
Abstract
Introduction: As research increasingly examines differences in headache characteristics between Caucasian and African American headache patients, it is requisite to determine the equivalence of existing headache measures for both racial groups.
Methods: This study examined the psychometric properties and measurement invariance of four widely used psychosocial headache measures. Caucasians (N = 173) and African Americans (N = 114) receiving treatment in four headache subspecialty clinics throughout Ohio completed the Headache Disability Inventory (HDI), the Migraine-Specific Quality of Life (MSQL) measure, the Headache Management Self-Efficacy (HMSE) scale, and the Headache-Specific Locus of Control (HSLC) scale prior to initiating new preventive therapies.
Conclusion: All measures demonstrated good internal consistency and measurement invariance. Despite adequate measurement invariance, the recommended factor structure of the HMSE scale yielded a poor fit for both African American and Caucasian patients. With perhaps the exception of the HMSE scale, the HDI, MSQL scale and HSLC scale are psychometrically sound and can be used with both Caucasian and African American headache patients.
Introduction
Approximately 3% of African Americans in the United States experience headaches on 180 or more days per year (1). A growing amount of research has compared African Americans and Caucasians with headache disorders. Although African Americans are less likely than Caucasians to be diagnosed with primary headache disorders, such as tension-type headache (TTH) and migraines, a higher prevalence rate of probable migraine (PM), a subtype of migraine that satisfies all but one criterion of a migraine diagnosis, has been found in African Americans compared to Caucasians (2). Among persons diagnosed with headache disorders, African Americans often report more frequent and severe headaches than Caucasians (3,4). Moreover, African Americans receiving care in headache subspecialty treatment clinics are twice as likely as Caucasians to terminate their clinic-based headache treatment before treatments are administered in their entirety (5).
Identifying and understanding race-related differences in headache patients is complicated by the fact that: (i) very few headache studies focus exclusively on ethnic minority groups; and (ii) the psychometric properties of multi-item headache measures are rarely evaluated by racial/ethnic group. Many psychosocial measures currently used in headache research, such as the Migraine-Specific Quality of Life (MSQL) scale (6), the Headache Disability Inventory (HDI) (7), and the Headache Management Self-Efficacy (HMSE) scale (8) were constructed 10 to 20 years ago using samples comprised almost exclusively of Caucasians. The psychometric properties and racial equivalence of commonly used headache measures have, for all intents and purposes, never been evaluated by patient race/ethnicity.
To date, efforts to develop equivalent headache measures have been limited to translating English-based measures for use in non–English speaking countries. This research has translated existing headache measures from English to French (9), English to Japanese (10), English to Danish (11) and English to German (12). However, while language translation is necessary when developing an equivalent measure for use with a different linguistic group, different cultures may interpret key constructs of a measure in conceptually different manners. Furthermore, little—if any—research has examined the validity and equivalence of headache measures between racial/ethnic groups within the same country (e.g. African Americans and Caucasians in the United States). This is problematic because terms that are used commonly in health-related research (e.g. self-efficacy, quality of life, locus of control) may have many different meanings between different racial/ethnic groups, even within the same country (13–15).
Responses to behavioral measures in health-related research often differ by race. For example, when completing self-report measures that assess behavior frequency or intensity, many African Americans engage in “telescoping” (i.e. believing that recent behaviors occurred more frequently than they actually did) (16); underreport health-injurious behaviors (e.g. high-risk sexual and substance use behaviors) (17); and overreport health-promoting behaviors (e.g. engaging in cancer screenings) (18). While other research finds that many behavioral measures apply equally well to African Americans and Caucasians (19), race-related biases and errors in self-reports that have been observed may threaten the psychometric integrity of many self-report behavioral measures and lead to erroneous conclusions regarding race differences (or the lack thereof) in important health behaviors (20).
The extent to which race-related reporting biases and errors that threaten the psychometric integrity of behavioral measures generalize to psychosocial measures (e.g. quality of life, locus of control) is unclear. Research has typically found relatively few differences between African Americans and Caucasians with headache disorders (21). It is unclear, however, if Caucasians and African Americans with headaches are truly comparable in headache characteristics or if psychometric limitations of these measures prevent the identification of race-related differences in this population.
This study examined the psychometric attributes and measurement invariance (MI) of the HDI (7), the MSQL scale (6), the HMSE scale (22) and the HSLC scale (23). MI is the extent to which scales have the same conceptual meaning across groups, a prerequisite to conducting between-group comparisons. Using data provided by patients in headache subspecialty treatment clinics, this study examined the psychometric adequacy of these measures by examining and comparing between races each measure’s internal consistency and, for two of the four measures, convergent validity. Multi-group confirmatory factor analyses assessed the scales’ MI in Caucasian and African American headache patients. Given the inconsistent findings from research examining the racial validity of measures in general, and the complete lack of research on this topic in headache patients, this study did not test any formal hypotheses. Instead, this research was exploratory in nature and tested whether widely used psychosocial headache measures applied equally well to African American and Caucasian headache patients.
