
Abstract
Objective
To describe a new subtype of new daily persistent headache that is triggered by a single Valsalva event.
Methods
A case series of patients was evaluated in an academic headache clinic over a 3-year time period.
Results
A total of seven patients (four female and three male) were diagnosed with this new subtype of new daily persistent headache. The headaches all began after a single Valsalva event. Average age at time of headache onset was 41 years (males: 39 years; females: 43 years) with an age range of 20–62 years. All patients developed their syndrome during the months of September to February with November and February being the most cited months (5/7 patients). Immediate worsening in the Trendelenburg position occurred in all patients and appeared to be an almost diagnostic test for the syndrome. No patient had papilledema on funduscopic exam. Five out of seven patients had no prior headache history including cough, exercise or migraine. Four of seven patients were of normal weight, while one was overweight and two were obese. A crowded posterior fossa was identified in five of seven patients on brain MRI. On cerebrospinal fluid pressure/volume lowering medication (acetazolamide, indomethacin and/or spironolactone), five out of seven patients achieved 90% plus improvement in headache frequency while three patients became pain free. Three patients were able to taper off medication without headache recurrence.
Conclusion
New daily persistent headache after a single Valsalva event appears to be a unique subtype of new daily persistent headache that is responsive to cerebrospinal fluid pressure/volume lowering medications. An abnormal reset of cerebrospinal fluid pressure/intracranial pressure to an elevated state is the presumed pathogenesis and may relate to the patient's baseline neuroanatomy of a crowded posterior fossa. There appears to be a circadian periodicity to the onset of the syndrome. Worsening in the Trendelenburg position is a probable diagnostic test. Defining new daily persistent headache subtypes by triggering event appears to be making a positive inroad in the understanding of this condition and helps present new effective therapies.
Introduction
New daily persistent headache (NDPH) is a unique form of chronic daily headache. The pathogenesis of NDPH is currently unknown. This likely reflects the fact that NDPH is not one disorder but that of multiple disparate conditions that can all produce a daily headache from onset (1,2). It has been suggested that subgroups of patients with NDPH may have the same underlying etiology if they have the same triggering event (1). Recognized NDPH subtypes by triggering event include: Post infectious; post stressful life event; post-surgical procedure; post SSRI withdrawal; post vaccination, and post chemical exposure (1,3). The complexity of NDPH is that around 50% of sufferers cannot define a unique initiating event (1,3). The ultimate goal in studying NDPH should be to define distinct subtypes of the disorder and then decipher in that subtype if a unique pathogenesis exists and then develop a specific treatment based on that knowledge. A new subtype of NDPH will now be presented: That which is triggered by a single Valsalva event. Presumed etiology of the headache is an abnormal reset of cerebrospinal fluid (CSF) pressure to an elevated state. This patient population demonstrates a very positive treatment response to CSF pressure/volume lowering medications.
Methods
To describe a case series of patients with a distinct subtype of NDPH, occurring after a single Valsalva event. All patients were evaluated in an academic headache neurology clinic. All patients were assessed over a 3-year time period (2015–2017). All patients were either self-referred or physician referred for a complaint of headache. None of the patients had been given a previous diagnosis of NDPH. The study was given exempt status by the Mayo Clinic IRB. All patients gave consent to have their case presentations included in this study.
Statistical analysis
This is a descriptive case-series study only, so no statistical analysis was utilized.
Results
Patient characteristics.
