
Abstract
There are limited data on the relationship between normal cerebrospinal fluid (CSF) opening pressure and bilateral transverse sinus stenosis (BTSS); there are also several conflicting reports about the upper limit of normal CSF opening pressure. To evaluate the influence of BTSS on the upper limit of normal CSF opening pressure, we prospectively recorded lumbar CSF opening pressures in 217 adult patients with neurological symptoms who underwent cerebral magnetic resonance venography (MRV). The CSF opening pressures ranged between 65 and 286 mmH2O (mean = 149.3,
Keywords
Introduction
There are several conflicting reports about what is the upper limit of normal cerebrospinal fluid (CSF) opening pressure. Indeed, 200 mmH2O was the early accepted upper limit of normal CSF pressure in healthy subjects (1). However, some authors (2) have reported CSF pressures > 200 mmH2O in 16% of 31 healthy individuals, and others (3) have obtained opening pressures between 200 and 250 mmH2O in 25% of 41 obese controls. This latter finding shifted the upper limit of normal CSF pressure to 250 mmH2O in obese subjects. More recently, another study (4) demonstrated that body mass index (BMI) did not significantly influence CSF opening pressure, which was < 200 mmH2O in both obese and non-obese subjects. A very recent study (5), however, indicated that CSF pressure of up to 280 mmH2O may be considered normal irrespective of BMI. Therefore, the definition of upper limit of normal CSF opening pressure remains controversial, making the diagnosis of intracranial hypertension syndrome difficult in clinical practice.
Another source of confusion stems from the relationship between CSF pressure and bilateral transverse sinus stenosis (BTSS). It has recently been observed that BTSS, identified through cerebral magnetic resonance venography (MRV), may be associated with idiopathic intracranial hypertension (IIH) without papilloedema (IIHWOP) in patients who had recurrent or chronic headache as an isolated neurological symptom (6,7).
In the current study, therefore, we measured lumbar CSF opening pressure in adult patients with neurological symptoms who underwent MRV in order to evaluate the influence of BTSS on the upper limit of normal CSF opening pressure.
Methods
Participants
Three hundred and fifty-nine adults with neurological symptoms underwent screening for eligibility for inclusion in the study; 142 of these subjects were ineligible. Two hundred and seventeen subjects were included in this prospective study: 167 had normal cerebral MRVs and 50 had BTSS. Institutional Review Board approval was obtained for the study, and written informed consent was obtained from all subjects.
Subjects
A total of 217 subjects (79 men and 138 women aged 16–76 years, mean 39.9 years) were enrolled between January 2006 and January 2008 among patients admitted to the Institute of Neurology (Catanzaro, Italy). Eligible patients included those with neurological symptoms who were candidates for lumbar puncture (LP) for diagnostic purposes. MR and MRV of the brain were performed before LP. All patients underwent LP to measure CSF opening pressure. Patients' characteristics were recorded, including age, gender, BMI (weight in kg divided by the square of height in metres), medications, evidence of systemic disease and presence of sleep apnoea. They were all seen by an ophthalmologist to confirm the absence of papilloedema. The criteria for exclusion from this study were: presence of signs and symptoms of generalized intracranial hypertension, such as persistent daily headache, intracranial noises, transient visual obscurations, double vision, pulsatile tinnitus, papilloedema and sixth nerve palsy or headache characteristic of low CSF pressure syndrome; MR evidence of structural brain lesions or hydrocephalus and evidence of current or prior cerebral venous thrombosis; abnormalities of CSF composition; and drug intake or systemic disease, all of which could lead to abnormal CSF pressure values. Migraine and tension-type headache were diagnosed according to the criteria established by the International Headache Society (8).
CSF opening pressure measurement
All LPs were performed by the same operator (F.B.) using a technique described elsewhere (4). In short, pretreatment of patients with anxiolytics and local anaesthesia was given. In a quiet room, with the subject in the left lateral decubitus position, a standard 22-G (only occasionally 20-G) Quincke pointed spinal needle with three-way stopcock was inserted. The opening pressure was recorded by using a manometer positioned at a 90° angle to the spinal canal with the patient's knees and hips in the extended position and neck straightened. The head and spine were strictly horizontal. The manometer was attached with an estimated loss of < 0.5 ml of fluid. CSF opening pressure was recorded for approximately 4 min, to be certain that the patient was adequately relaxed and that the pressure values had stabilized.