Methods
Study procedures
Between July 2004 and June 2008, 311 patients were recruited in four headache subspecialty treatment centers in Columbus (N = 120), Toledo (N = 108), Cleveland (N = 68), and Cincinnati (N = 15), all cities in the US state of Ohio. Study inclusion criteria were: (i) 18 years of age or older; (ii) satisfying International Headache Society (IHS) criteria for episodic migraine, chronic migraine, episodic TTH, chronic TTH or medication overuse headache; (iii) a determination by the physician that the patient should begin new preventive medication therapy; and (iv) provision of informed consent. This study focused only on the 287 participants who self-identified as African American (N = 114) or Caucasian (N = 173). The primary objective of this project’s parent study was to determine how patient race was related to headache characteristics, adherence to headache treatment protocols and treatment outcomes. This psychometric analysis of widely used psychosocial headache measures is a secondary study of the larger parent project.
Recruitment materials (i.e. brochures and posters) that described the study were distributed to participating clinics for display and distribution to patients. While patients were recruited by site physicians and nurses during the patient’s initial clinic visit, only the physician determined patient eligibility. Because persons of color were relatively underrepresented in all four treatment centers, all racial minority patients who presented for treatment were approached for study enrollment. The larger pool of Caucasian patients enabled the project to use a recruitment strategy in which only every fifth Caucasian patient was approached for study enrollment. Eligible patients who volunteered for the study provided written informed consent in the treatment clinic after being treated by the physician. Patients were initially assessed at pre-treatment and re-assessed at three follow-ups (see Figure 1). The parent study’s methodology is described elsewhere in greater detail (24,25). The study was approved by the university’s Institutional Review Board, and no adverse events were reported during the project.
Study assessment and treatment schedule. PT, preventive therapy.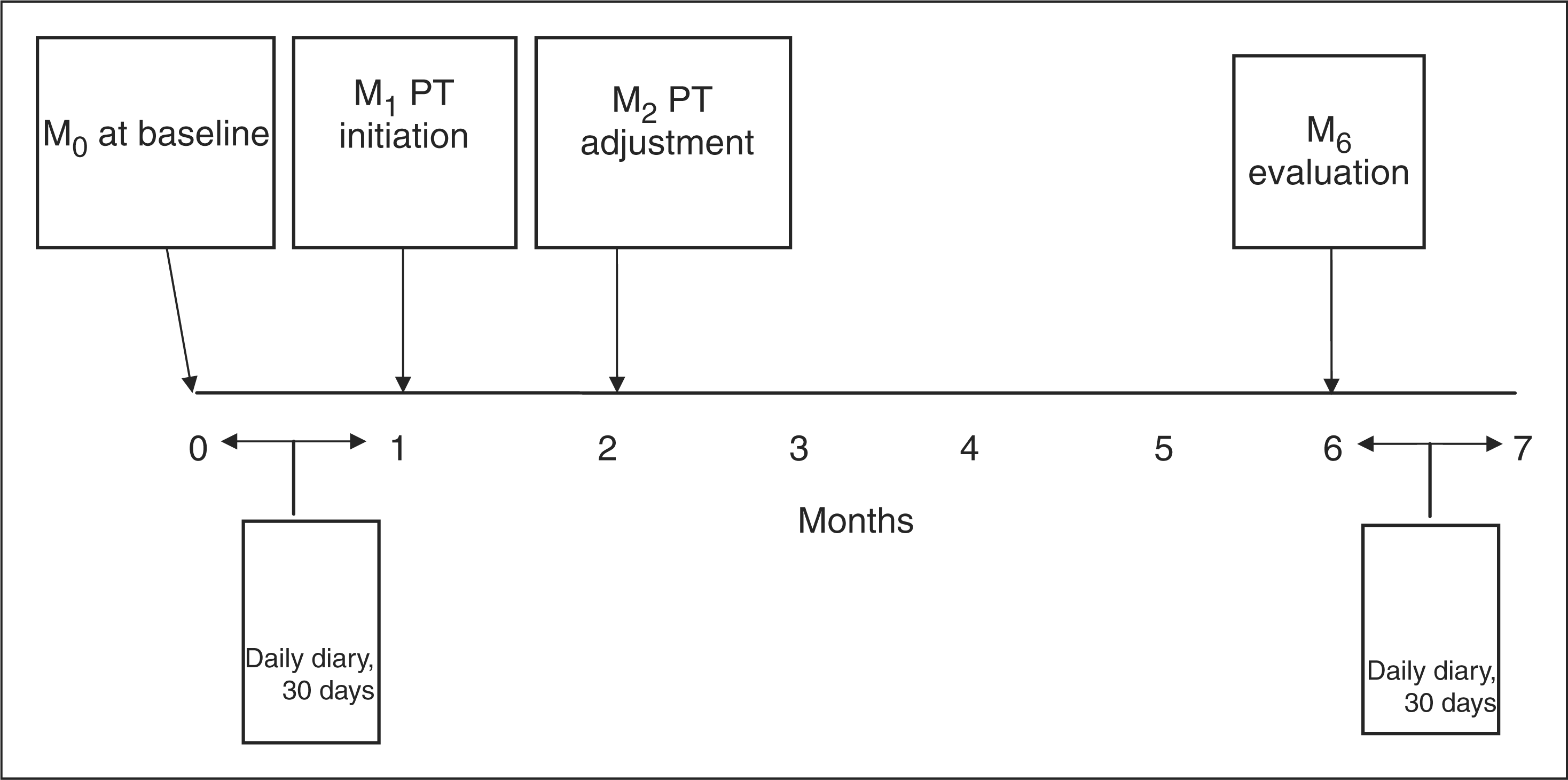
Assessment methodologies
This study collected data using four different methodologies: (i) face-to-face headache diagnoses; (ii) telephone-based assessments of psychiatric comorbidity; (iii) 30-day daily diaries (for headache frequency, severity and disability); and (iv) self-report surveys completed by patients during each of their four clinic visits. Each methodology is described below in greater detail. The psychometric properties of study measures were evaluated using data provided by patients during their baseline (M0) visit.
Headache diagnosis. During the initial patient-physician interaction, the physician diagnosed each patient’s current headache disorder(s) using IHS criteria (26). The physician also documented each patient’s past and current pharmacological headache treatments.
