
Abstract
Aims: Migraine has a wide clinical spectrum. Our aim was to group information on migraine characteristics into meaningful components and to identify key components of the migraine phenotype.
Methods: We performed two principal component analyses, one among participants in the Women’s Health Study enrollment cohort and one in a sub-cohort with additional migraine-specific information.
Results: Among the 9427 women with migraine attack–related information at enrollment, the three most important components pertained to central nervous system (CNS) sensitization, attack frequency/pain location and aura/visual phenomena. In the subgroup of 1675 women with more detailed information, food triggers and unspecific symptoms constituted two principal components that explain more of the variance of the migraine phenotype than the three attack–related components.
Conclusions: Our results indicate that information on migraine-associated features, symptoms and triggers is highly correlated, allowing the extraction of principal components. Migraine attack–related symptoms are best summarized by symptoms related to CNS sensitization, attack frequency/pain location and aura/visual phenomena. Taking a more general view, unspecific symptoms and food triggers appear to carry stronger importance in characterizing the migraine phenotype. These components are useful for future research on the pathophysiology and genetics of migraine and may have implications for diagnosing and treating patients.
Introduction
Migraine is a common debilitating disorder with a complex and heterogeneous phenotype. It presents with recurrent headache attacks, associated symptoms of vegetative disturbance and hypersensitivity of various functional systems of the central nervous system (CNS) (1,2). Meticulous descriptions of patients with migraine can be found in the medical literature going back hundreds of years (3). However, there has also been long-standing controversy about obligatory characteristics for migraine (4). The International Classification of Headache Disorders (ICHD) from 1988 was among the most important achievements in this regard (5), and the revised version from 2004 is the current gold standard for headache diagnosis (4,6).
The ICHD-II focuses on attack-related features, including pain intensity, localization and characteristics as well as nausea/vomiting and photo- and phonophobia to diagnose migraine. However, in addition, more general phenomena are considered typical for migraine. These pertain, for example, to severity of migraine, such as age at onset, attack frequency, family history and presence of aura (1,7,8), but also to triggering factors, including foods, drugs and hormones (9–11).
Attempts to systematically group, summarize and prioritize this vast amount of information from attack-related features, unspecific symptoms and triggers have been sparse (12–14). However, categorizing this information into main groups (components) and identifying their importance in migraine would help to understand the complexity underlying migraine as well as to further clinical, epidemiological, and genetic research in migraine.
We attempted to identify such main groups by performing principal component analyses using migraine-related information from a large cohort of women participating in the Women’s Health Study (WHS). First, we analyzed attack-related features among women who reported migraine during the year prior to enrollment (“active migraine”, N = 9427). Then we additionally investigated unspecific migraine symptoms and triggers among a subgroup of women for whom we had more detailed information from a migraine-specific questionnaire (N = 1675) and compared the results.
Subjects and methods
Study population
The WHS was designed as a randomized, placebo-controlled trial to test the benefits and risks of low-dose aspirin and vitamin E in the primary prevention of cardiovascular disease (CVD) and cancer among apparently healthy women. The design, methods and results have been described in detail previously (15,16). Briefly, a total of 65,169 US female health professionals aged ≥ 45 years at baseline (between September 1992 and May 1995) without a history of CVD, cancer or other major illnesses were enrolled, of which 39,876 were randomized to active aspirin (100 mg on alternate days), active vitamin E (600 IU on alternate days), both active agents, or both placebos. All participants provided written informed consent and the Institutional Review Board of Brigham and Women’s Hospital approved the WHS. Baseline information was self-reported and collected by a mailed questionnaire, which asked about migraine, many cardiovascular risk factors and lifestyle variables.
Of the women enrolled, those who reported migraine attacks at least once per month during the previous year were sent a detailed migraine-specific questionnaire and asked if they were willing to participate in a migraine sub-study. This sub-study aimed to evaluate the role of low-dose aspirin in the prophylaxis of migraine (17). The time period between obtaining migraine information from the enrollment questionnaire and from the detailed migraine-specific questionnaire ranged from a few weeks to less than nine months.
