
Abstract
Background
Spontaneous intracranial hypotension is diagnosed by an abnormal finding in brain MRI, spinal imaging, or lumbar puncture. However, the sensitivity of each test is low. We investigated whether patients with suspected spontaneous intracranial hypotension and negative imaging findings would respond to epidural blood patch.
Methods
We prospectively recruited patients with new-onset orthostatic headache admitted at the Samsung Medical Center from January 2017 to July 2021. In patients without abnormal imaging findings and no history of prior epidural blood patch, treatment outcome—defined as both 50% response in maximal headache intensity and improvement of orthostatic component—was collected at discharge and three months after epidural blood patch.
Results
We included 21 treatment-naïve patients with orthostatic headache and negative brain and spinal imaging results who received epidural blood patch. After epidural blood patch (mean 1.3 times, range 1–3), 14 (66.7%) and 19 (90.5%) patients achieved both 50% response and improvement of orthostatic component at discharge and three months post-treatment, respectively. Additionally, complete remission was reported in 11 (52.4%) patients at three-month follow-up, while most of the remaining patients had only mild headaches. Among nine (42.9%) patients who underwent lumbar puncture, none had an abnormally low opening pressure (median 13.8 cm H2O, range 9.2–21.5).
Conclusion
Given the high responder rates of epidural blood patch in our study, empirical epidural blood patch should be considered to treat new-onset orthostatic headache, even when brain and spinal imaging are negative. The necessity of lumbar puncture is questionable considering the high response rate of epidural blood patch and low rate of “low pressure.”
Introduction
Spontaneous intracranial hypotension (SIH) is a disorder caused by cerebrospinal fluid (CSF) leak in the absence of a preceding procedure or penetrating trauma that cause dural tears. SIH can be provoked by minor trauma or vulnerabilities in the connective tissue (1,2). CSF leakage causes a loss of buoyancy of the brain resulting in a dislocation of the brain from the surrounding structures, resulting in pain and neurological symptoms (3,4). Orthostatic headache is a typical symptom of SIH, while the spectrum of SIH symptoms includes non-orthostatic headache, tinnitus, diplopia, nausea, vomiting, and even coma (5–8). With disease chronification, the clinical features can change, which can make the diagnosis and treatment of SIH difficult (9,10). Early diagnosis and management may help avoid chronification and neurological deterioration.
According to the International Classification of Headache Disorder-3 criteria, SIH can be diagnosed based on low CSF pressure (<60 mm CSF) or brain or spine imaging tests with evidence of CSF leakage (11,12). However, these diagnostic tests have inadequate sensitivity to reliably exclude SIH. Previous studies have not shown invariably high sensitivity for each test. Low CSF pressure has been reported in 34–93% of patients with SIH (4,13–19). Contrast-enhanced brain magnetic resonance imaging (MRI) showed abnormalities suggesting SIH in 29–100% of patients (13–29), while extradural CSF was documented in only 13–74% of computed tomography (CT) myelography and 38–100% of spinal MR (13,14,17–19,30–33). Considering that these findings are reported in patients with SIH defined by at least one abnormal finding from the three tests, the actual presence of abnormal diagnostic test findings may be considerably lower than previously reported. Furthermore, lumbar puncture may deteriorate the symptoms of SIH, as it can worsen CSF hypovolemia. Thus, the necessity for CSF pressure measurement is debatable (4,15).
Considering the pitfalls of diagnostic tests, we first conducted brain and spinal imaging for the initial diagnosis of SIH. If negative, an epidural blood patch (EBP) was performed in patients with suspected SIH without CSF pressure measurement, while only selected patients underwent lumbar puncture before EBP. Herein, we present the results of EBP treatment in patients with clinically suspected SIH but no imaging abnormalities.
Methods
Patient
We prospectively registered 191 patients admitted at the Samsung Medical Center due to suspected SIH between January 2017 and July 2021 in a prospective headache clinic registry. The suspicion of SIH was based on new-onset headache of an orthostatic nature, otherwise unexplained. Orthostatic headache was defined as any headache that worsens by sitting or standing and relieves after lying down. Patients who underwent lumbar puncture within one month prior to onset and those who had previously undergone EBP in other hospitals were excluded from this analysis. All patients provided written informed consent for the registry study, which included serial prospective follow-up evaluations. The institutional review board of the Samsung Medical Center approved this study.