Psychiatric disorder diagnosis. Psychiatric disorders were diagnosed using the Primary Care Evaluation for Mental Disorders (PRIME-MD) (27). The PRIME-MD was administered to all patients enrolled in the study by trained research staff during a telephone interview conducted within two days after the patient completed his or her pre-treatment visit. The PRIME-MD was used because it was designed specifically for use in primary care settings and yields a subset of diagnoses included in the Diagnostic and Statistical Manual of Mental Disorders, including mood and anxiety disorders, alcohol and substance (abuse/dependence), eating disorders and somatoform disorders.
30-Day daily diary. During the interval between the pre-treatment and one-month follow-up visit, patients completed self-administered, paper-and-pencil daily diaries in which they recorded the frequency, severity and disability of headaches experienced during the 30 day assessment period. Headache frequency was the “number of days over the 30-day period during which patients experienced a ‘mild,’ ‘moderate’ or ‘severe’ headache.” Headache severity was assessed for each headache using a 4-point scale (0 = no pain, 1 = mild pain, 2 = moderate pain, 3 = no disability, 1 = mild disability, 2 = moderate disability, 3 = severe disability).
Self-administered surveys. Patients also completed self-administered surveys at the headache treatment clinics during their initial treatment visit. Measures assessed through self-administered surveys are described below:
Headache Disability Inventory (7). The 25-item HDI assessed the perceived impact of headaches on one’s emotional and functional well-being. The HDI comprised two subscales: (i) Emotional-Related Disability (13 items: e.g. “My headaches make me angry”); and (ii) Functional-Related Disability (12 items: e.g. “I do not enjoy social activities because of my headaches”). Higher scores indicated greater overall, emotional and functional disability due to one’s headaches.
Headache-Specific Locus of Control Scale (23). The 33-item HSLC scale measures patients’ beliefs regarding factors that control their headaches. The HSLC scale contained three subscales that assessed patients’ beliefs that their headaches were controlled by their own efforts (Internal subscale, 11 items), chance circumstances (Chance subscale, 11 items) or health care professionals (Health Care Professional subscale, 11 items). Respondents rated the extent to which they agreed with each item using a 5-point scale (1 = “strongly disagree” to 5 = “strongly agree”).
Headache Management Self-Efficacy Scale (8). The 25-item HMSE scale measured patients’ perceived confidence that they could engage in various behavioral strategies to prevent headache episodes or manage headache-related pain and disability. Sample items included: “There are things I can do to prevent headaches,” “Once I have a headache, there is nothing I can do to control it” and “I can prevent headaches by changing how I respond to stress.” Patients rated the extent to which they agreed with each item using a seven-point scale (1 = “strongly disagree” to 7 = “strongly agree”).
