
Abstract
Introduction: Bilateral transverse sinus stenosis (BTSS) has been reported to be associated with idiopathic intracranial hypertension without papilloedema in headache sufferers.
Subjects and methods: To test the accuracy of short-term cerebrospinal fluid (CSF) pressure monitoring through a lumbar needle for detection of elevated intracranial pressure in headache sufferers with BTSS, we prospectively performed lumbar puncture in order to measure lumbar CSF opening pressures and to monitor, for 1 h, the CSF pressure in 48 consecutive headache sufferers with BTSS and in 50 consecutive headache sufferers with normal appearance of transverse sinuses or stenosis of one transverse sinus.
Results: Of the 48 headache sufferers with BTSS, 18 (37.5%) had elevated CSF opening pressure and abnormal pressure waveforms, but short-term CSF pressure monitoring revealed abnormal pressure waves associated with elevated mean CSF pressure also in 26 (86.6%) out of 30 patients who had normal opening pressures. None of the 50 headache sufferers with normal appearance of transverse sinuses or stenosis of one transverse sinus had abnormal pressure waves and elevated CSF pressures.
Conclusions: In this study, short-term CSF pressure monitoring through a lumbar needle revealed abnormal pressure waves and elevated mean CSF pressures in the majority of headache sufferers with BTSS who had normal CSF opening pressures. These findings demonstrate the accuracy of short-term CSF pressure monitoring through a lumbar needle in estimating CSF pressure; they also highlight that a single-spot opening pressure measurement has a low accuracy for recognition of increased intracranial pressure in headache sufferers with BTSS.
Keywords
Introduction
Latterly, a growing body of evidence (1–6) has reported idiopathic intracranial hypertension (IIH) without papilloedema (IIHWOP) in headache sufferers. However, the clinical recognition of IIHWOP among headache sufferers cannot be reliably made, and patients with IIHWOP have often experienced extended delays in being diagnosed (7,8).
In everyday practice, the diagnosis of IIHWOP relies on the single-spot measurement of cerebrospinal fluid (CSF) opening pressure )9), but a single-spot lumbar measurement may lead to inconclusive CSF opening pressure recordings in headache sufferers with IIHWOP. A second lumbar puncture or prolonged (24 h) intracranial pressure monitoring through spinal drain may be necessary to document elevated intracranial pressure in patients with IIHWOP (9–11). However, even though the value of 24-h CSF pressure monitoring through lumbar drain is well recognised for establishing the diagnosis of IIH (12–14), the invasiveness of the procedure and other complications limit the diffusion of this diagnostic tool in clinical practice. Hence, there is a need for a minimally invasive diagnostic tool that can improve our ability to document elevated intracranial pressure in patients who are suspected of having IIHWOP.
More recently, several studies (5,6) have demonstrated bilateral transverse sinus stenosis (BTSS) in headache sufferers with IIHWOP; hence, BTSS is a predictor of IIHWOP in patients with migraine and chronic tension-type headache (CTTH). We hypothesized, therefore, that short-term CSF pressure monitoring through a lumbar needle could improve our ability of documenting elevated intracranial pressure in headache sufferers with BTSS. To address this question, we tested the accuracy of short-term CSF pressure monitoring for detection of elevated intracranial pressure in 48 consecutive headache sufferers with BTSS and in 50 headache sufferers without BTSS, who were candidates for diagnostic lumbar puncture.
Subjects and methods
Participants
Ninety-eight subjects were included in this prospective study: 50 patients with normal appearance of transverse sinuses (TSs) or unilateral TS stenosis and 48 patients with BTSS. Institutional Review Board approval was obtained for the study, and written informed consent was obtained from all the subjects.
Patients
Eighty-five women and 13 men (mean age, 43.5 years; SD 12.0 years) with chronic migraine (CM) and CTTH who had minimal response to treatment were consecutively enrolled from April 2005 until April 2009 among the patients admitted to the Institute of Neurology in Catanzaro. CM and CTTH were diagnosed according to the criteria established by the International Headache Society (IHS) (15). All patients were given the same standardised form to obtain headache, general medical (including body mass index: weight in kilograms divided by the square of height in metres), neurological and family histories. Interviews and neurological examinations were conducted on all patients by the same neurologists. Every eligible patient had a normal magnetic resonance (MR) scan of the brain and underwent a cerebral MR venography (MRV) before lumbar puncture (LP). All patients underwent LP in order to measure CSF opening pressure and to monitor CSF pressure for 1 h through a lumbar needle. The criteria for exclusion from the study were: (i) abnormal neurological examination; (ii) presence of papilloedema or MR evidence of structural brain lesions; or (iii) hydrocephalus. IIHWOP was diagnosed if the patient did not have papilloedema (confirmed by an ophthalmological consultation) and met the following diagnostic criteria for IIH: (i) symptoms of increased intracranial pressure; (ii) normal gadolinium-enhanced MR of the brain; (iii) documented elevated intracranial pressure; (iv) normal CSF contents; (v) no history of systemic disease or drug intake known to be associated with elevated intracranial pressure; and (vi) no evidence of current or prior cerebral venous thrombosis.
