
Abstract
It is unknown if comorbid conditions account for the association between migraines and work performance. This issue was investigated in the National Comorbidity Survey Replication (n = 9282). Twelve-month severe or persistent migraines and other headaches were assessed with comorbid 12-month mental and physical disorders using the WHO Composite International Diagnostic Interview. Work performance was assessed using the WHO Health and Work Performance Questionnaire. Significant associations of these conditions with work disability disappeared with controls for comorbid disorders, but severe or persistent migraines continued to predict work loss days even with controls. Individual-level and societal-level annual human capital values were $1165 and $9.3 billion for this subset of migraines. Roughly 20% of these associations were due to comorbidity, 60% to direct effects and 20% to indirect effects through temporally secondary comorbidities. These strong associations suggest that workplace interventions for severe or persistent migraines might have a positive return-on-investment for employers.
Epidemiological research shows that migraine is a commonly occurring condition, affecting as many as 18% of women and 6% of men (1), that has substantive adverse financial effects associated with workplace outcomes (being out of the labour force, sickness absence, low work performance) (2–4). These results have led to recent calls for the expansion of migraine screening and treatment programmes in workplace settings as a way to reduce the indirect workplace costs of migraine (5–7) as well as to address the problem of low migraine detection and treatment (8–10). Implementation of such interventions might be premature as an alternative interpretation of existing results exists. Specifically, migraines are known to be highly comorbid with a number of other physical (11,12) and mental (13,14) disorders (13,15) and the work impairments associated with migraines are known to increase with comorbidity (16,17). This raises the possibility that comorbidities might either account for the associations of migraines with workplace outcomes or, alternatively, that the strength of the associations between migraines and workplace outcomes might vary as a function of the presence or absence of other comorbid disorders.
No previous study of the predictive associations between migraines and workplace outcomes has investigated these possibilities comprehensively. However, a recent report based on the nationally representative National Comorbidity Survey Replications (NCS-R) (18), which included not only working people, but also homemakers, students and others, showed that the significant total-sample associations between headaches (distinguishing migraines from other headaches) and role impairment in the WHO Disability Assessment Schedule (19) were largely explained by comorbid physical and mental disorders (20). In the light of this finding, it is important to examine whether comorbidity explains the associations of migraines with workplace outcomes. The current report presents such an analysis based on the NCS-R. Associations between migraines and workplace outcomes are assessed with the WHO Health and Work Performance Questionnaire (HPQ) (21,22) both with and without controls for a wide range of comorbidities.
Methods
Sample
The NCS-R design has been described extensively elsewhere (18) and consequently will be reviewed only briefly here. The NCS-R is a nationally representative face-to-face household survey carried out in 2001–2003. The response rate was 70.9%. The interview was administered in two parts. Part I included core assessments of DSM-IV mental disorders administered to all respondents (n = 9282). Part II included questions about physical disorders, impairments and other correlates administered to all Part I respondents who met lifetime criteria for any core disorder plus a roughly one-in-three probability sub-sample of other respondents (n = 5692). The Part II sample was weighted to adjust for the over-sampling of Part I respondents with DSM-IV disorders. The Part II sample is used in the current report. A more detailed discussion of NCS-R sampling and weighting procedures is presented elsewhere (23).
Measures
Migraines and other headaches
The NCS-R included a checklist of chronic physical disorders selected from the list used in the U.S. National Health Interview Survey (24,25). Respondents were asked to report both lifetime presence, age-of-onset (AOO) and occurrence during the past 12 months of each disorder. Only disorders present in the past 12 months are considered here. Headaches were assessed with a question about ever experiencing ‘frequent or severe headaches’. People who reported such headaches in the past 12 months were then asked additional questions to determine whether they met the International Headache Society criteria for migraine (ICHD-II) (26). Twelve-month headaches that did not meet the criteria for migraine are also considered as a point of comparison with migraine. Respondents were classified into mutually exclusive categories of having frequent or severe migraines, other frequent or severe headaches, or not having 12-month frequent or severe headaches.