Image analysis
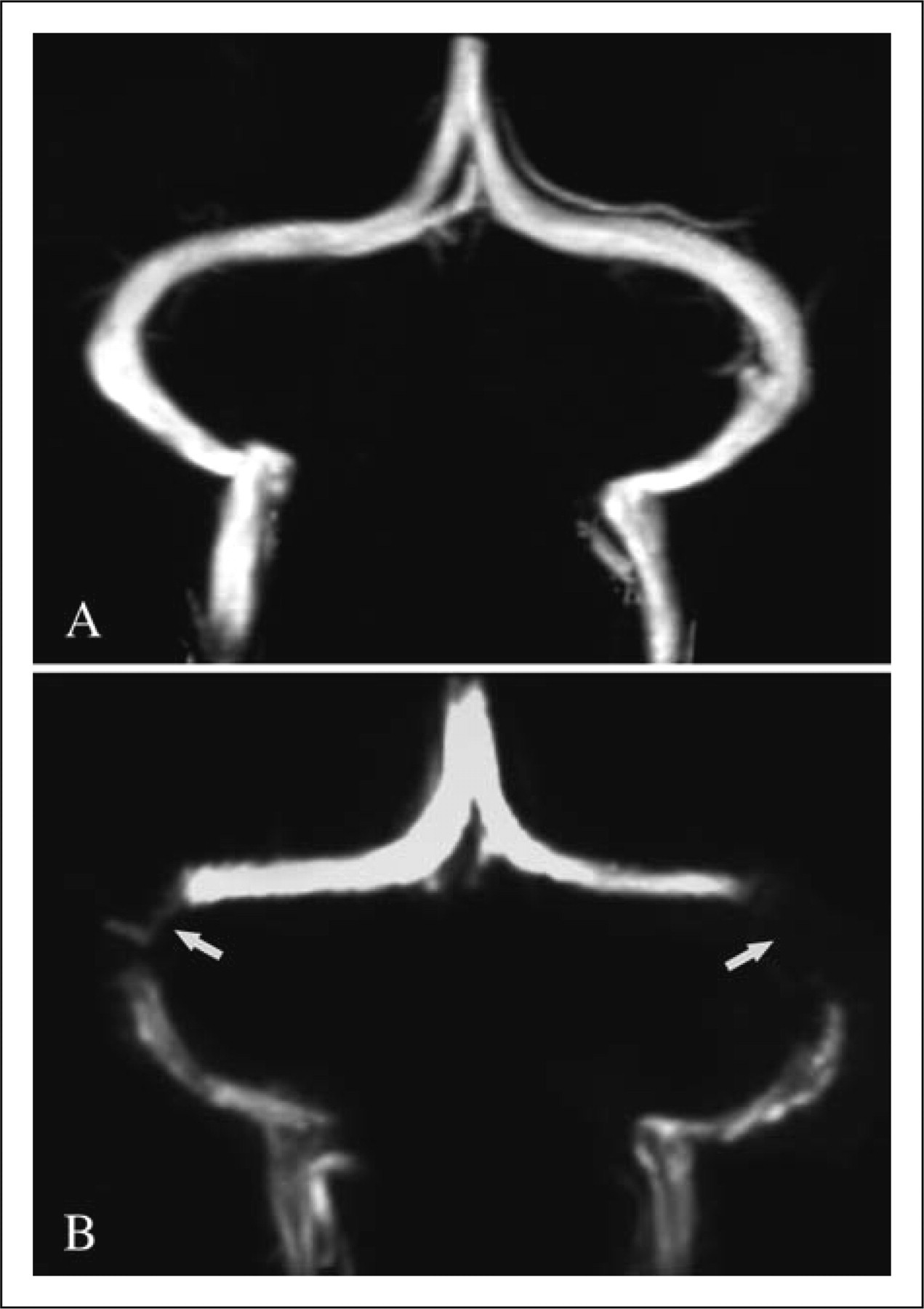
MR and MRV of the brain were performed on all subjects on a 1.5-T scanner (GE Medical Systems, Milwaukee, WI, USA). Brain MR consisted of sagittal T1- and transverse T2-weighted spin echo sequences with a slice thickness of 5 mm and an interslice gap of 1 mm. MRV was performed using 3D-PC techniques as described elsewhere (9). All brain MR and MRV were analysed by the same neuroradiologists who were blind to each patient's history. We classified the transverse sinus (TS) stenosis as present or absent. BTSS was considered present when the signal flow was poor or lacking (flow gap) in the mid-lateral portion of both transverse sinuses, while unilateral TS stenosis was considered present when flow gaps were found in one TS.