CSF pressure measurement
The same operator (FB) performed the LP on each patient. Pretreatment of patients was made with anxiolytics and local anaesthesia. In a puncture room, with the subject in the left lateral decubitus position, a standard 22-G (only occasionally 20-G) Quincke pointed spinal needle with a three-way stopcock was inserted. As soon as CSF appeared at the needle hub, the pressure transducer was attached to the hub of the needle via a 10-cm long flexible tube. The level of the transducer was in the same horizontal plane as the estimated level of the lumbar puncture needle in the subarachnoid space; the transducer was then zeroed. A pressure cable linked the transducer to the monitor (Passport 2, Datascope Corporation, Mahwah, NJ, USA). The patient was in a quiet resting state, the head and spine were strictly horizontal with the patient’s knees and hips in the extended position and neck straightened and a normal breathing pattern with the mouth open was ascertained throughout the recordings. At the beginning, opening pressure was recorded for 4 min to be certain that the pressure values had stabilised. Immediately after, CSF pressure was also monitored for a 60-min period to analyze the mean pressure, peak and highest pulse amplitude and abnormal pressure waveforms. Physician observation was continuous in order to analyze CSF pressure only during artefact-free epochs.
Image analysis
MR and MR venographies of the brain were performed on all subjects with a 1.5 T scanner (GE Medical Systems, Milwaukee, WI, USA). Brain MR consisted of sagittal T1- and transverse T2-weighted spin echo sequences with a slice thickness of 5 mm and an interslice gap of 1 mm. MR venography was performed using 3D-PC techniques as described elsewhere (16). All brain MR and MR venographies were analyzed by the same neuroradiologists who were blinded to each patient’s history. We classified the TS stenosis (TSS) as present or absent. TSS was considered present when the signal flow was poor or lacking (flow gap) in the mid-lateral portion of the transverse sinus (unilateral TSS) or in both transverse sinuses (BTSS).
Statistical analysis
For continuous variables, means of patient groups classified according to the chosen criteria were compared using the one-way ANOVA test or the unpaired t-test, as appropriate. Post-hoc comparisons were made using unpaired t-test corrected according to the Bonferroni method. For categorical variables, counts and percentages are reported. Differences in frequency distributions among groups were assessed using the chi-squared test. The paired t-test was used to evaluate the differences in means of pressure measurements inside each group. Statistical analysis was performed using the Statistical Package for Social Science software (SPSS, v17.0, Chicago, IL, USA) for Windows.
Results
The characteristics of the 98 headache sufferers are summarised in Table 1. Cerebral MR venography revealed normal appearance of TSs in 33 (33.6%) patients, but displayed stenosis in the mid-lateral portion of a single TS in 17 (17.3%) patients and stenosis of both TSs in 48 (48.9%) patients (Figure 1).
MR venography of the transverse sinuses, showing (A) normal appearance of the transverse sinuses and (B) flow gap in the mid-lateral portion of both transverse sinuses (arrow). Both coronal view. Characteristics and cerebrospinal fluid pressures in 98 headache sufferers CSF, cerebrospinal fluid; MRV, cerebral magnetic resonance venography; CM, chronic migraine; CTTH, chronic tension-type headache. Data are given as mean ± SD.
aUnpaired t-test; bchi-squared test. CSF opening pressure versus CSF mean pressure: P < 0.001 (all subjects); P = 0.008 (normal CSF pressure); P < 0.001 (elevated CSF pressure).