Evaluation and epidural blood patch
All patients with suspected SIH were evaluated using gadolinium-enhanced brain MRI, computed tomography (CT), or MR myelography. At the Samsung Medical Center, MR myelography has been the preferred choice of diagnosis since 2019, thus, the majority of the patients underwent MR myelography. All imaging findings were interpreted by two neuroradiologists (MS and EYK, with 8 and 23 years of experience in neuroradiology, respectively). As the current ICHD-3 criteria for headache attributed to low CSF pressure requires at least one proof of CSF leakage on imaging (brain or spine) and low CSF pressure (<60mm CSF) (12), lumbar puncture was needed to document low CSF pressure in imaging-negative patients with suspected SIH. However, lumbar punctures were actually performed in only a few patients included in this study. The EBP was performed under C-arm fluoroscopic guidance by experienced anesthesiologists.
Using a brain MRI-based scoring system (Bern Score) (34), the probability score for the likelihood of an CSF leak was assessed in all imaging-negative patients and compared between patients included in this study and those excluded. The score comprised of major components (2 points each) including pachymeningeal enhancement, engorgement of venous sinus, and effacement of the suprasellar cistern of 4.0 mm or less and minor ones (1 point each) including subdural fluid collection, effacement of the prepontine cistern of 5.0 mm or less, and mamillopontine distance of 6.5 mm or less (34). Based on the literature, the probability of having a CSF leak was classified into low (total scores ≤2 points), intermediate (3–4 points), and high (≥5 points).
Outcome
All patients were assessed for treatment outcomes both at discharge and three months after discharge. As part of the prospective registry, we collected information on the presence of orthostatic headache and headache intensity (supine vs. sitting or standing) three months after treatment. Treatment outcome was first assessed quantitatively on the basis of improvement of orthostatic component and 50% response at discharge and three months after discharge. A 50% response was defined as a 50% or greater reduction in the maximal headache intensity presented with a numeric rating scale. An improvement of orthostatic component was defined as no clear headache exacerbation by sitting or standing. The treatment outcome was quantitatively defined as having both 50% response and improvement of orthostatic component at discharge and three months after discharge. Treatment outcome was also qualitatively assessed at three months and grouped into complete remission, persistence of orthostatic headache, and persistence of non-orthostatic headache.
Statistical analysis
We collected the data in an Excel spreadsheet (Microsoft) and used Microsoft Excel for all the descriptive analysis. Data are presented as number (percentage) or median (interquartile range; IQR) unless specified. Treatment outcomes were presented at each time point. Subgroup analysis was performed in terms of treatment outcomes stratified according to the number of EBP conducted. The Bern Scores were compared by using the Student’s t-test.
Results
Patient characteristics
During the study period, 191 patients were admitted due to suspicion of SIH. Among the 121 patients who underwent both brain MRI and CT or MR myelography, 74 showed at least one abnormality to indicate a diagnosis of SIH. Of the 47 (38.8%) patients who had normal brain and spinal imaging findings, we identified 21 treatment-naïve patients without a prior history of EBP who underwent blind EBP for the first time in the study center (Table 1). A flowchart of the study procedure is presented in Figure 1. Among the 21 patients included in this study, most were female (76.2%), with a mean age of 40 years (range, 16–64 years). Preceding minor trauma was reported in eight (38.1%) patients: heavy lifting (n = 4), aerobic exercise (n = 1), use of a massage chair (n = 1), minor in-car traffic accident (n = 1), and vomiting (n = 1). All the patients had daily headaches which persisted while standing or sitting. The median headache intensity on the numeric pain rating scale (range 0–10) was 7 (interquartile range 6–8) and 0 (interquartile range 0–2) while standing and in supine position, respectively. The median time from standing to the maximal headache intensity was five minutes (interquartile range 1–52.5 min). Most of the cases (19 patients, 90.5%) reported that their headache peaked within two hours after standing, while the remaining two (9.5%) had “second-half-of-the-day” headache.

Flow diagram of patient selection in this study.
Information regarding excluded patients
A total of 121 patients underwent both brain MRI with gadolinium enhancement and CT or MR myelography. Among them, 45 patients showed abnormal findings in gadolinium-enhanced brain MRI: subdural fluid collection (n = 1), pachymeningeal enhancement (n = 38), venous engorgement (n = 7), pituitary hyperemia (n = 14), and brain sagging (n = 3). Sixty patients showed abnormal findings in CT (n = 18) or MR (n = 43) myelography.