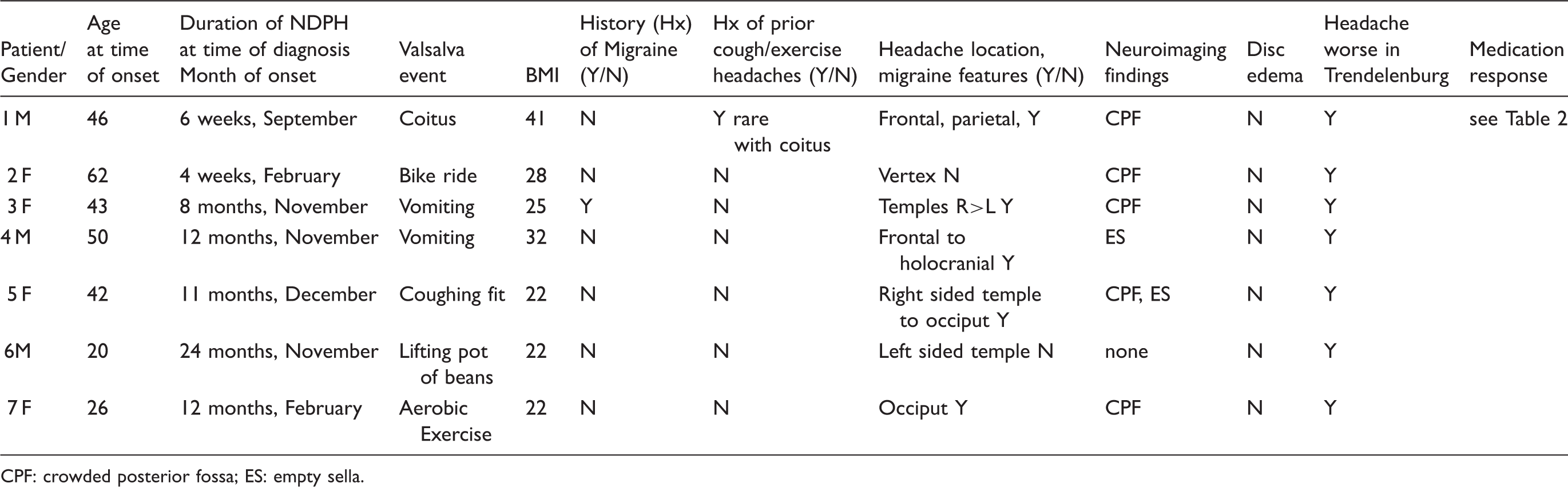
CPF: crowded posterior fossa; ES: empty sella.

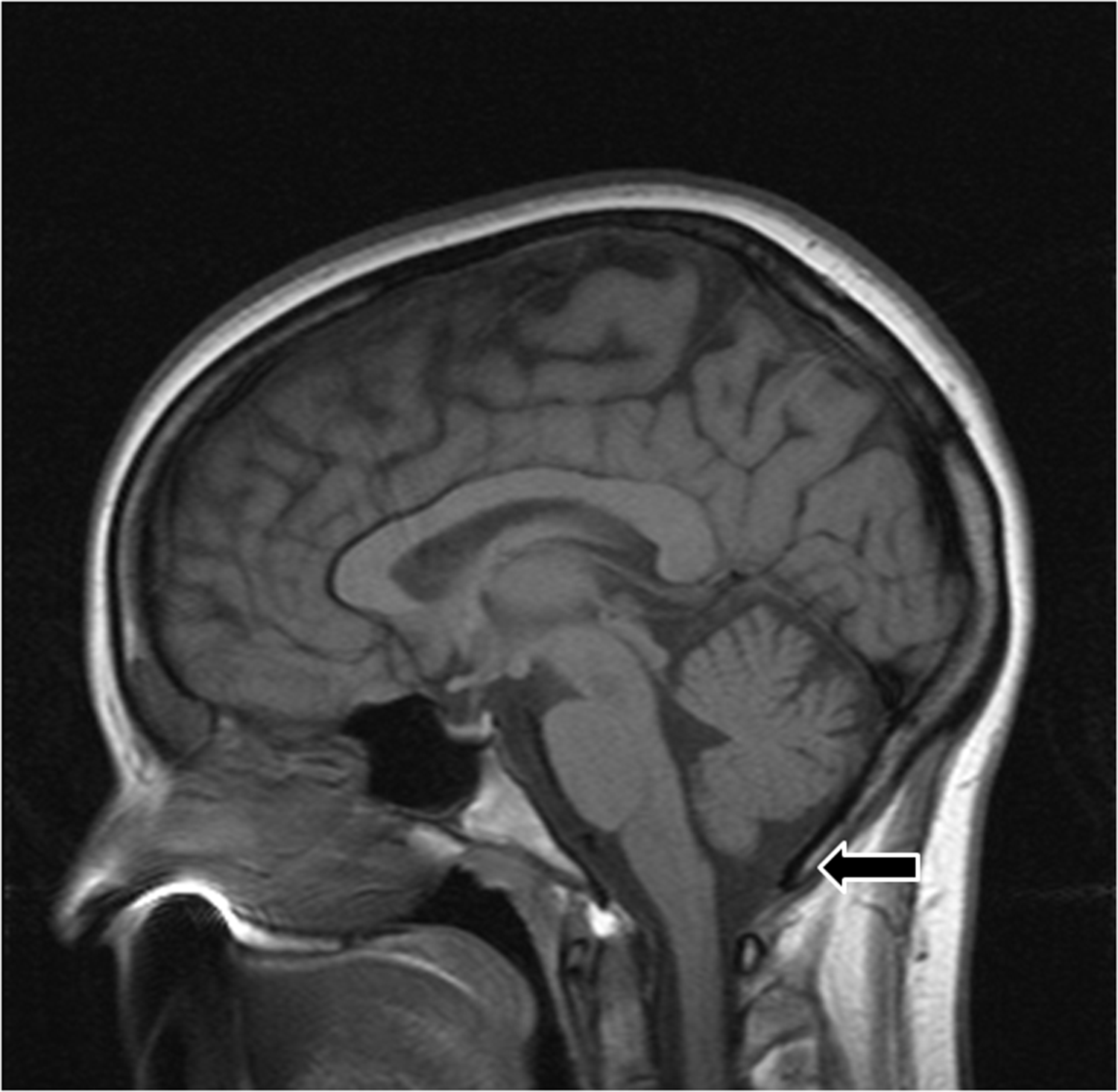
(Patient1): MRI Brain Sagittal T1 weighted image. Arrow is pointing to the crowded posterior fossa.

(Patient 2): MRI Brain Sagittal T1 weighted image. Arrow is pointing to the crowded posterior fossa.

(Patient 5): MRI Brain Sagittal T1 weighted image. Arrow is pointing to the crowded posterior fossa.

(Patient 7): MRI Brain Sagittal T1 weighted image. Arrow is pointing to the crowded posterior fossa.
Treatment response.

A representative case is presented to provide the clinical description and treatment response for this unique NDPH population.
Case presentation
Case 1 (Patient 1): A 46-year old man presented with a daily persistent headache after having coitus six weeks prior. Original headache began during sexual activity and was non-thunderclap at onset. Prior headache history consisted of several bouts of isolated short-lived headaches with sexual activity only. His past medical history was significant for obesity, obstructive sleep apnea (OSA) (compliant with C-PAP), tobacco use, hyperlipidemia and hypertension. Headache was best in the morning before arising and worsened during the day. He had some lightheadedness with it and only phonophobia as an associated migrainous symptom. The daily headache would worsen during any form of exertion including sexual activity. He had tried no preventive medication for headache and only over the counter NSAIDs as an abortive with minimal improvement. Neurologic examination was non-focal, including no disc edema on funduscopic examination. His headache immediately worsened in the Trendelenburg position (10 degree head down tilt). Neuroimaging including MRI brain, magnetic resonance angiogram (MRA) head and neck and MR venogram were read as normal (no aneurysm, dissection, vasospasm or signs of intracranial