Comorbid physical disorders
As described in more detail elsewhere (27), seven additional classes of chronic physical conditions were assessed in the NCS-R chronic conditions checklist. These included cancer, cardiovascular disorders (heart attack, hypertension, other heart disease, stroke), diabetes, digestive disorders (irritable bowel syndrome, ulcer), musculoskeletal disorders (arthritis, chronic back or neck problems), respiratory disorders (allergies, asthma, chronic obstructive pulmonary disorder) and sense organ impairments (hearing impairment, vision impairment). As with headaches, only disorders present in the past 12 months are considered here. Assessments of chronic conditions based on checklists like this have been widely used in population-based surveys and have been shown to yield more accurate reports than estimates derived from open-ended condition questions (28). Methodological studies have documented good concordance between responses to checklist questions and independent medical records (29–31). As reported elsewhere (32), the prevalence estimates of these disorders in the NCS-R are in accordance with those in other large-scale community surveys.
Comorbid mental disorders
As described in more detail elsewhere (33), mental disorders were assessed with Version 3.0 of the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI) (34), a fully structured lay-administered interview designed to generate research diagnoses of commonly occurring DSM-IV (35) mental disorders. The CIDI assessed 20 different mental disorders in four classes (anxiety, mood, externalizing and substance disorders). Mental disorders are considered here only if they were present in the past 12 months. Generally good concordance was found in an NCS-R clinical reappraisal study (36) between DSM-IV diagnoses based on the CIDI and diagnoses based on independent clinical assessments (37).
Socio-demographic controls
Socio-demographic controls used here include age, sex, race-ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, other), education (less than high school graduate, high school graduate, some college, college graduate), employment status (employed or self-employed, homemaker, student, retired, disabled, looking for work, other) and broad occupational categories (professional, sales-clerical, technical-precision crafts, service-general labourer). Work disability was considered an outcome in one part of the analysis in order to determine if migraines are related to being unable to work. The remainder of the analysis was then carried out among respondents who were either employed or self-employed at the time of interview.
Workplace outcomes
Absenteeism and work performance over the past month (4 weeks) were assessed with the WHO Health and Work Performance Questionnaire (HPQ) (21,22). Absenteeism was defined in terms of days of missed work, while work performance was defined using a 0–10 summary scale where 0 means doing no work at all on days at work and 10 means performing at the level of a top worker. Importantly, respondents were not asked to make inferences about the health problem(s) responsible for their absenteeism or low work performance. Information about salary was used to transform the measures of absenteeism and work performance from a time metric to a salary metric for purposes of estimating human capital loss associated with migraines and other headaches. Salary was incremented by 25% to estimate fringe benefits. Previous research has documented good concordance of HPQ absenteeism and work performance measures with objective measures based on payroll records and supervisor ratings (21,22).
Analysis methods
Prevalence estimates of frequent or severe migraines and other headaches were compared across socio-demographic sub-samples. Logistic regression analysis was used to study patterns of comorbidity of headaches with other disorders. Logistic regression coefficients and their standard errors were exponentiated to create odds-ratios (ORs) and 95% confidence intervals (CIs) for ease of interpretation. Logistic regression analysis was also used to estimate associations of history of recent frequent or severe migraines and other headaches with work disability, while linear regression analysis was used to estimate associations of history of recent frequent or severe migraines and other headaches with absenteeism and work performance among workers. Twelve-month prevalences of frequent or severe migraines and other headaches were coded as yes-no dummy predictor variables in these regression equations. Socio-demographic controls were included in all equations.
These equations were then elaborated to include controls for comorbid physical and mental disorders. The effects of comorbid disorders that mediate the associations of recent frequent or severe migraines or other headaches with work performance (i.e. disorders that are to some degree caused by headaches and have independent effects on work performance) can be considered indirect effects of headaches. As a result, a rough distinction was made between comorbid disorders likely to have started at an earlier age than headaches (referred to as temporally secondary disorders) and those likely to have started at the same age or later age than headaches (referred to as temporally primary disorders). Temporally secondary comorbid disorders were defined as those with an AOO later than that of headaches in at least 70% of comorbid cases. All other comorbid disorders were considered temporally primary.