Migraine Specific Quality of Life Scale (6). A 14-item adapted version of the MSQL assessed the impact of headache disorders on patients’ quality of life. Because the original MSQL items referred only to migraines, the term “migraine” was replaced with the more general term “headache” when relevant. For example, the original MSQL item “In the past 4 weeks, how often have migraines interfered with how well you dealt with family, friends and others close to you” was changed to “In the past 4 weeks, how often have your headaches interfered with how well you dealt with family, friends and others close to you” (emphasis added). The MSQL scale comprised three subscales: (i) Role Restriction (7 items: e.g. “How often have headaches left you too tired to do work or daily activities?”); (ii) Role Prevention (4 items: e.g. “How often were you not able to go to social activities such as parties and dinner with friends because of your headaches?”); and (iii) Emotional Functioning (3 items: e.g. “How often have you felt fed up or frustrated because of your headaches?”). The overall scale and the three subscales were scored so that lower scores indicated better quality of life.
Demographics. As part of the 30-day diary, patients indicated the racial group with which they most identified, their age, gender, number of years of education, current employment (full-time, part-time, unemployed), type of health insurance coverage (e.g. health maintenance organization, preferred provider, private, government-sponsored) and annual income.
Data analytic procedures
Coefficient alpha was calculated for each measure by race to assess its internal consistency. The convergent validity of the HDI and MSQL scale was assessed by calculating the Pearson Product Moment correlation coefficient between these two scales and measures that were assessed through different methodologies but that, theoretically, should have correlated with the multi-item measures. Finally, robust maximum-likelihood estimation multigroup confirmatory factor analyses (CFA) were used to test the equivalence of the MSQL scale, the HDI, the HMSE scale and the HSLC scale in African American and Caucasian samples. Multigroup CFAs were conducted using LISREL 8.54 (28). Because the amount of missing data was minimal (<5%), missing values were not imputed; analyses were conducted using only those cases that contained complete data. Test-retest reliability coefficients were not calculated for study measures because the changes and/or adjustments in medications administered at the M0 baseline visit (e.g. changes in acute therapies and/or previously prescribed preventive therapies) may have altered patients’ headache activity between the M0 and M1 treatment visits and reduced each measure’s test-retest reliability.
Results
Participant characteristics and headache treatments at baseline
The average patient was 36.5 years of age, female (88%) and had completed 14.0 years of education. The modal headache diagnosis was episodic migraine (with or without aura). The average patient experienced 17.3 headache days per month and had been living with headaches for 7.9 years (standard deviation [SD] = 9.9 years, median = 4.0 years). Acute medications being taken by patients at their M0 baseline visit (and prior to the initiation of new preventive headache therapies) included triptans (34%), ergotamine/antiemetic (21%) and simple/compound analgesics (15%). Preventive therapies being taken by patients at their M0 baseline visit were vitamins (16%), anticonvulsants (9%), other antidepressants (7.4%) tricyclic antidepressants (6%), and beta blockers (4%).
Baseline differences between Caucasians and African Americans
Sociodemographic and clinical characteristics of Caucasian and African American patients; mean (SD)

SD, standard deviation; USD, US dollars. *Based on data obtained through daily diaries completed after patient’s initial appointment.
Coefficient alpha of headache measures by race
Psychometric attributes of headache-specific measures by race

HDI, headache disability inventory. ***p < .001. **p < .01. *p < .05. #Higher scores indicate poorer quality of life.
Convergent validity of HDI and MSQL by race
Table 2 shows the results of analyses assessing the convergent validity of the HDI and the MSQL scale by race. The 25-item HDI completed using the study’s self-report survey correlated significantly with headache disability scores assessed via 30-day self-report daily diaries in both Caucasians, r(121) = .38, p < .001 and African Americans, r(57) = .48, p < .001. These correlations did not differ significantly (z = 0.75, p = 0.46). The correlation between the MSQL scale completed using a self-report survey and headache severity assessed through 30-day daily diaries in Caucasian patients, r(123) = .28 was essentially identical to the correlation between the two measures in African American patients, r(62) = .27 (z = 0.07, p = 0.95).