In 47 patients who had no abnormalities in brain or spinal imaging, 26 were not included in the analysis because of higher suspicion of other headache disorders (n = 4), epidural blood patch was done in other hospitals prior to visit (n = 13), refusal of epidural blood patch (n = 3), and symptom remission before or during the evaluation (n = 4).
When we compared the Bern Score in imaging-negative patients who were included (n = 21) and excluded (n = 26) in this study, the mean Bern Score was higher in the included patients than in those excluded (1.8 ± 1.40 vs. 1.0 ± 1.26, p = 0.043). However, the Bern Scores were overall low in both groups, with none having a high probability of SIH based on the score (5 or higher) in each group. Patients were classified as having low and intermediate probability of SIH in 13 (61.9%) and 8 (38.1%) in the included group and 22 (84.6%) and 4 (15.4%) in the excluded group, respectively (p > 0.999).
Investigation and treatment
Among the 21 patients, spine imaging was performed using CT myelography in five (23.8%) patients and MR myelography in 16 patients (76.2%). Nine (42.9%) patients underwent lumbar puncture to measure the opening pressure. The median opening pressure was 13.8 cmH2O (range 9.2–21.5 cmH2O), and none of the patients who underwent lumbar puncture showed an abnormally low opening pressure. A typical case is shown in Figure 2.

Example cases of suspected spontaneous intracranial hypotension with and without imaging abnormalities.
Seventeen (81.0%) patients received a single EBP, while two each (9.5%) received EBP twice and thrice. The region of blind EBP was determined based on the safety, frequency in the imaging-positive patients, and location of preceding events that could be a plausible cause of CSF leak, if any. The most frequently performed site of the first EBP was the L4-5 level (33.3%), followed by the C7-T1 level (23.8%). The most frequent site of any EBPs was the L4-5 (29.6%), followed by C7-T1 (22.2%). The median volume of EBP was 11 mL (IQR 10–14) and 15 mL (IQR 10–19) in the cervicothoracic junction and lower lumbar region, respectively.
Treatment outcome
Treatment outcomes are summarized in Table 2. At discharge after the last EBP, 14 (66.7%) patients showed both 50% response and improvement of orthostatic component. Preventive medications were co-administered in five (23.8%) patients. In terms of safety, 15 patients experienced treatment-emergent adverse events. The most frequent treatment-emergent adverse event was back pain in 13 patients (86.7%), followed by itching and pressure-like headache in two (13.3%) patients. No serious adverse events were reported after the EBP.
Patient demographics and characteristics.

Data are presented as median (interquartile range).
Gd, gadolinium; NRS, numeric rating scale.
*Within one month before the symptom onset.
After three months after EBP treatment, three patients were able to discontinue oral preventive medications (patient 1: propranolol 40 mg/d, nortriptyline 20 mg/d with a total duration of one month; patient 2: nortriptyline 20 mg/day, tizanidine 1 mg/day with a total duration of one month; patient 3: flunarizine 5 mg/day with a total duration of three months). Only two (9.5%) patients continued oral preventive medications (patient 4: topiramate 100 mg/day; patient 5: nadolol 80 mg/day and topiramate 25 mg/day). Two patients who had less than 50% response immediately after following EBP procedure additionally showed ≥50% pain reduction after three months at the outpatient clinic. Including four patients who showed excellent response immediately after the EBP procedure and were lost to follow-up at three months, 19 patients (90.5%) had both 50% response and improvement of orthostatic component. When the treatment outcome was qualitatively assessed, the headache intensity was much reduced to numeric pain rating scale of 1 (out of 10), and complete remission was achieved in 11 (52.4%) patients (Table 3). Other detailed information regarding the remaining headache is provided in Table 3.
Subgroup analysis
In the subgroup analysis, the results were stratified by the number of EBP received (Table 4). In the subgroup of 17 patients who underwent EBP once, 76.5% experienced remission of orthostatic headache with a 50% responder rate of 88.2%, and 94.1% reported for any of the two outcomes. In two patients who underwent EBP twice, the orthostatic component was remitted in both patients (100%), and the 50% responder rate was 50%. In the subgroup of patients who received EBP three times, only one patient (50%) achieved remission of orthostatic headache and a 50% response.
Treatment outcome at discharge and 3 months after epidural blood patch.

Headache characteristics at three-month follow-up.