A final elaboration of the equations evaluated the statistical significance of interactions between headaches and summary measures of number of comorbid physical disorders and number of comorbid mental disorders in predicting the outcomes. These summary measures of comorbidity were used because we lacked sufficient statistical power to evaluate the modifying effects of individual comorbid disorders.
In interpreting the results of the analyses, it is important to note that the key predictors in the regression equations are measures of disorders present at some time during the 12 months before interview, while the workplace outcomes were assessed for the 1 month (not 12 months) before interview. This means that the regression coefficients should be interpreted as the average effects of 12-month disorders on work performance in a typical month of the year, taking into consideration the fact that the disorders are not always active throughout the year. A more detailed discussion of the logic of this comparison is presented elsewhere (32).
Because the NCS-R data are weighted and clustered, the Taylor series linearization method (38) implemented in the SUDAAN software system (39) was used to obtain design-based estimates of statistical significance. Significance tests of sets of coefficients in the logistic regression equations were made using Wald χ2 tests based on design-corrected coefficient variance-covariance matrices. Statistical significance was consistently evaluated using 0.05-level two-sided tests.
Results
Prevalence and socio-demographic correlates
Socio-demographic predictors of frequent or severe headaches in the 12 months before interview among employed or self-employed Part II NCS-R respondents

Significant at the 0.05 level, two-sided test.
The headache questions were asked in a way such that respondents could be classified as having migraines or other headaches but not both.
Unweighted number of respondents in the subsample (e.g. there are a total of 2139 employed or self-employer women in the sample, of whom 8.9% had frequent or severe migraines, another 10.3% had other frequent or severe headaches, and the remaining 80.8% did not have frequent or severe headaches).
Based on a multivariate logistic regression equation that included all socio-demographic variables as predictors.
Comorbidities with physical and mental disorders
Conditional 12-month prevalence and comorbidity of chronic physical disorders with frequent or severe headaches among employed or self-employed Part II NCS-R respondents (n = 3955)

Significant at the 0.05 level, two-sided test.
Based on a separate multivariate logistic regression equation for each comorbid disorder that included all socio-demographic variables and the dummy predictors for migraines and other headaches as predictors.
Conditional 12-month prevalence and comorbidity of DSM-IV mental disorders with frequent or severe headaches among employed or self-employed Part II NCS-R respondents (n = 3955)