Analyses of measurement invariance
Robust maximum-likelihood estimation multi-group confirmatory factor analyses tested the equivalence of the MSQL scale, the HDI, the HMSE scale and the HSLC scale between African American and Caucasian samples. This method computed a Satorra-Bentler (scaled chi square) (SB χ2) and robust standard errors that adjusted for multivariate kurtosis (29). The absolute fit of the measurement model was evaluated using the SB χ2, with a preference for models with a SB χ2 to degrees of freedom ratio of ≤2 (30). Because the traditional chi-square statistic as a test of absolute fit is sensitive to sample size (31), the Comparative Fit Index (CFI) was used. CFI values range from 0 to 1, with values ≥ .90 and ≥ .95 representing adequate and excellent model fit, respectively (32,33). The Root Mean Square Error of Approximation (RMSEA) (34) statistic was supplied as an indication of the population error variance (35). Interpretation of RMSEA values in terms of fit were as follows: good (<0.05), acceptable (0.05–0.08), marginal (0.08–0.10), and poor (>0.10) (35–37). For differences between nested models, the SB χ2 difference test was used (38).
MI analyses determined if the same factor structures provided an adequate fit for both African American and Caucasian samples by testing models that had increasingly restrictive and hierarchical constraints. More specifically: Model 1, Configural Invariance, tested the measurement model in which the factor pattern (pattern of factor loadings) was equal between groups; Model 2, Weak Factorial Invariance, added equal factor loadings to the constraint of equal factor pattern; Model 3, Strong Factorial Invariance, added equal intercepts; Model 4, Strict Factorial Invariance, tested equal factors loadings, intercepts, and error variances; and Model 5, Strict Factorial Invariance, added equal factor variances. If the constraints placed on the factor structures resulted in a worse model fit (as evidenced by a significant increase in the SB χ2 difference test) (38), the model was not considered to meet that particular level of invariance.
MSQL scale goodness of fit model statistics for multi-group confirmatory factor analyses
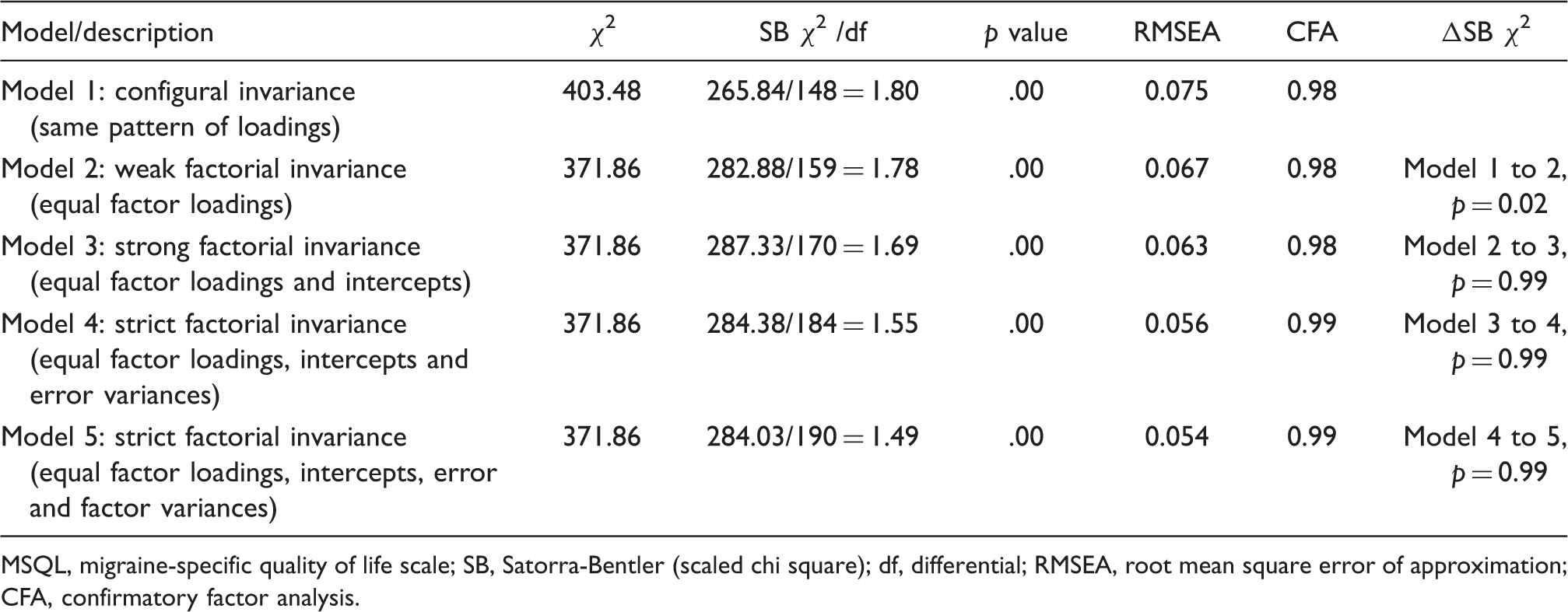
MSQL, migraine-specific quality of life scale; SB, Satorra-Bentler (scaled chi square); df, differential; RMSEA, root mean square error of approximation; CFA, confirmatory factor analysis.