Statistical analyses
One-way analysis of variance and post hoc test were used to assess differences in CSF pressure, BMI and age among the groups. Characteristics of the patients with low and high opening pressure were analysed using the unpaired t-test. All P-values were two-tailed, and the α level was set at P < 0.05.
Results
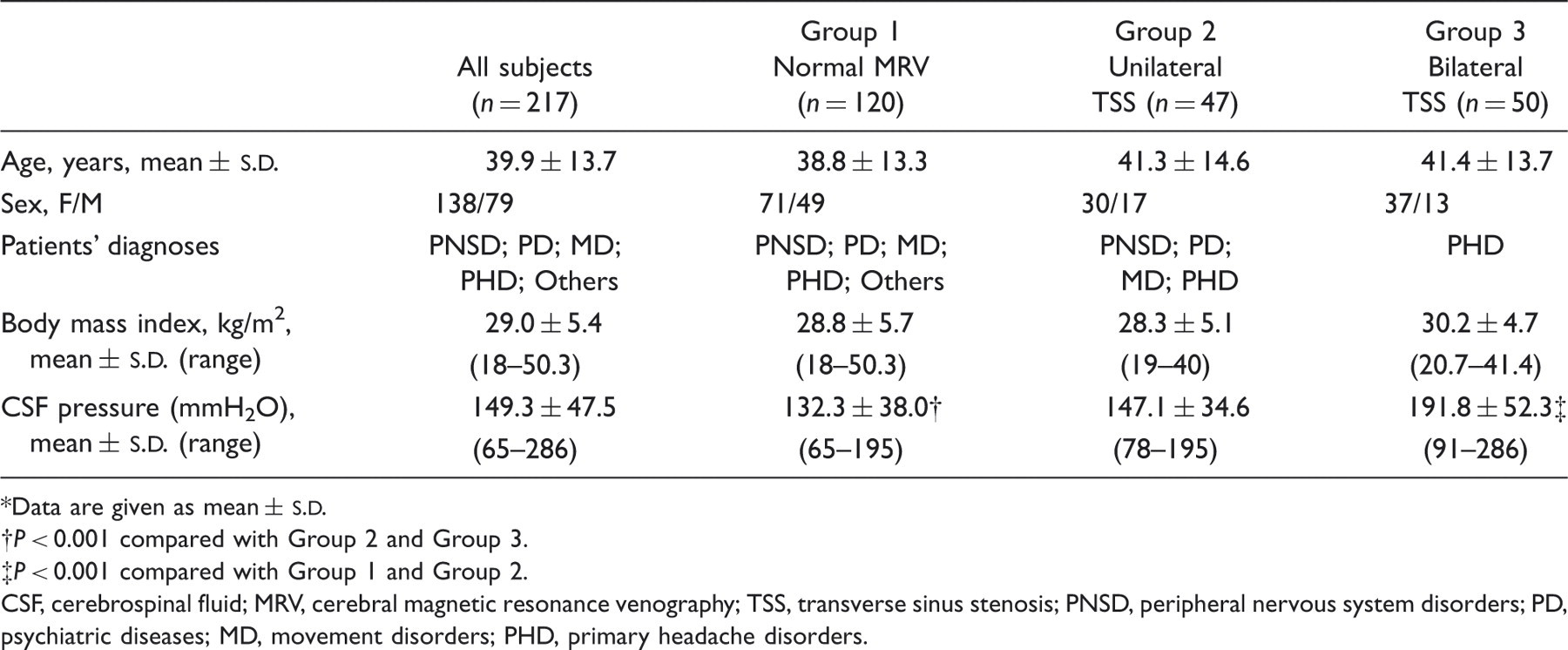
The characteristics of the 217 subjects studied are summarized in Table 1. The range of CSF pressure ranged between 65 and 286 mmH2O (mean = 149.3, Flow diagram from screening to study completion. Of the 359 patients prescreened, 142 were ineligible. MRV, magnetic resonance venography; BTSS, bilateral transverse sinus stenosis; BTSS Magnetic resonance venography of the transverse sinuses, showing both normal appearance of the transverse sinuses (A) and flow gap in the mid-lateral portion of transverse sinuses (arrow) (B). (A,B) Coronal view. Characteristics of the 217 patients with neurological symptoms Lumbar CSF pressures in patients with neurological symptoms grouped according to MRV findings*
Data are given as mean ±
P < 0.001 compared with Group 2 and Group 3.