Assessment of migraine and migraine-related information
Baseline questionnaire. Participants were asked on the baseline questionnaire: “Have you ever had migraine headaches?” and “In the past year, have you had migraine headaches?” From this information, we categorized women into “any history of migraine;” “active migraine,” which includes women with self-reported migraine during the past year; and “prior migraine,” which includes women who reported ever having had a migraine but none in the year prior to completing the questionnaire. Women with active migraine were asked further details about the migraine attack frequency (daily, weekly, monthly, every other month, less than six times per year), aura or any indication a migraine is coming (yes, no), unilateral pain location (yes, no), pulsating pain quality (yes, no), inhibition of daily activities (yes, no), nausea and/or vomiting (yes, no), sensitivity to light (yes, no), sensitivity to sound (yes, no), attack duration of 4–72 hours (yes, no) and aggravation by routine physical activity (yes, no). In a previous study of the WHS (18), we have shown good agreement of our migraine classification with modified 1988 International Headache Society (IHS) criteria for migraine (ICHD-I) (5). If a woman did not check the box regarding a migraine feature, we categorized this as “no”.
Migraine-specific questionnaire. The detailed migraine-specific questionnaire contained questions pertaining to migraine features/characteristics, migraine-related symptoms and migraine triggers. Women were asked about the following: age at migraine onset (<10 years, 11–20 years, 21–30 years, 31–50 years, >50 years); migraine attack frequency during past year (daily, weekly, every other week, monthly); migraine severity during past year (light, moderate, severe); migraine duration during past year (<4 hours, 4–24 hours, 25–48 hours, 49–72 hours, >72 hours); number of days unable to function due to migraines during past year (0 days, 1–12 days, 13–24 days, 25–36 days, 37–48 days, >48 days); location of migraine (unilateral or behind one eye, front of head, back of head, whole head); character of migraine (pounding, pulsating, crushing, sharp, aching, burning); frequency or severity of migraine related to menstrual cycle (yes, no).
History of migraine was asked for every blood relative (no, yes, don’t know, not applicable) and combined into a variable “family history of migraine” (yes, other).
Frequency (never, sometimes, always) of the following symptoms was asked: aura or any indication a migraine is coming; double vision; other visual symptoms; nausea/vomiting; sensitivity to light; sensitivity to sound; behavioral or personality changes; unusual food cravings; bloating or fluid retention; sensory symptoms (tingling, numbness); speech or language symptoms; dizziness or vertigo; unilateral weakness in face, arms or legs. For the analysis these variables were categorized as “yes” or “no”.
In addition, women were asked if migraine is triggered or made worse by: physical activity; red wine; white wine; other alcohol; coffee; tea; cola drinks; cheeses; chocolate; artificial sweeteners; cold cuts or preserved meats; monosodium glutamate; hormones (post-menopausal estrogens, oral contraceptives); anti-angina drugs and vasodilators. Answer categories were “no” and “yes”; those pertaining to food also included “don’t know”.
Based on information from this migraine-specific questionnaire, we have shown excellent agreement between self-reported migraine and ICHD-II–based migraine classification in the WHS (19). We created a missing indicator variable for missing values.
Statistics
We used descriptive statistics to describe migraine-related information among women reporting migraine and report percentages and numbers.
Principal component analysis
Principal component analysis is a technique based on matrix algebra to create summary components from a number of observed variables (20). This analysis approach is typically applied to data sets with a large number of variables and observations.
Principal component analysis uses a regression to select from a pool of variables a subset of variables that explain most of the variance among all observed variables in order to derive a first summary component. The first component accounts for the largest amount of variance among all observed variables. This is expressed by eigenvalues or by the proportion or percentage of the total variance. In the next step a new subset of the observed variables is selected that best accounts for the remaining variance to derive the second component. This process continues and the total number of components extracted equals the number of observed variables. However, only a small number of components accounts for most of the total variance in the data set. We retained principal components with eigenvalues > 1, that means only those that explain more variance than any of the individual variables. A final transformation (“factor rotation”) is used to demonstrate more clearly which individual variables contribute to each principal component.
We performed two principal component analyses. The first analysis was among women reporting active migraine on the baseline (enrollment) questionnaire. We entered all available variables pertaining to migraine attacks as listed above.
The second analysis was among the subgroup of women with migraine with available information from the migraine-specific questionnaire pertaining to migraine features/characteristics, migraine-associated symptoms and migraine triggers, as described above.