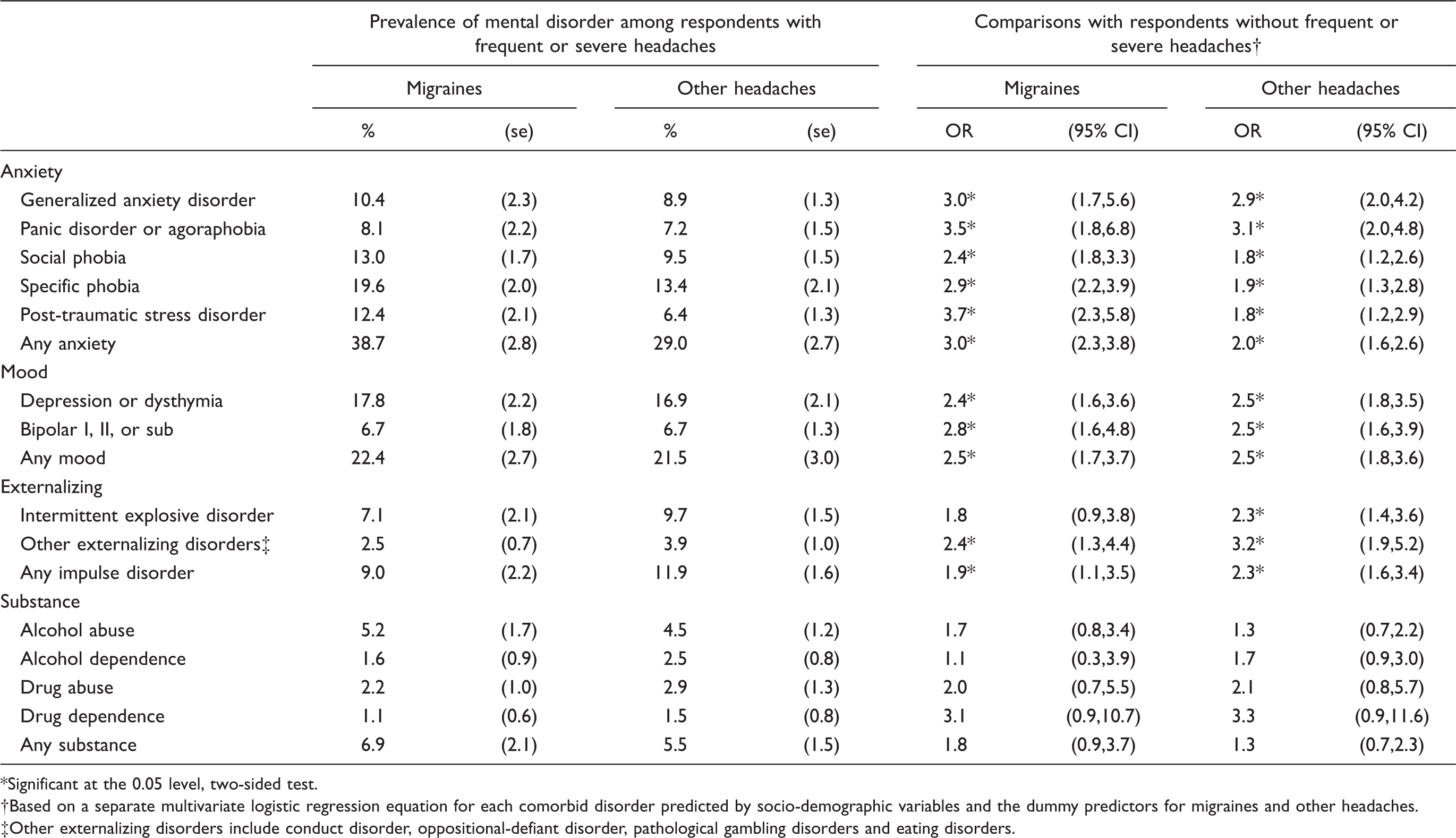
Significant at the 0.05 level, two-sided test.
Based on a separate multivariate logistic regression equation for each comorbid disorder predicted by socio-demographic variables and the dummy predictors for migraines and other headaches.
Other externalizing disorders include conduct disorder, oppositional-defiant disorder, pathological gambling disorders and eating disorders.
Temporal priorities between headaches and comorbid conditions
Comparisons of retrospective AOO reports of frequent or severe headaches with other disorders among respondents with 12-month migraines show that frequent or severe headaches have an earlier AOO in the clear majority of cases (70% or more) of only four of the physical disorders considered here: arthritis, other pain conditions, high blood pressure and ulcers, with between 71.5% (arthritis) and 89.9% (ulcers) of respondents reporting that their headaches started at an earlier age than these comorbid disorders (detailed results are available on request).The situation is somewhat different for other respondents with 12-month frequent or severe headaches, where an earlier AOO of the frequent or severe headaches in the clear majority of cases was found only for two of the physical disorders considered here: high blood pressure (70.8%) and diabetes (75.8%). In carrying out analyses of mediators, we considered these disorders temporally secondary and the others temporally primary with respect to frequent or severe migraines or other headaches.
Predictive effects on disability, sickness absence and work performance
Predictive effects of frequent or severe headaches on workplace outcomes with and without controls for comorbid physical and mental disorders among employed or self-employed Part II NCS-R respondents (n = 3955)

Significant at the 0.05 level, two-sided test.
The results reported in Part I are based on logistic regression equations in which dummy variables for 12-month presence of migraines and other headaches were used to predict disability (coded 1) vs. others in the labour force (coded 0, included the employed, the self-employed and the unemployed looking for work), controlling for socio-demographics. The estimates (Est) presented are odds-ratios and their 95% confidence intervals (CIs). The results reported in Parts II–III are based on linear regression equations in which dummy variables for 12-month presence of migraines and other headaches were used to predict number of past-the-job work performance (a 0–10 self-anchoring scale where 0 means doing no work and 10 means the work of a top worker), controlling for socio-demographics, hours expected to work and estimated performance of the average worker. The estimates (Est) presented in Parts II–III are linear regression coefficients and their 95% confidence intervals (CIs).