P < 0.001 compared with Group 1 and Group 2. CSF, cerebrospinal fluid; MRV, cerebral magnetic resonance venography; TSS, transverse sinus stenosis; PNSD, peripheral nervous system disorders; PD, psychiatric diseases; MD, movement disorders; PHD, primary headache disorders. MRV findings in patients with neurological symptoms grouped according to lumbar CSF pressures*
Data are given as mean ± CSF, cerebrospinal fluid; MRV, cerebral magnetic resonance venography; PNSD, peripheral nervous system disorders; PD, psychiatric diseases; MD, movement disorders; PHD, primary headache disorders.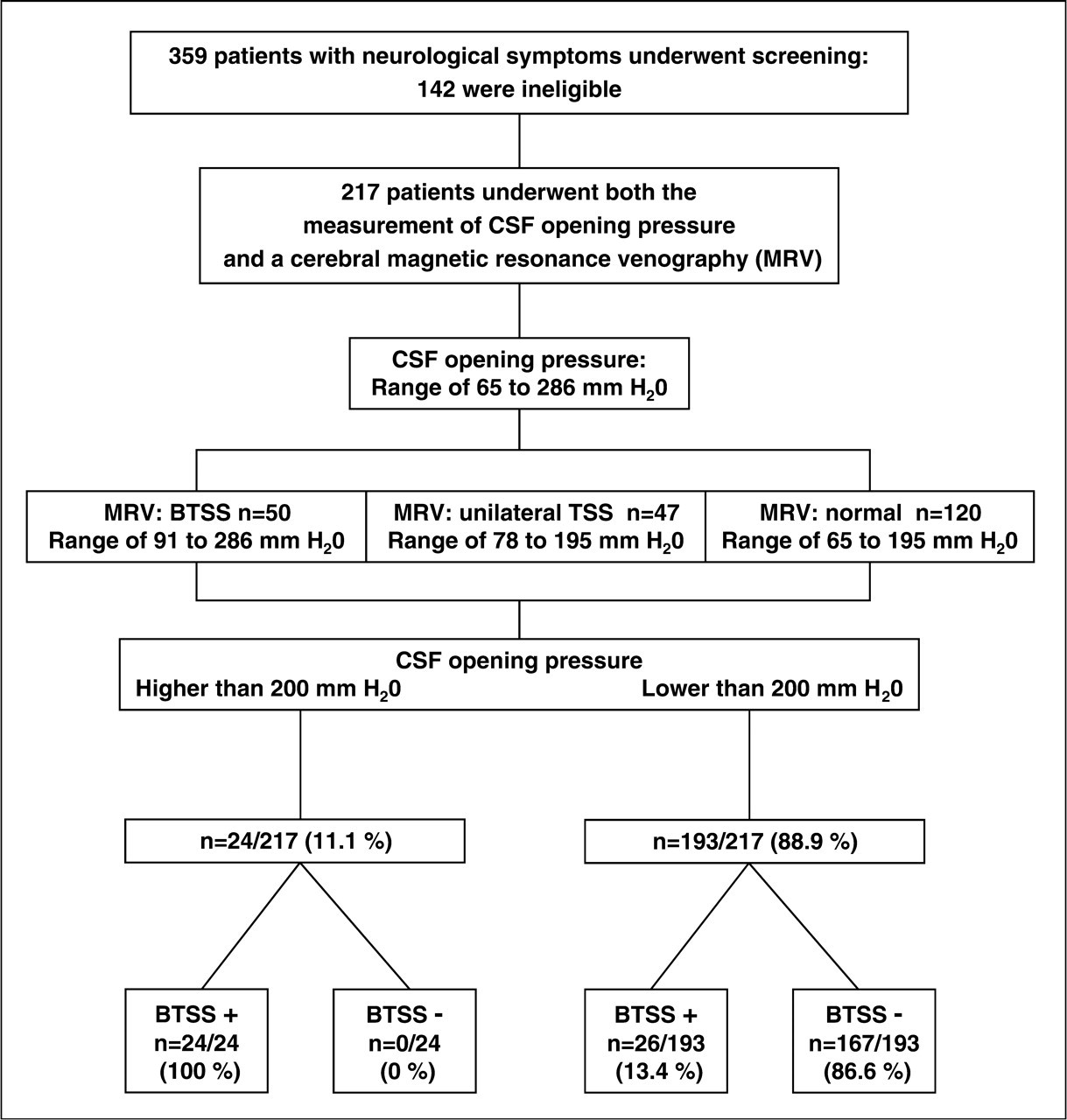


Discussion
Every patient with an opening pressure > 200 mmH2O displayed BTSS on MRV, whereas only 13% of patients with CSF pressures < 200 mmH2O displayed BTSS. In contrast, no patients with both normal appearance of transverse sinuses and unilateral TS stenosis on MRV had CSF pressures > 200 mmH2O. All patients with BTSS were headache sufferers. These results demonstrate that the upper limit of normal CSF opening pressure is related to BTSS in headache sufferers. In accordance with these data, there is evidence showing BTSS in cases of IIH with and without papilloedema (6,7,10). To our knowledge, this is the first report showing opening pressures between 200 and 280 mmH2O associated with BTSS in adult patients with neurological symptoms, in which MRV was used for exploring the disturbance of flow of transverse sinuses in patients who were candidates for LP.
The mechanism by which BTSS may increase CSF pressure is still being debated (11,12). Some have suggested that obstruction of venous outflow, especially of transverse sinuses, can lead to venous hypertension, which in turn causes an increase in intracranial pressure (13–16). The relationship between increased intracranial pressure and sinus venous pressure in patients with IIH is well understood (13). Indeed, some authors have demonstrated the presence of a pressure gradient between the proximal and distal parts of the TS in patients with IIH (14). This observation was confirmed in patients with IIH who showed, on MR venography and manometry, a BTSS with elevated venous pressure proximal to the stenosis. Dilation of one of the transverse sinuses with a stent decreased both the pressure gradient and the intracranial pressure, suggesting a causal relationship between venous outflow