hypotension) although he appeared to have a crowded posterior fossa (Figure 1). The patient's daily headache at initial consult was considered to be NDPH but by time duration did not yet meet ICHD criteria (4). NDPH was later confirmed after repeat subsequent visits. The headache was hypothesized to be caused by a persistent elevation of CSF pressure based on his triggering event, neuroanatomy and worsening in Trendelenburg. Acetazolamide at 250 mg bid helped considerably but did not make him pain free. Eventually on a dose of 500 mg bid he became pain free and he was able to taper off medication without recurrence after several months of doing well on treatment. His daily pain lasted > 1 year before the correct dose of medication was found. Part of this was due to inconsistency of taking the medication.
Discussion
All presented patients met ICHD-3 beta criteria for NDPH (4). Those individuals who had their initial consult before the 3-month time prerequisite for ICHD diagnosis eventually met the criteria after subsequent visits. This unique subtype of NDPH is marked by the onset of daily head pain occurring immediately after or during a single Valsalva event. The Valsalva events were not unique for the patients, and while in some the event was more prolonged or more intense than a previous experience (excessive vomiting and uncontrolled fit of coughing for example), for others it was not. This form of NDPH appears to develop in individuals typically without a precedent headache history, specifically exercise, cough or migraine headache. The syndrome affects both genders and it can occur in athletes and non-athletes as one of the patients was a fitness instructor (Patient 7). It can affect individuals above or below the age of 40 years, thus it does not fit the typical age range for either primary exercise headache or primary cough headache, which are both Valsalva triggered head pain syndromes (4).