Linear regression analysis was used to evaluate the predictive effects of frequent or severe migraines and other headaches on absenteeism, controlling for socio-demographics (Table 4, Part II). Migraines but not other headaches were found to be significantly associated with absenteeism: 0.9 excess sickness absence days per month, which translates into 10.7 days per year for each worker with 12-month migraines. The latter, given the mean salary (plus an estimated average 25% fringe benefits) of workers with frequent or severe migraines in the sample, translates into a mean annual per capita human capital loss of approximately $1165 due to excess sickness absence among workers with these kinds of migraines. Given the prevalence of frequent or severe migraines in the labour force, these individual-level effects translate into an annualized 86.5 million lost workdays, with a human capital loss of approximately $9.3 billion in the US labour force. The regression coefficient for frequent or severe migraines predicting absenteeism becomes smaller (0.6 days per month) when controls are introduced for all comorbid disorders, but increases to a statistically significant 0.7 days per month if disorders that might be temporally secondary are deleted from the model. This suggests that approximately 60% (0.6/.9) of the gross association between frequent or severe migraines and sickness absence is due to the direct effects of these migraines, while another approximately 20% [(0.7–0.6)/0.9] is due to indirect effects through temporally secondary comorbid disorders and the remaining approximately 20% [(0.9–0.7)/0.8] is due to the confounding effects of temporally primary comorbid disorders. Linear regression analysis was also used to evaluate the predictive effects of frequent or severe migraines and other headaches on work performance, controlling for socio-demographics (Table 4, Part III). Neither type of headache was found to be a significant predictor of this outcome either in the model without controls or in models with controls for comorbid disorders.
Variation in effects based on comorbidity
No significant differences in the predictive effects of ether frequent or severe migraines or other headaches were found among respondents who differed in number of either comorbid physical, mental or overall disorders. (Detailed results are available on request.) This result holds true in evaluating interactions to predict disability (χ2 1 = 0.0–1.7, P = 0.19–0.98), absenteeism (χ2 1 = 0.0–1.7, P = 0.19–0.98) and work performance (χ2 1 = 0.0–1.7, P = 0.19–0.98).
Discussion
We found much lower prevalence estimates of frequent or severe migraines (5.5%) and other headaches (7.5%) in the NCS-R than in previous community surveys (11,40). The NCS-R prevalence estimates of other chronic conditions, in comparison, are quite similar to those found in other surveys (32). Our lower prevalence estimates of headaches almost certainly are due to the fact that we asked about ‘frequent or severe’ migraines and other headaches. In addition, some respondents might have interpreted the question as asking about frequent and severe headaches, leading to an even greater reduction in reported prevalence.
We documented statistically significant gross predictive associations of frequent or severe migraines and other headaches with work disability, but these were completely explained by comorbid disorders. Previous studies have generally found either non-significant (41,42) or substantively small (43) associations between headaches and employment status. The fact that we found somewhat larger gross associations presumably reflects our focus on frequent or severe headaches. That these associations were explained by comorbid disorders is indirectly consistent with evidence that the impairments associated with headaches are concentrated among the minority of headache sufferers who have complex comorbidities (11).
We documented a statistically significant gross predictive association between frequent or severe migraines, but not other headaches, and sickness absence but not work performance. The failure to find predictive effects on work performance might be interpreted to mean that headaches severe enough to impair workplace functioning typically lead US workers with frequent or severe headaches to remain at home (or go home early) rather than to go to (or stay at) work. However, that interpretation is indirectly inconsistent with the results of community surveys that show headache sufferers often go to work with impairing headaches (44–46). It might be that this seeming inconsistency is resolved by the fact that workers with frequent or severe migraines are more likely to stay at home, but results from a recent survey in a very large convenience sample are inconsistent with this interpretation as well in that the lost work performance reportedly caused by severe migraines in that study was due largely to low on-the-job work performance rather than to sickness absence (4).