Factor structure of the MSQL for Caucasians and African Americans
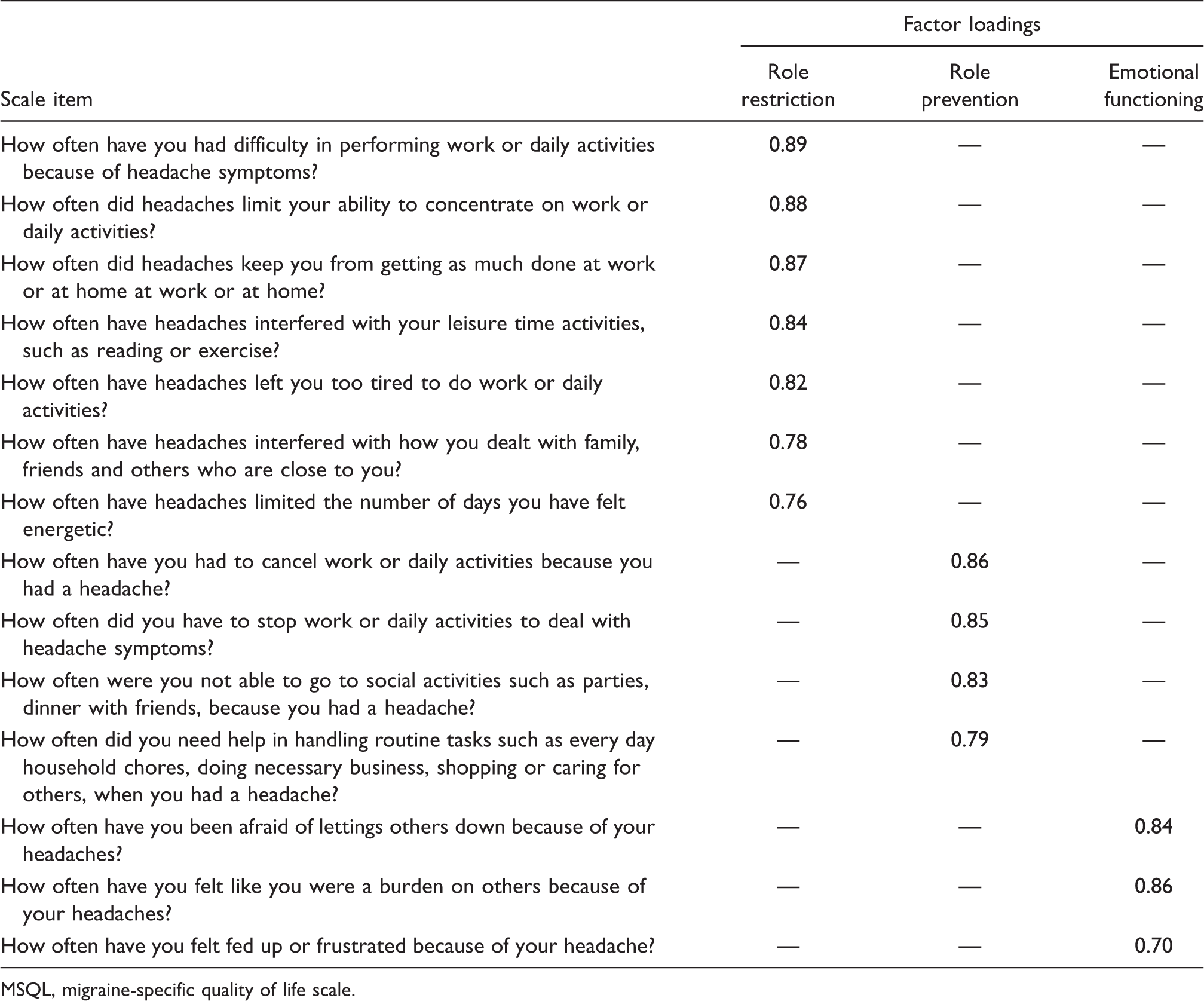
MSQL, migraine-specific quality of life scale.
HDI goodness of fit model statistics for multi-group confirmatory factor analyses

HDI, headache disability inventory; SB, Satorra-Bentler (scaled chi square); df, differential; RMSEA, root mean square error of approximation; CFA, confirmatory factor analysis.