The author hypothesizes that this subtype of NDPH is potentially caused by an abnormal reset of the patients' CSF pressure/volume to an elevated state after a Valsalva event. The persistent CSF pressure elevation is presumed to be at a level that induces head pain but not papilledema. The hypothesis is that all individuals have their own unique range of CSF pressure/volume that they are acclimated to and anything that alters that range, even by minimal amounts, can induce headache. Presumably, if this alteration becomes fixed or static then persistent head pain will become the norm. An increase in CSF pressure with Valsalva maneuvers has been noted all the way back to the time of Quincke in the late 1800s (5). It appears that with a Valsalva maneuver, CSF pressure typically increases between 10–13mmHg in humans (5,6). A mild elevation in baseline CSF pressure as a cause of the presented patient's headaches was somewhat proven in the two patients who had lumbar punctures with normal opening pressures by recognized criteria and with both improving with CSF pressure/volume lowering medications. In addition, the fact that both developed post-LP headaches after typical CSF volume removal for analysis (8–10 cc of fluid) denotes a CSF pressure just above their baseline range as they easily went below their normal range with volume removal and developed headaches.
The question is, why daily persistent head pain after a single Valsalva event and not a short burst of resolving headache that is noted with cough headache or a several hour headache that then remits as appreciated with exercise-induced headache? A majority (6/8) of the presented patients had what the author terms a “crowded or tight posterior fossa” on brain MRI (Figures 1–4); thus, minimal space between the cerebellar tonsils and skull base. Figure 5 denotes a patient with pseudotumor cerebri but without a crowded posterior fossa for comparison. This neuroanatomic issue could potentially lead to NDPH after Valsalva by several mechanisms:
It predisposes the patient to persistent or intermittent obstruction of CSF flow, leading to an elevation of baseline CSF pressure levels near the headache-producing threshold and then after Valsalva, which raises CSF pressure further via intraabdominal and intrathoracic pressure changes transmitted to the cranial vault and via alterations of cerebral venous return, a headache is then generated because pain threshold levels are now reached. The “abnormal” neuroanatomy then maintains the elevated CSF pressure, producing a persistent daily headache. Thus, an abnormal reset to an elevated CSF pressure state that self sustains without the need of further triggering events. MRI Brain Sagittal T1 weighted image in a patient with known pseudotumor cerebri but without evidence of a crowded posterior fossa (arrow).
This same neuroanatomic issue has been noted in patients who develop cough headache (7). As most individuals do not develop an NDPH syndrome after a single Valsalva event, it would be assumed that even before the triggering event this patient population had a baseline elevation in their CSF pressure levels close to the headache-producing threshold point but not over it. Then the Valsalva pushes them over the threshold to produce headache, and their neuroanatomy does not allow them to reset back to their normal baseline. Could the cough and potentially exercise headache population present differently if their baseline CSF pressure levels are not as near the headache threshold level prior to the Valsalva event, and thus only a short-lived head pain is produced secondary to their neuroanatomy? No case patient had a Chiari malformation by criteria. No formal measurements were made to assess the posterior fossa area as was completed in the Chen et al. (7) investigation and thus posterior fossa “crowding” is an observation alone in the present case series. Worsening in the Trendelenburg position seems to be a consistent positive finding in this patient population and one that could help to solidify the hypothesis that the syndrome is caused by elevated CSF pressure (8–10).
If indeed a baseline elevation of CSF pressure is needed prior to Valsalva to produce this subtype of NDPH, another possible risk factor outside of the patients' neuroanatomy is an elevated BMI. Only two of our patients, however, were obese while four of seven were of normal weight. As both obese patients were older males (age > 45 years at headache onset), this could infer that for the male patients an elevated BMI, older age class and a crowded posterior fossa are the needed risk factors to develop post-Valsalva NDPH. In women, BMI does not appear to be a required risk factor.