For each principal component retained we report two measures: the eigenvalues and the percentage of variance explained. The percentage of variance explained equals the eigenvalue divided by the number of variables. Furthermore, we report the factor pattern matrix after rotation (containing correlation coefficients of the observed variables and principal components) along with the communalities for each observed variable. Communality is the proportion of variance of an observed variable that is due to common factors or shared with other variables. We labeled each principal component according to the variables contributing most heavily to them.
We further investigated the stability of the retained principal components in each of the two data sets by determining the variance of the eigenvalues with a resampling technique. For this we repeatedly calculated eigenvalues using 90% of the data with replacement after each calculation. This was done ten times and we then calculated the mean and the standard deviation (SD) of the 10 sets of eigenvalues for each principal component.
All analyses were performed using SAS version 9.1 (SAS Institute, Cary, NC, USA).
Results
Analysis among women reporting active migraine on the baseline questionnaire
Migraine features among women with active migraine in the WHS (N = 9427)
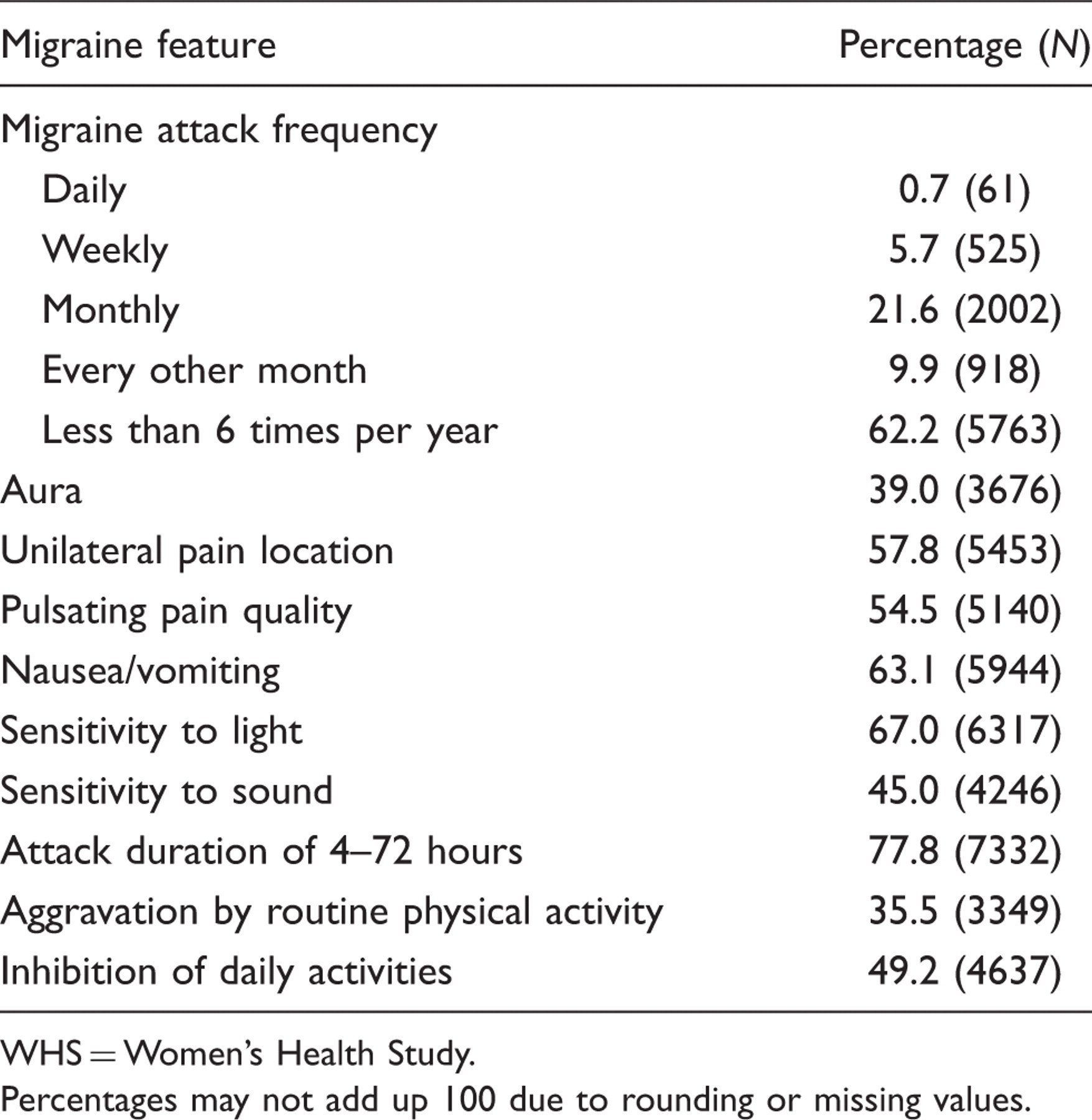
WHS = Women’s Health Study.
