was not due to treatment changes. We also considered the PGIC scale as a patient-related outcome. Indeed, some patients did not experience such attack frequency reduction, but were nevertheless satisfied because the attack intensity or duration decreased, did not justify sumatriptan injection, or because a frequency reduction <50% was sufficient to improve their quality of life. We considered that a threshold of >30% reduction in attack frequency was sufficient to define a response in those patients, given the severity of their disease (mean preoperative EQ-5D VAS score was 38) and their previous resistance to any medical treatment. We observed a major improvement of the quality of life in patients who experienced a decrease >30% of their CH attacks, similar to those experiencing a decrease >50%. Moreover, similarly, a reduction >30% of the pain intensity numerical rating scale is accepted as sufficient to consider that an analgesic medication is efficient in primary care (22). Consequently we used a composite score that took into consideration the association of these three criteria and allowed the patients to be categorised in three groups: excellent responders, mild responders and non-responders.
Although this series of iCCH patients treated by ONS is one of the largest published to date, the number of patients studied remained small, due to the rarity of this situation. Cluster headache is an orphan disease. Chronic and medically intractable cluster headache is even infrequent. ONS has been used in this condition since 2007 in only a few centres, as a compassionate treatment, and is not currently reimbursed in our country. Moreover, as ONS induces the perception of paresthesias in the occipital region, its evaluation in blinded conditions appears difficult and a placebo effect cannot be ruled out. However this effect was probably low, because patients who did not feel the paresthesias any more, due to hardware dysfunction, often observed a recurrence of their attacks within the following days. The rarity of iCCH and these methodological difficulties probably explain why ONS efficacy has been studied in open trials only, as we did. However, a large randomised controlled trial is currently ongoing (23) and will probably clarify the therapeutic effect of ONS in iCCH more objectively.
The main sources of patients’ dissatisfaction came from the surgical complications. Although there was no mortality and no neurological deficit, 33% of the patients experienced complications, mainly hardware-related. This high rate of complications in our study may be explained by the learning curve of ONS, a relatively recent technique in most of the participating centres, and for which no consensus exists concerning the surgical aspects. Surgical experience, design of ONS-dedicated hardware and use of rechargeable batteries should decrease the risk of complications in the future. Surgical complications of ONS remain far less severe than those observed with deep brain stimulation (24–26), and we believe that ONS should be proposed before DBS in the surgical treatment of iCCH (27). The place of ONS relative to spheno-palatine ganglion stimulation remains debatable, considering that only few data are available for the latter (28).
Considering the severity of CCH in these medically refractory patients and its major impact on their quality of life, the dramatic improvement potentially induced by ONS justifies, in our opinion, the risks and cost (29) of this therapeutic approach. However, long-term evaluation on large series of patients will be necessary, considering that the long-term efficacy of ONS has recently been questioned (30).
Clinical implications
In this nationwide multidisciplinary observational study, 70% of intractable chronic cluster headache patients responded to occipital nerve stimulation, including 48% of excellent responders. Occipital nerve stimulation significantly reduced the attack frequency, the functional and emotional headache impacts and dramatically improved the health-related quality of life of responders. Surgical minor complications were observed in 33% of the patients. Considering the severity of the disease in these medically refractory patients and its major impact on their quality of life, the dramatic improvement potentially induced by occipital nerve stimulation justifies, in our opinion, the risks and cost of this therapeutic approach.
Footnotes
Acknowledgements
We thank Philippe Longchamp (CHU de Nancy) and Christophe Nuti (CHU de St Etienne) for their contributions.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D Fontaine and M Lanteri-Minet received consultant fees and research grants from Medtronic and St Jude Medical. S Chabardes has been a consultant for Medtronic and Boston Scientific. These three companies manufacture and commercialise neuromodulation devices that can be used for occipital nerve stimulation. Other authors have nothing to disclose.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was promoted and supported by the Centre Hospitalier Universitaire de Nice. St Jude Medical and Medtronic have financially partially supported the study, but had no role in the study design, data collection, analysis and reporting.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.