obstruction and increased intracranial pressure (15,17). The above-mentioned data support our finding that CSF opening pressure is related to BTSS. However, the cause of BTSS remains uncertain. It is noteworthy that sinus stenosis always occurs in the mid-lateral portion of the TS, suggesting that there must be some anatomical reason that makes the mid-lateral part of the TS the preferential site for developing an obstructive process. There is anatomical evidence (18,19) showing large arachnoid granulations and septa of varying sizes within transverse sinuses of normal brains from human cadavers. These latter findings support the hypothesis that the presence of a large septum or large arachnoid granulation may be one of the causes of BTSS observed in our patients. Interestingly, our study showed that 13% of patients with an opening pressure < 200 mmH2O had BTSS. Consistent with this finding, in a previous study (12) we found that BTSS persisted in patients with IIHWOP when CSF pressure normalized, suggesting that BTSS is only one of the contributing factors involved in IIH. In accordance with this evidence (12), two patients in our study with BTSS and normal CSF pressures displayed opening pressures > 200 mmH2O upon second LP. This finding highlights that BTSS may be not a normal anatomical variant but a pathological process, hence a possible confounder in determining the upper limit of normal CSF pressure. Indeed, a recent study (20) has shown that patients with marked BTSS should have also a cerebral blood flow towards the upper limit of normal to be symptomatic. Moreover, in our series no patients with normal appearance of transverse sinuses or unilateral TS stenosis had opening pressure > 200 mmH2O. These data are in agreement with the observation that patients with either normal appearance of transverse sinuses (4,21,22) or unilateral TS stenosis (21) on MRV had CSF pressures < 200 mmH2O. Furthermore, the observation that dilation of one of the transverse sinuses with a stent normalized CSF pressure in patients with IIH associated with BTSS, supports our finding that only patients with BTSS had opening pressures > 200 mmH2O. Taken together, the above observations and our findings demonstrate the relationship between BTSS and CSF opening pressure, suggesting that headache sufferers with opening pressures > 200 mmH2O should be tested for BTSS by MRV.