Factor structure of the HDI for Caucasians and African Americans

HDI, headache disability inventory.
HMSE scale goodness of fit model statistics for multi-group confirmatory factor analyses

HMSE, headache management self-efficacy scale; SB, Satorra-Bentler (scaled chi square); df, differential; RMSEA, root mean square error of approximation; CFA, confirmatory factor analysis.
Factor structure of the HMSE scale for Caucasians and African Americans

HMSE, headache management self-efficacy scale.
HSLC goodness of fit model statistics for multi-group confirmatory factor analyses

HSLC, headache-specific locus of control scale; SB, Satorra-Bentler (scaled chi square); df, differential; RMSEA, root mean square error of approximation; CFA, confirmatory factor analysis.
Factor structure of the HSLC scale for Caucasians and African Americans
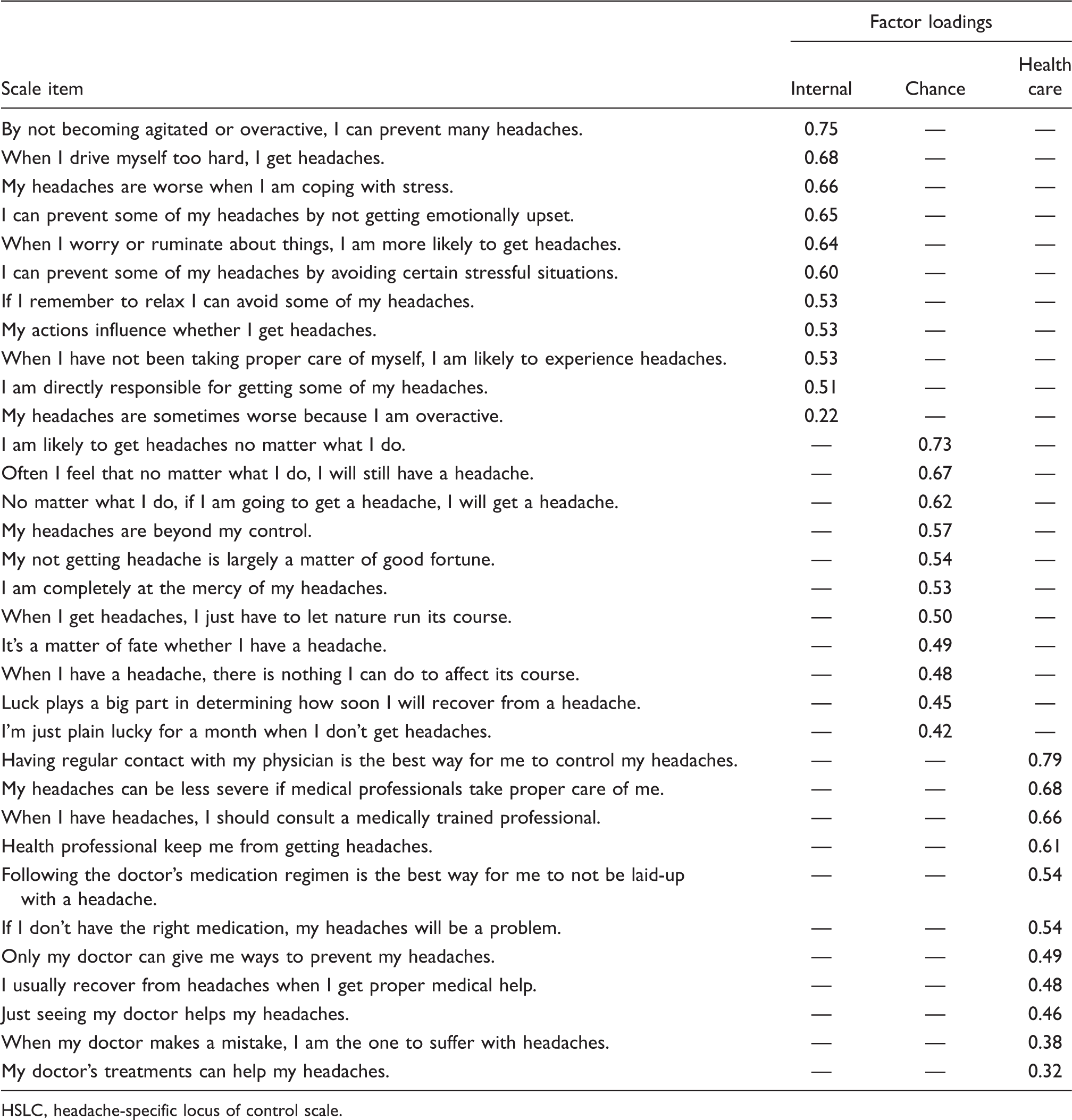
HSLC, headache-specific locus of control scale.