Percentages may not add up 100 due to rounding or missing values.
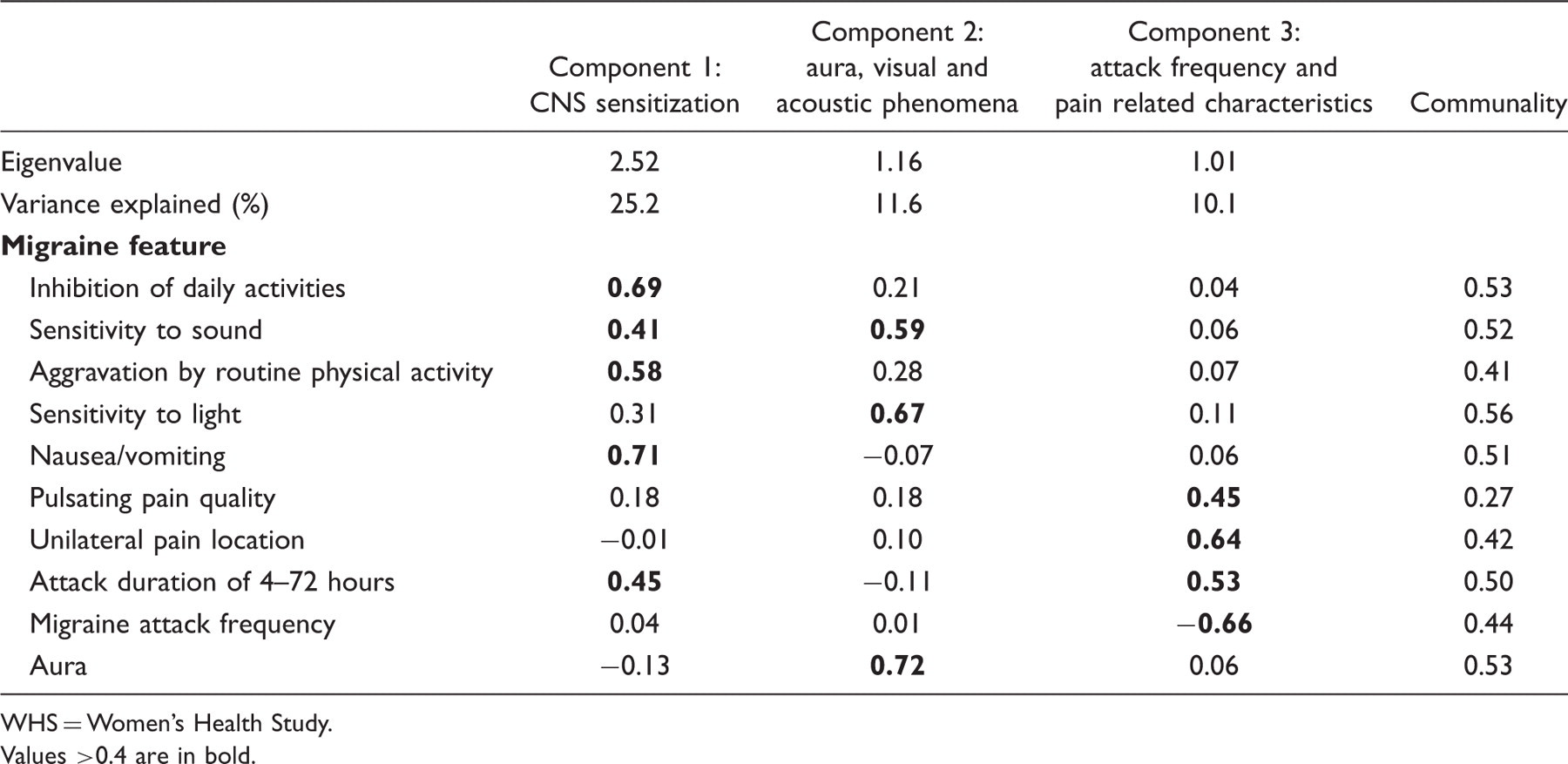
Eigenvalues and variance explained for principal components as well as factor loading after orthogonal rotation from principal component analysis of migraine features among women with active migraine in the WHS (N = 9427)

WHS = Women’s Health Study.