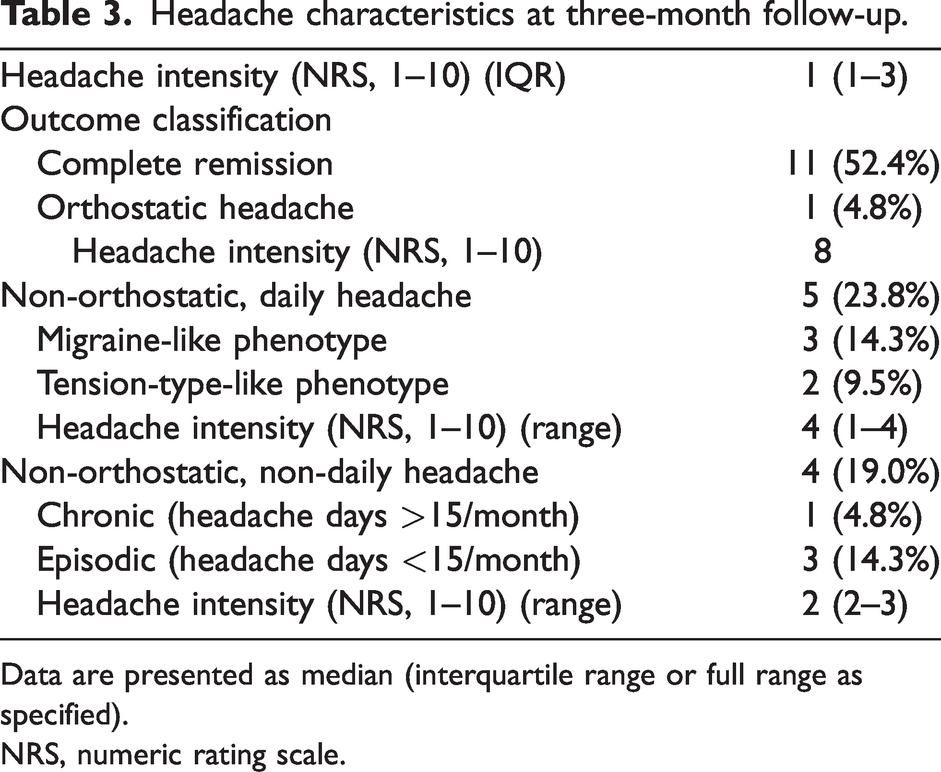
Data are presented as median (interquartile range or full range as specified).
NRS, numeric rating scale.
Subgroup analysis in terms of the number of epidural blood patch.

EBP, epidural blood patch.
Suggested strategy for the investigation and treatment of suspected SIH
We algorithmized the strategy for the investigation and treatment of suspected SIH (Figure 3). In patients with new onset headaches with orthostatic features otherwise unexplained by disorders other than low pressure headaches, we suggest performing non-invasive evaluations using gadolinium-enhanced brain MRI and MR myelography first. If there are any abnormalities in those tests, the diagnosis of definite SIH can be made and the treatment should be done with targeted or blind EBP based on the localization of CSF leakage on the myelography. When patients show negative non-invasive imaging findings, blind EBP can be tried first. If a patient does not respond to the first EBP, blind EBP can be repeated in spinal levels distant from the first EBP in case of high clinical suspicion of SIH. CT myelography can be considered for the exact localization of the leakage site. In cases where the clinical suspicion of SIH is low or intermediate, lumbar puncture can be considered for diagnostic clarity. If negative, patients can be treated with preventive medications and followed up. If this does not lead to satisfying treatment outcome, the clinical suspicion of SIH can be re-evaluated and repeated EBP or CT myelography can be considered again.

Algorithm for the investigation and treatment of new onset orthostatic headache.
Discussion
The major findings of this study are as follows: 1) Approximately 40% of patients with suspected SIH showed no abnormalities on brain and spine imaging; 2) In patients with normal brain and spine imaging, blind EBP yielded a high response rate for remission of orthostatic headache to non-orthostatic headache and reducing headache intensity by >50%; 3) In a small proportion of patients who underwent lumbar puncture, the diagnostic value was not significant when the brain and spine imaging findings were negative.