Discussion
As researchers investigate potential race differences in persons with headache disorders, a critical prerequisite is the establishment of MI of the multi-item headache measures used to detect these differences. Currently, it is assumed that psychosocial headache measures apply equally well to headache patients of different racial groups. This research tested this assumption by assessing the MI of widely used psychosocial headache measures in Caucasian and African American headache patients.
The psychosocial headache measures assessed in this study evinced good internal consistency for both Caucasian and African American headache patients. Coefficient alpha for the psychosocial measures always exceeded 0.80 for both groups, a criterion commonly used to demonstrate adequate internal consistency (39). Two widely used psychosocial headache measures (i.e. the HDI and the MSQL scale) demonstrated good convergent validity. Specifically, the self-report HDI correlated significantly with headache disability assessed through 30-day daily diaries while the self-report MSQL scale correlated significantly with headache severity recorded via 30-day daily diaries in both racial groups. These findings should increase researchers’ confidence in headache patients’ abilities to provide accurate data about their headache disability and quality of life assessed through more global measures that use longer retrospective recall periods.
MI was established for the HDI, the MSQL scale, and the HSLC scale. This suggests that these measures apply equally well to Caucasian and African American headache patients and that race-related differences observed on these measures are, in all likelihood, identifying actual between-group differences that are not the result of measurement artifacts.
While the HMSE scale evinced adequate MI, the measure’s established factor structure provided a poor fit for both Caucasians and African Americans as assessed by several indices (CFA ≤ .80, RMSEA ≥ .10; and SB χ2 /df ≥ 2.33). These findings suggest that while Caucasians and African Americans conceptualized self-efficacy similarly, the scale not be a particularly good assessment of headache management self-efficacy for either group. These results were somewhat unexpected given the scale’s high coefficient alpha in Caucasians (α = 85) and African Americans (α = .88). These findings also demonstrate why relying solely on a scale’s coefficient alpha is insufficient to substantiate its psychometric adequacy. Because the scale’s developers (8) speculated that the HMSE scale may contain two subscales (i.e. Headache Prevention and Headache Management subscales), the scale may have provided a better fit to data collected in the current study if two factors had been specified.
Future research should test if the HMSE scale is unidimensional, comprised of two or more subscales, or, alternatively, develop new measures of headache management self-efficacy. The poor fit of the scale in this study may have also been due to one or more characteristics of the sample (i.e. patients in participating subspecialty clinics reported very frequent and disabling headaches), the current study’s use of CFA as opposed to exploratory factor analyses (EFA), or other methodological factors of which we are unaware. A future measure of headache management self-efficacy might also be more psychometrically rigorous, and clinically meaningful, if it assesses self-efficacy in a specific domain (e.g. headache prevention self-efficacy, behavioral headache management self-efficacy).
This study has several limitations. All participating headache treatment centers were located in relatively large cities in Ohio; the extent to which study findings generalize to other geographic areas is unclear. The study’s sample had only adequate numbers of patients to assess the psychometric properties of study measures in Caucasian and African American headache patients. Future research should assess the psychometric attributes of these and other psychosocial headache measures with additional racial groups, such as Latinos/Latinas, Asian Americans/Pacific Islanders, and Native Americans.
Despite these limitations, this study adds to the existing headache literature by establishing MI between Caucasian and African American headache patients on several widely-used psychosocial headache measures. In both racial groups, the HDI, the HSLC scale, and the MSQL scale evidenced acceptable internal consistency, convergent validity, and MI, suggesting that these measures are likely to perform well for Caucasian and African American headache patients in cross-sectional research. Findings demonstrating MI between Caucasians and African Americans indicated that the two racial groups were using the same conceptual framework when completing these measures and that between-group comparisons on these measures are appropriate.
As headache researchers continue to examine potential race-related differences in headache characteristic in headache patients (or between-group differences on other variables such as gender, age and socioeconomic status), it will be increasingly important to consider carefully the psychometric attributes and MI of measures used in research of this type. As increasingly sophisticated data analytic methods become available to headache researchers (e.g. multi-group CFA), it is important that these approaches are integrated into their research to ensure that measures being used are assessing the constructs they purport to assess and to justify the conduct of between-group comparisons that are often the focus of contemporary headache research.
Footnotes
Acknowledgements
This research was supported by Grant K01 NS046582 from the National Institute of Neurological Disorders and Stroke (B. Heckman, P.I.).