Of the 98 patients, 44 had abnormal pressure waves with mean pressures ranging from 210–444 mmH2O; the remaining 54 patients had both normal opening pressures and mean CSF pressures below 200 mmH2O (Table 1). According to CSF pressure findings, patients were divided into three groups (Table 2). Group 1 comprised 54 patients, each with both normal opening pressure (mean, 131.9 mmH2O; SD 26.0; range, 82–178 mmH2O) and normal mean CSF pressure (143.3 mmH2O; SD 31.8; range, 77–197 mmH2O; Figure 2). Group 2 comprised 26 patients, each with normal opening pressure (mean, 176.0 mmH2O; SD 15.9; range, 137–191 mmH2O) and elevated mean pressure (222.9 mmH2O; SD 13.1; range, 210–251 mmH2O) associated with abnormal pressure waves (Figure 3). Group 3 included 18 patients, each with both elevated CSF opening pressure (mean, 247.4 mmH2O; SD 31.7; range, 205–329 mmH2O) and elevated mean CSF pressure (mean, 270.3 mmH2O; SD 55.0; range, 210–444 mmH2O) associated with abnormal pressure waves (Figure 3). All patients in Group 2 and Group 3 displayed marked stenosis in the mid-lateral portion of both TSs, whereas 50 patients in Group 1 had normal MRV or unilateral TS stenosis.
Short-term CSF pressure monitoring through a lumbar needle. Group 3, elevated mean CSF pressures in 18 patients with bilateral transverse sinus stenosis (BTSS) and elevated opening pressures. Group 2, elevated mean pressures in 26 patients with BTSS and normal opening pressures. Group 1, normal