Based on these results, the most plausible interpretation of our failure to detect an effect of frequent or severe migraines on work performance is that our measure of work performance was too coarse to detect this effect. It is noteworthy in this regard that the assessment method we used is different from the method used in many other studies of the effects of migraines on work performance, where respondents record the occurrence of migraines and assess the extent to which migraines lead to sickness absence or reduced work performance on the days of their occurrence. It is clear from these studies that migraineurs both miss many days of work due to migraines and also, when they go to work despite having a migraine, often have lower-than-average work performance. The approach used in the NCS-R, in comparison, asked respondents to report average work performance over a 1-month recall period, averaging days with migraines and days without migraines. This 1-month recall measure might be too coarse to detect the adverse effect of migraines on work performance on days when respondents had migraines. Another possibility, though, is that migraineurs might increase their work performance on days when they do not have migraines in order to make up for their lost productivity on days when they do have migraines. A diary study would be needed to assess this possibility rigorously, recording daily ratings of work performance of migraineurs both on days with and without migraines and comparing both sets of ratings with the ratings of workers who do not have migraines. We are aware of no such study, but this would be a valuable addition to the literature.
The significant predictive association found in the NCS-R between frequent or severe migraines and sickness absence (an adjusted mean difference of 10.7 sickness absence days per year) is larger than the estimates in most previous epidemiological surveys, where annualized mean sickness absence days due to migraines has been 1.5–7.1 (11,40,47), although the mean associated with other frequent or severe headaches in the NCS-R (3.8) is within the range of previous surveys (48–50). The high NCS-R estimate associated with frequent or severe migraines is consistent with evidence that migraineurs who rate their headaches severe have more lost productivity than other migraineurs (5).
The annualized societal-level human capital estimated effect of sickness absence due to frequent or severe migraines, $9.3 billion, compares with estimates of $12 billion (6) and $13 billion (7) in previous US studies. Our estimate is 70–75% as large as these other estimates despite the estimated prevalence of migraine in our sample being less than half that in these other studies, reflecting the higher per-worker estimated impact of migraine in our sample of frequent or severe migraineurs. Furthermore, as noted above, this might be an under-estimate to the extent that frequent or severe migraines are associated with decrements in work performance that are not picked up by our coarse performance measure. Approximately 20% of the gross association between migraines and sickness absence was attributed to temporally primary comorbid disorders 60% to the direct predictive effects of migraines and 20% to indirect effects of migraines through temporally secondary disorders. No evidence was found that the significant predictive effect of migraines on sickness absence varies as a function of number of comorbid physical or mental disorders. We are unaware of any previous study that examined this specification.
Several limitations of the study need to be considered when interpreting the above results. First, the focus on workers with ‘frequent or severe’ headaches made it impossible to estimate the prevalence or evaluate the work impairments of all migraineurs. Furthermore, as the terms ‘frequent’ and ‘severe’ were not defined, it is impossible to characterize precisely the sub-sample of migraineurs who endorsed this diagnosis.
Second, the HPQ assessment of workplace outcomes is doubtlessly imperfect. The HPQ measure of absenteeism has been shown to be strongly correlated with independent payroll records of absenteeism (21,22), while the HPQ work performance measure is strongly correlated with independent supervisor evaluations (22) and daily diary records (21). However, these associations are less than perfect and have been validated only in the aggregate, raising the possibility of bias in self-reports that might be systematically related to the presence of headaches. As noted above, the coarse measure of average work performance might be a source of particular concern to the extent that it does not pick up impairments in work performance on days of migraines.
Third, the time frame of the key measures was not consistent (i.e. 12-month prevalence of headaches and comorbid disorders vs. 1-month prevalence of workplace outcomes). Disorders were assessed in a 12-month framework because the focus of the survey was on chronic conditions. Workplace outcomes were assessed in a 1-month framework because retrospective self-reports of these outcomes are inaccurate beyond a 1-month recall period (51). As discussed in more detail elsewhere (21,22), the associations we report consequently describe average monthly effects of having a 12-month history of frequent or severe headaches among respondents who might or might not have had headaches every month. Use of a consistent 1-month time frame would have yielded stronger associations and smaller standard errors.