At variance with these data is recent evidence (23) showing a high frequency of IIHWOP in patients with chronic migraine (CM), in which all patients had normal MRV. Our major criticism is the lack of information about the MRV technique used for exploring the disturbance of flow of transverse sinuses in CM patients. A correct MRV technique is needed to demonstrate the absence of BTSS. On MRV, 2D-time-of-flight images and 3D-PC images acquired with a velocity encoding factor (VENC) of 40 cm/s tend to bias the interpretation of flow signal toward normality, underestimating the disturbances of flow of transverse sinuses, whereas 3D-PC MRV set with the VENC to 15 cm/s represents the best non-invasive technical approach for visualizing BTSS in patients with IIH (9). Indeed, in the current study using 3D-PC MRV technique with VENC set to 15 cm/s we have found BTSS in a number of patients who were candidates for LP. Nevertheless, an elevated cerebral blood flow could also explain the elevated CSF pressure in the absence of BTSS in patients with CM (20).
At variance with our findings, moreover, previous reports have found opening pressures > 200 mmH2O in normal subjects (2,3,5). These results supported the observation that opening pressures up to 250 mmH2O may be considered normal. The elevated CSF pressures obtained in the aforementioned studies may be due to confounding factors, such as factors that can increase CSF pressure. BTSS, in fact, was not investigated by using MRV in the previously mentioned studies that determined the normal limits of CSF opening pressure (2,3,5). In these studies, therefore, the presence of BTSS among patients with opening pressures > 200 mmH2O cannot be excluded. This latter observation may be a likely explanation for higher CSF pressure values obtained in previous studies, and it emphasizes that factors potentially increasing CSF pressure, such as BTSS, should be carefully considered when investigating the normal limits of CSF opening pressure.
Indeed, in this study to determine the CSF opening pressure as accurately as possible, we took into consideration other confounding factors that potentially increase CSF pressure: in order to avoid elevated CSF pressure from the Valsalva manoeuvre, which encompasses anxiety in acute pain (24), we adopted both local anaesthesia and pretreatment of patients with anxiolytics; to be certain that the patient was adequately relaxed and that the pressure values had stabilized, the steady-state opening pressure was recorded for approximately 4 min in a quiet room; patients with elevated levels of CSF protein or patients who used drugs influencing CSF pressure were excluded. Unlike the authors of this study, previous authors (2,3,5) who investigated normal limits of CSF pressure did not thoroughly characterize these factors, all of which can lead to elevated opening pressure. Furthermore, the signs and symptoms considered in the exclusion criteria reflect those of both raised intracranial hypertension and low CSF pressure syndrome. Hence, our exclusion criteria left us with patients in whom most practising neurologists would not suspect an altered intracranial pressure disorder.
Finally, our findings prove that when CSF opening pressure is determined with careful control for potential confounders, the value of 200 mmH2O may be a reliable upper limit of normal CSF opening pressure in adult patients with neurological symptoms. Thus, in everyday practice, we suggest that headache sufferers with opening pressures > 200 mmH2O should be carefully investigated for detecting BTSS by using MRV.
Footnotes
Competing interests
None to declare.