mean pressures in 50 patients with normal appearance of the transverse sinuses or stenosis of one transverse sinus and normal opening pressures. Short-term CSF pressure monitoring through a lumbar needle. Abnormal pressure waves (arrow) associated with elevated mean CSF pressure in a patient with bilateral transverse sinus stenosis (BTSS) and opening pressure >200 mmH2O (A). Abnormal pressure waves (head arrow) associated with elevated mean CSF pressure in a patient with BTSS and CSF opening pressure <200 mmH2O (B). Fluctuations of normal CSF pressure in a patient with normal appearance of the transverse sinuses and opening pressure <200 mmH2O (C). Cerebral magnetic resonance venography findings in patients grouped according to cerebrospinal fluid pressure findings MRV, cerebral magnetic resonance venography; CSF, cerebrospinal fluid. Data are given as mean ± SD.
aOne-way ANOVA; bchi-squared test; c
P = 0.007 (Group 1 vs Group 2); d
P < 0.001 (Group 1 vs Group 2 and Group 1 vs Group 3); e
P < 0.001 (Group 2 vs Group 3). CSF opening pressure versus CSF mean pressure: P = 0.002 (Group 1); P < 0.001 (Group 2); P = 0.173 (Group 3).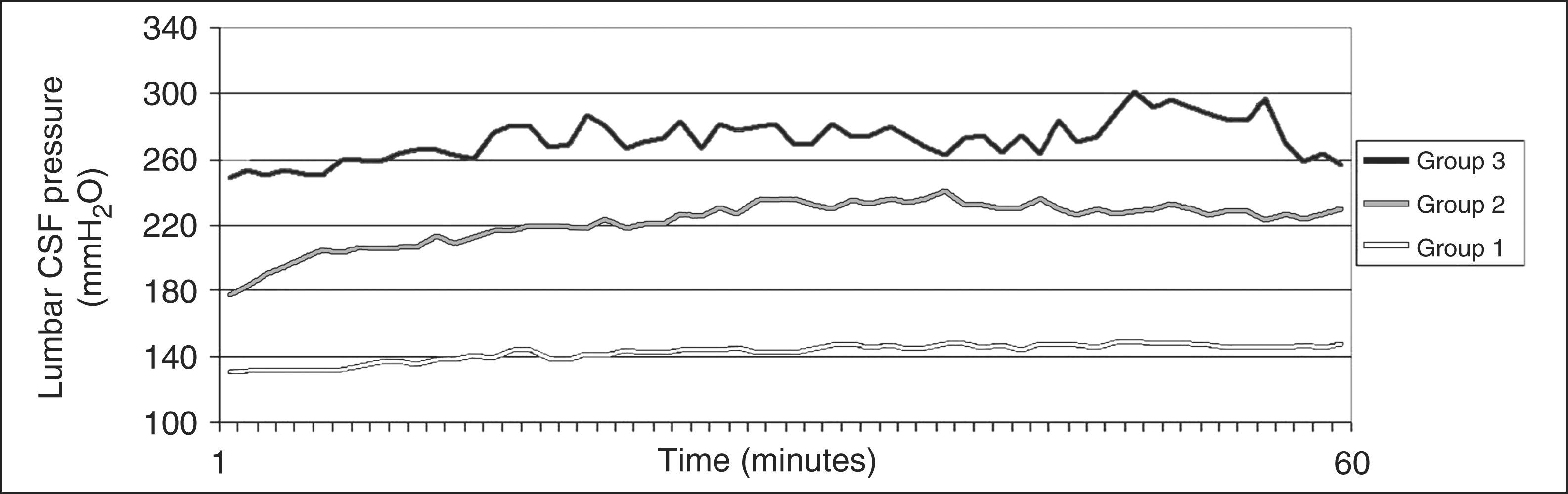

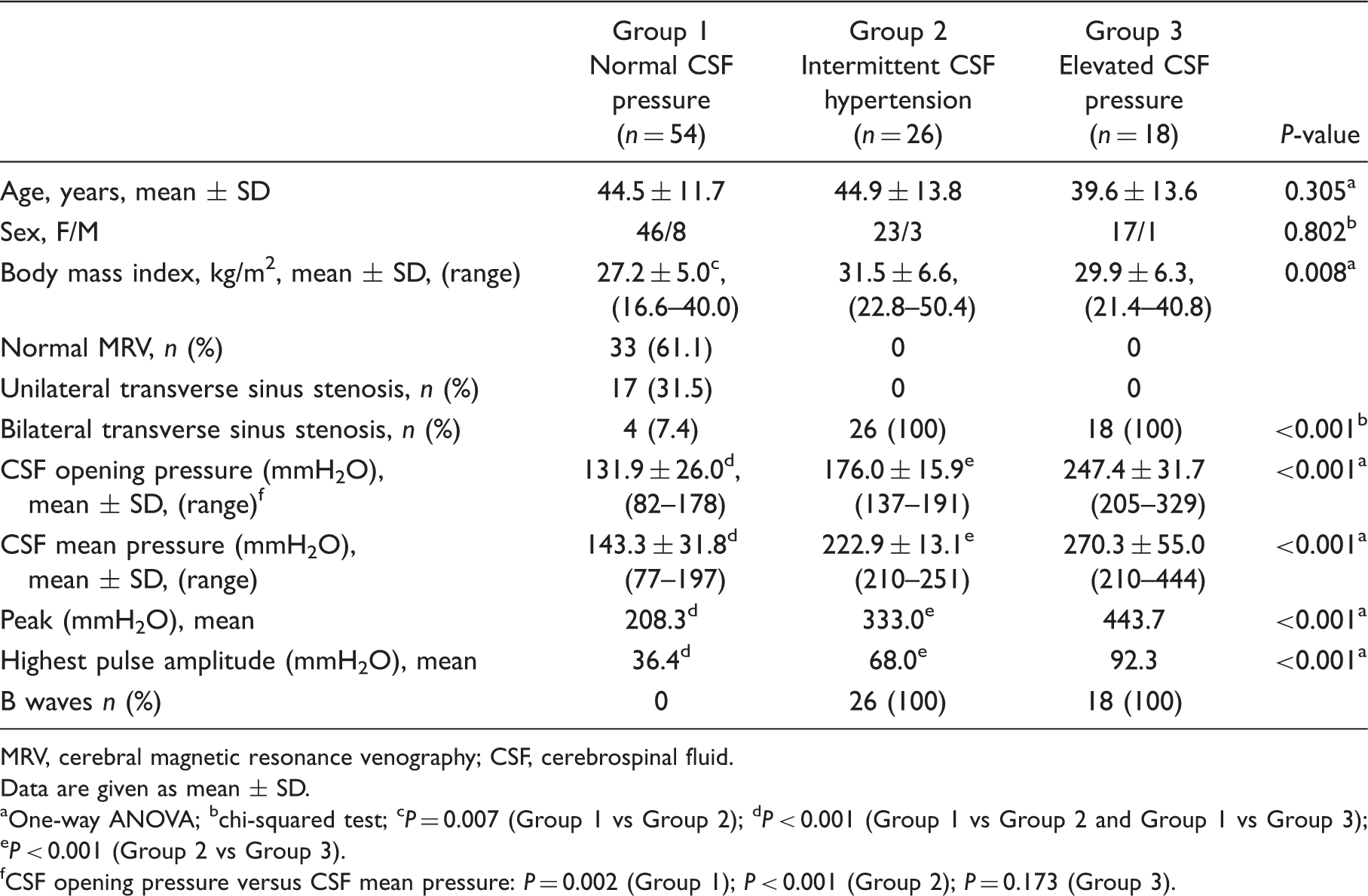
The headache profiles of patients with BTSS did not differ from those of patients with normal MR venographies or with unilateral TSS and normal CSF pressures, whereas the body mass index was significantly different among the groups (Table 2).