Values >0.4 are in bold.
Analysis among women with information from the migraine-specific questionnaire
Migraine features and other migraine characteristics among the subgroup of women participating in the WHS with information from the migraine-specific questionnaire (N = 1675)


WHS = Women’s Health Study.
Percentages may not add up 100 due to rounding or missing values.
Eigenvalues and variance explained for principal components as well as factor loading after orthogonal rotation from principal component analysis of migraine features/characteristics among the subgroup women participating in the WHS with information from the migraine-specific questionnaire (N = 1675)

WHS = Women’s Health Study.
Values >0.4 are in bold.
Component 6 largely overlaps with component 1 by combining variables for alcohol triggers with those for physical activity being a trigger and migraine duration. Component 7, which combines variables for migraine character, location and severity, conceptually overlaps with component 2, but explains much less of the variance. Component 8 is only characterized by anti-angina drugs/vasodilators and hormones being triggers and component 9 only by family history of migraine, hence explaining very little variance.
Sensitivity analysis
We also performed a principal component analysis among women participating in the sub-study restricted to information on migraine features from the baseline questionnaire. The results were stable and comparable to those obtained from among all women reporting migraine at baseline.
Eigenvalues and variance explained for principal components as well as factor loading after orthogonal rotation from principal component analysis of migraine features among women with active migraine in the WHS who participated in the sub-study
WHS = Women’s Health Study.
Values >0.4 are in bold.
Discussion
The main results from our analyses are that information regarding migraine attack-associated features, associated symptoms and triggers are highly correlated, allowing the extraction of summary variables (principal components). Specifically, analysis among women with information on migraine features allowed extraction of three principal components. In order of importance these pertain to CNS sensitization, attack frequency/pain location, and aura/visual phenomena. Furthermore, analysis among the subgroup of women with more detailed migraine information allowed extraction of five principal components. In order of importance these pertained to food triggers, unspecific symptoms, CNS sensitization, migraine severity and aura/visual phenomena. The principal components in both data sets appear to be reliable measures, as indicated by the small standard deviations of the eigenvalues.
Migraine is a phenotypically heterogeneous headache disorder. The consensus diagnostic criteria established by the IHS (6) are based on migraine features and constitute a snapshot of the most severe symptoms often occurring at the peak of an attack. However, many patients may only present a subset of or a mild form of features, precluding the diagnosis of migraine. The concept of “probable migraine” partly accounts for this heterogeneity (6).
A related concept that attempts to explain the phenotypical heterogeneity and complexity among primary headaches from a functional-anatomical perspective is the modular headache theory. According to this theory certain features of primary headaches can be ascribed to modules–groups of neurons that produce a feature or symptom of headache (12).
Our statistical approach supports the idea that migraine features can be grouped into main categories. Features of CNS sensitization, which are also emphasized in the IHS criteria for migraine, appear to be most important. However, our analyses also suggest that considering more general phenomena may yield additional information. We identified food triggers and unspecific symptoms as the two most important components in the subgroup of women, with additional information on the more general phenomena, explaining 21% and 12% of the total variance. We also identified components pertaining to CNS sensitization, migraine severity and aura/visual symptoms in this subgroup; however, they were less important than the more general phenomena.