Could time of year and/or time of day play a role in the syndrome? All of the presented patients appeared to develop their headache disorder from around the autumn clock change to near the spring clock change, suggesting a possible circadian-based threshold issue. It has been demonstrated that human CSF production exhibits a circadian pattern, as CSF pressure levels in the middle of the night are 2 to 3.5 times higher than that in the morning (11). Could time of year also influence this? Thus, if a patient with the correct neuroanatomy and/or elevated BMI then has a distinct exertional event during a specific time of year, and possibly time of day, could this form of NDPH develop?
Is this truly a new syndrome or a subform of an already recognized Valsalva-based primary headache disorder? This type of headache could be considered a prolonged variant of primary exercise headache, but it does not reach ICHD-3 criteria based on duration of head pain and lack of repetitive events (4). There may be some previous data alluding to a persistent interictal pain in patients with cough headache (12,13). Thus, is this a cough headache variant or did those patients with cough headache truly have NDPH post a single Valsalva event that would then exacerbate with coughing? Very recently, three female patients were reported who developed acute onset pseudotumor cerebri after a bout of coughing (14). All were below the age of 30 years, all obese, and all had dural vein stenosis on imaging. Their syndrome alleviated after initiation of acetazolamide combined with weight loss. The authors suggested a hydraulic theory for pseudotumor in which two steady states exist: A non-clinical state of low ICP and non-compressed dural venous sinuses and a pathologic state of high ICP and significant dural vein stenosis. Prolonged Valsalva, with its secondary impairment of cerebral venous return, could potentially trigger a switch in steady states to a self-sustained abnormal state with daily headache and disc edema. The hydraulic model as stated by the authors requires dynamic alterations in dural venous sinus diameter. The idea of having two steady states and the ability to create a self-sustaining pathologic steady state even after removal of the Valsalva trigger fits well with the presented abnormal CSF pressure reset theory. However, our female case patients were on average older, not obese and more importantly had normal venous imaging, suggesting a unique syndrome to the pseudotumor cerebri patients and possibly a different underlying pathology.
In regard to treatment, this particular subtype of NDPH appears to be very sensitive to medications that lower CSF pressure/volume and bucks the trend that NDPH is treatment refractory (Table 2). Acetazolamide was utilized in six of seven patients (Patient 4 had a contraindication) and five responded favorably, although two could not tolerate it long term secondary to side effects. Indomethacin alone was successful for Patient 2 (acetazolamide failure), while Patient 6 needed a combination therapy of spironolactone and indomethacin, and Patient 5 needed acetazolamide and indomethacin to feel better. Four out of seven patients no longer had daily head pain (three had complete resolution), while another patient was 90% improved but still had daily headache. Three patients were able to stop medication without headache recurrence. Two patients' treatment response was inconclusive either because of lack of long-term follow-up (Patient 3 only tried one medication) or intolerance/contraindication to effective medications (Patient 4). Based on this small case series alone, it appears that starting effective treatment earlier in the course of symptoms may predict complete pain resolution and the ability to stop medication without headache recurrence.
Limitations of this case series study include not having a true quantitative measurement of posterior fossa area, as was completed by Chen et al. (7) in their cough headache patients. Another limitation was not ruling out OSA in all patients, as this could raise baseline CSF pressure and be a risk factor for developing the syndrome (15). However, the one patient who had known OSA prior to NDPH onset actually developed the syndrome on CPAP treatment, thus OSA therapy was not protective against developing this subtype of NDPH. The limited number of case patients precludes the ability to make definitive statements about the clinical presentation of this NDPH subtype.
Conclusion
NDPH after a single Valsalva event appears to be a unique subtype of NDPH that is responsive to CSF pressure/volume lowering medications. An abnormal reset of CSF pressure to an elevated state is the presumed pathogenesis and may relate to the patient's baseline neuroanatomy of a crowded posterior fossa. There appears to be a circadian periodicity to the onset of the syndrome. Worsening in the Trendelenburg position is a probable diagnostic test. Defining NDPH subtypes by triggering event appears to be making a positive inroad in the understanding of this condition and helps present new effective therapies.
Footnotes
Key findings
Daily persistent headache after a single Valsalva event appears to be a unique subtype of NDPH.
This syndrome may develop because of an abnormal reset of CSF pressure/volume to an elevated state.
Medications that lower CSF pressure/volume appear to be effective at treating this distinct subtype of NDPH.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.