Of note, a transitory (2–4 weeks) improvement of headache intensity and frequency was observed after the LP in the majority of the patients with elevated intracranial pressure. We recommended an informal weight reduction diet programme in all obese patients and prescribed acetazolamide (500 mg/day) and topiramate (100 mg/day) simultaneously in the majority of patients with abnormal pressure waves. The response to medical treatment was good in most of these patients, while only a few patients showed minimal response. The ability of the patients to tolerate the medical treatment was satisfactory. During the follow-up, two of these patients underwent a second CSF pressure monitoring, and both had normal CSF pressures.
Discussion
In this study, short-term CSF pressure monitoring through a lumbar needle revealed abnormal pressure waves and elevated mean pressures in the majority of headache sufferers with BTSS who had normal opening pressures. These findings demonstrate the accuracy of short-term CSF pressure monitoring through a lumbar needle in estimating CSF pressure; they also highlight that a single-spot opening pressure measurement has a low accuracy for recognition of increased intracranial pressure in headache sufferers with BTSS.
It is interesting that, in our series of patients with abnormal pressure waves, all were headache sufferers with BTSS. BTSS is a condition that has been reported to be associated with increased intracranial pressure (17) in patients with chronic or recurrent headache (5,6). Hence, the presence of BTSS in our series of headache sufferers with abnormal pressure waveforms may be an explanation for abnormal fluctuations of CSF pressure in these patients. Indeed, increased pressure in the dural venous sinuses caused by obstruction of the TS, which in turn leads to increased intracranial pressure (18), could be the contributing factor involved in the pathogenesis of abnormal fluctuations of CSF pressure in our patients. This hypothesis is supported from manometry of the TS in patients with IIH (19), showing a substantial proximal-to-distal pressure gradient, and from reports of decrease of intracranial pressure following stenting of the TS in patients with IIH(20). Consistent with these findings, in our series of headache sufferers with normal appearance of TS and unilateral TS stenosis, all patients had normal CSF opening pressures and short-term CSF pressure monitoring did not reveal abnormal pressure waveforms. These latter findings demonstrate the lack of a disorder of intracranial pressure in these patients and are in agreement with the observations that patients with either normal appearance of TS (21–23) or unilateral TSS (23,24) on MRV had normal CSF opening pressures. Taken together, the above mentioned data support our finding that abnormal pressure waves were detected only in patients with BTSS.
In our series of headache sufferers, the results of the CSF pressure recordings indicated a significant difference between the values of opening pressures and the values of mean CSF pressures in about two-thirds of patients with BTSS. The discrepancy between the two methods of CSF pressure measurement may be explained by the abnormal fluctuations of CSF pressure in these patients. It is well recognised that CSF pressure may vary considerably with time (25,26). Moreover, abnormal fluctuations of CSF pressure have been demonstrated in patients with IIH (12–14). Furthermore, some authors (10) have reported that 24-h CSF pressure monitoring revealed abnormal pressure waves ranging from 22–40 mmHg in seven out of nine patients suspected of having IIHWOP; other authors (11) have also demonstrated the presence of normal resting CSF pressures associated with abnormal pressure waveforms during 24-h lumbar CSF pressure monitoring through a lumbar drain in a series of 10 headache sufferers suspected of having IIHWOP. These latter data support our finding that a single-spot measurement of opening pressure was less accurate than 1-h CSF pressure monitoring in estimating intracranial pressure in our series of headache sufferers with BTSS. On this basis, taking into consideration the presence of abnormal pressure waves and elevated mean pressures, the transitory improvement of headache after LP and the good response to pressure lowering treatment, we classified these patients as having secondary headache and mild IIHWOP. It is noteworthy that these patients would not have been identified if a short-term CSF pressure monitoring had not been performed on headache sufferers with BTTS. This latter observation supports our view that a careful investigation of headache sufferers is vital to make this diagnosis. Hence, the recognition of this condition requires a headache specialist and an expert neuroradiologist for selecting headache sufferers with BTSS who are candidates for short-term CSF pressure monitoring.
Finally, our investigation supports the hypothesis that the frequency of abnormal pressure waves among headache sufferers with BTSS may be greater than physicians realise, because there may be an error in excluding the recognition of this condition on the basis of a single-spot opening pressure measurement. In everyday practice, we suggest that headache sufferers with BTSS should be suspected of having a disorder of intracranial pressure, and they should have their CSF pressures analyzed by means of short-term CSF pressure monitoring through a lumbar needle.