When comparing the results of the two analyses, differences among the two groups of migraineurs have to be considered. The smaller group of migraineurs is a more severely affected subgroup of the larger one. For example, women in the subgroup all have attack frequencies of at least monthly and they have a higher prevalence of aura, other migraine related features, and attack frequencies from 4–72 hours. This may have the following implications. First, CNS sensitization, migraine severity and aura/visual phenomena are more general phenomena, which are important for all migraineurs. This is supported by robust results from our sensitivity analysis, indicating that among participants in the subgroup principal components with labels very similar to those in the whole cohort are retained. While features of CNS sensitization are most important in both groups, the importance of the second and third component has switched (Tables 2 and 5). This is not surprising when considering that for more severely affected migraineurs, like women in the sub-study, phenomena of hypersensitivity of the senses are often more compromising than the headache. Second, in addition to those three components, food triggers and unspecific symptoms may be more specific for more severely affected migraineurs. However, we could not verify this, because detailed information was unavailable for the whole group of migraineurs.
An interview-based physician diagnosis is considered the gold standard for the diagnosis of migraine. Although this is not feasible in large population-based studies, standardized epidemiologic tools have been successfully implemented in such studies. We have previously shown that in the WHS (18,19). Standardized questionnaires are ideal tools to systematically acquire a large amount of data, which can then be analyzed by data mining techniques like principal component analysis for underlying association patterns. Such an approach may be considered hypothesis generating in the sense that the new components may serve as surrogate outcomes in future studies aiming to decipher the epidemiological, physiological, or genetic basis as well as for drug treatment trials. Previous studies in migraine have used other data mining techniques to investigate certain phenotypic and genetic migraine features (13,14,21). For example, migraineurs were investigated with latent class analysis based on their symptoms according to IHS criteria (13,14). Using this technique, patients were classified into four phenotypic categories based on the severity of their symptoms, suggesting a continuum of the overall migraine phenotype. In contrast, our analysis aimed to identify main categories (principal components) among the many migraine features and characteristics that are most important in characterizing a migraine patient.
The strengths of our study include the large number of women with self-reported migraine both from the baseline and from the migraine-specific questionnaire as well as the detailed information regarding migraine features, migraine-associated symptoms and migraine triggers.
However, the following limitations should be considered. We cannot exclude potential misclassification of migraine and migraine features both based on the baseline questionnaire and on the migraine-specific questionnaire. We may have missed migraineurs who did not check the box on migraine on the baseline questionnaire. Likewise, women with other moderate-to-severe headaches may have checked the box on migraine. However, in a previous study (18), we have shown good agreement of our migraine classification with the 1988 IHS criteria for migraine (5) and we have shown excellent agreement between self-reported migraine and 2004 IHS criteria for migraine in the WHS sub-cohort (19).
In conclusion, our results indicate that much of the migraine-related information is correlated and support the concept that features indicating CNS sensitization constitute the most important component of individual attacks. However, on a more general basis, triggering factors and unspecific symptoms may be much more important for characterizing the migraine phenotype. The identified components are useful for targeted future research on the pathophysiology and genetics of migraine and may have implications with regard to diagnosing and treating patients.
Footnotes
Acknowledgements
We are indebted to the participants in the Women’s Health Study for their outstanding commitment and cooperation; to the entire Women’s Health Study staff for their expert and unfailing assistance.
Funding and support
The Women’s Health Study is supported by grants from the National Heart, Lung, and Blood Institute (HL-43851), the National Cancer Institute (CA-47988), and the National Institute of Neurological Disorders and Stroke (NS-34108). The funding agencies played no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review or approval of the manuscript.
Full disclosures for the last two years
Dr Schürks has received an investigator-initiated research grant from the Migraine Research Foundation. He has received honoraria from L.E.K. Consulting for telephone surveys and from the American Academy of Neurology for educational material.
Dr Buring has received investigator-initiated research funding and support as Principal Investigator from the US National Institutes of Health and research support for pills and/or packaging from Bayer Heath Care and the Natural Source Vitamin E Association. Dr Kurth has received investigator-initiated research funding from the French National Research Agency, the US National Institutes of Health, Merck, the Migraine Research Foundation and the Parkinson’s Disease Foundation. Further, he is a consultant to i3 Drug Safety and World Health Information Science Consultants, LLC; he has received honoraria from the American Academy of Neurology, Genzyme, Merck and Pfizer for educational lectures, and from MAP Pharmaceuticals for participating in a scientific advisory panel.
None of the disclosures for any of the authors represents a conflict of interest with regard to this specific manuscript.