The first noteworthy finding of this study is that a high proportion (approximately 40%) of patients showed normal brain and spine imaging findings despite orthostatic headaches. Previous studies have reported the sensitivity of each diagnostic modality; however, heterogeneity exists regarding the study settings, diagnostic modality used, and inclusion criteria. Consequently, only a few studies have estimated the proportion of patients with normal findings on both brain and spinal imaging. Schievink et al. reported that of 107 patients with suspected SIH, approximately 14% showed no abnormalities on brain and spinal imaging findings (13). Akbar et al. reported that 15% of patients had no CSF leak on CT myelography and negative findings on MR in a highly selected group of 41 patients who underwent both CT myelography and MR myelography with intrathecal gadolinium (31). Compared to these two studies, our study yielded a higher proportion of patients with normal brain and spinal imaging. This discrepancy may be attributed to the broader inclusion of patients in our study. Although it is extremely difficult to identify the real cause of orthostatic headache when objective imaging findings are lacking, our study may indicate the possibility of underdiagnosis under the current diagnostic criteria and warrant broadening of the clinical suspicion of SIH.
Our second major finding was that blind EBP was effective in remitting orthostatic headaches and reducing headache intensity in patients with no imaging abnormalities. This type of information could not be obtained from previous studies, because most included patients with SIH were diagnosed using the ICHD criteria. The diagnostic criteria for SIH are based on any abnormalities in brain MRI, spinal imaging, or CSF opening pressure in the ICHD-3, plus the EBP response in the ICHD-2. A recent study on a topic similar to our study included the EBP response as a case definition of SIH, and therefore may be biased (24). We identified only one study in which the response rate after EBP was available in patients with suspected SIH but normal imaging findings, and the EBP response was not used as an inclusion (13). The study reported that only one out of 11 patients without brain and spinal imaging abnormalities responded to EBP. In contrast, our study yielded a high response rate of 66.7% having both 50% response and improvement of orthostatic component at discharge, 90.5% having both 50% response and improvement of orthostatic component at three months, and 52.4% showing complete remission at three months after EBP. This could be, in part, based on the sample size and definition of treatment response. In addition, as not all patients with normal imaging findings underwent EBP, the response rate in our study could have been overestimated as patients with high clinical suspicion were more likely to receive EBP. Nevertheless, our study supports the importance of EBP in patients with normal imaging findings. Considering the excellent safety profile of EBP reported in several studies, EBP should be considered in patients with orthostatic headache and clinical suspicion of SIH but without definite abnormalities in brain and spinal imaging.
In our study, lumbar puncture was performed in only nine patients and none had an opening pressure lower than the known normal range (6–20 cmH2O). This result suggests that the diagnostic yield of lumbar puncture may not exceed the therapeutic gain of empirical EBP. Moreover, it can cause additional CSF leakage and adversely affect the disease course. Considering this, we decided not to perform lumbar puncture in most of our patients. Given the high response rate and safety profile of empirical EBP in our study, we suggest that EBP, not lumbar puncture, should be the next step when brain and spinal imaging are negative in patients with clinically suspected SIH. Although the current ICHD-3 criteria require at least one brain MRI abnormalities, CSF leak in spinal imaging, or low opening pressure from the lumber puncture, a new diagnostic entity of “probable SIH” can be made in imaging-negative patients in whom lumbar puncture was avoided or deferred.
One of the strengths of our study is that this is the first prospective study to demonstrate the usefulness of EBP in patients with suspected SIH without imaging evidence. Another strength lies in the comprehensive evaluation using a structured follow-up protocol. Nevertheless, our study has some limitations that should be acknowledged. First, the number of patients included in this analysis was relatively small. Because this study was conducted in a tertiary university hospital, several of the patients had already received EBP prior to referral. In addition, some patients with a low clinical suspicion or those who refused invasive procedure did not undergo EBP. Second, digital subtraction myelography or lateral decubitus CT myelography was not available at Samsung Medical Center during the study period. As a result, we were unable to exclude the possibility of a CSF-venous fistula. However, blind EBP nevertheless yielded a high response rate. Finally, short-term oral preventives were combined to prevent post-EBP or post-SIH headaches in a small proportion of the patients, which may have affected the early response rate.
In conclusion, EBP is a feasible treatment for patients with suspected SIH lacking brain and spinal imaging abnormalities. We propose that EBP should be considered before lumbar puncture in this patient group given the low diagnostic yield of lumbar puncture and the possibility of deterioration after lumbar puncture.
Clinical implications
Approximately 40% of patients with suspected SIH showed no abnormalities on brain and spine imaging. Blind EBP yielded a substantial response rate in patients with normal brain and spine imaging. In cases with “probable SIH” where the orthostatic headache is prominent and there are no abnormalities in appropriate brain and spinal imaging and no possibilities of disorders other than SIH, the next step could be a therapeutic trial of EBP before performing an invasive diagnostic procedure.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP; No. 2020R1A2B5B01001826 to MJL).