Fourth, the distinction between temporally primary and secondary comorbidities should be recognized as merely a rough approximation. It is well known that cross-sectional naturalistic studies are incapable of distinguishing between explanatory variables (i.e. pre-existing comorbidities that both increase risk of headaches and independently influence work performance) and mediating variables (i.e. comorbidities that occur secondary to headaches and independently influence work performance) (52) and that data analyses making this distinction must be based on assumptions imposed on the data (53). Because of this, we are surer that 60% of the gross effect of migraines with sickness absence is independent of the comorbid conditions than that the remaining 40% of the gross effect is due 20% to temporally primary and 20% to temporally secondary comorbidities. Nonetheless, the findings that the majority of the gross effect is independent of these comorbidities and that a meaningful part of the remaining gross effect might be due to the indirect effects of migraines through secondary comorbidities are important in light of the wide recognition that the major burden of headaches is concentrated in the minority of cases that have high comorbidity (11,54).
Given the importance of comorbidity, future research should refine the distinction between temporally primary and secondary comorbidities using prospective data. Earlier studies have documented significant prospective associations between migraine and subsequent onset of panic disorder (55) and major depressive disorder (56). Such prospective studies need to be expanded to consider a wider range of physical and mental disorders and to investigate how much the prospective associations of migraine with sickness absence are mediated by secondary disorders. It would be useful to examine in this way the distinct comorbid clusters that have been documented to co-occur with migraine (12) and to conduct experimental evaluations of the effects of migraine treatments on the onset, persistence and severity of these comorbid disorders (57).
In the context of the above limitations, the results reported here suggest that efforts to detect and provide best-practice treatment to workers with frequent or severe migraines might have significant human capital benefits to employers. Such experiments have not been carried out, although a significant effect of migraine medication with triptans vs. placebo on self-reported work productivity was documented in a randomized clinical trial (58) and significant before-after reductions in sickness absence were documented in several open-label studies of migraine treatment in workplace samples (59–62). These results suggest that large-scale workplace effectiveness trials are warranted for workers with frequent or severe migraines. It is not clear if a positive employer return-on-investment (ROI) would be found in such experiments, but the estimated average annual $1165 human capital cost associated with frequent or severe migraines obtained in the NCS-R is high enough to think that even partial remediation might have a positive ROI, especially given that this estimate of human capital cost might be downwardly biased by virtue of the coarseness of our measure of work performance. More complex intervention targeting approaches, possibly aimed at interfering with illness progression (63) or at tailoring treatments based on comorbidities (64) or at providing coordinated management as well as treatment (65), might show even higher long-term ROIs. Documentation of such positive effects could be of great value in promoting the expansion of workplace migraine screening and disease management programmes to address the low detection and treatment of workers with migraines (8,9).
Footnotes
Acknowledgements
The National Comorbidity Survey Replication (NCS-R) is supported by the National Institute of Mental Health (NIMH; U01-MH60220) with supplemental support from the National Institute of Drug Abuse, the Substance Abuse and Mental Health Services Administration, the Robert Wood Johnson Foundation (Grant # 044780), and the John W. Alden Trust. Additional support for preparation of this paper was provided by GlaxoSmithKline. NCS-R investigators include Ronald C. Kessler (Principal Investigator, Harvard Medical School), Kathleen Merikangas (Co-Principal Investigator, NIMH), James Anthony (Michigan State University), William Eaton (The Johns Hopkins University), Meyer Glantz (NIDA), Doreen Koretz (Harvard University), Jane McLeod (Indiana University), Mark Olfson (Columbia University College of Physicians and Surgeons), Harold Pincus (University of Pittsburgh), Greg Simon (Group Health Cooperative), T. Bedirhan Ustun (World Health Organization), Michael Von Korff (Group Health Cooperative), Philip Wang (NIMH), Kenneth Wells (UCLA), Elaine Wethington (Cornell University), and Hans-Ulrich Wittchen (Technical University of Dresden). The views and opinions expressed in this report are those of the authors and should not be construed to represent the views of any of the sponsoring organizations and agencies, or the US Government. A complete list of NCS publications and the full text of all NCS-R instruments can be found at http://www.hcp.med.harvard.edu/ncs. Send correspondence to ![]()