
Abstract
The coronavirus disease 2019 (COVID-19) pandemic in Australia resulted in significant additional infection control precautions for consumers and the health workforce. Prior to widespread vaccine availability, substantial changes were made to the operating theatre management of patients presenting for surgery with suspected or diagnosed COVID-19. This study aimed to calculate the actual costs of operating theatre care for patients with confirmed or suspected COVID-19. Data were prospectively collected for all patients presenting for surgery with confirmed or suspected COVID-19 at the Royal Brisbane and Women’s Hospital. Information collected included patient characteristics, surgical and anaesthesia details, equipment, theatre utilisation, staffing and cleaning. The associated variable costs and usual costs of care were calculated according to the Australian National Efficient Price. We compared estimated usual costs with those estimated for patients with confirmed or suspected COVID-19. Twenty-four patients with suspected COVID-19 infection underwent surgery between May 2020 and February 2021. Cost analysis revealed a mean (standard deviation (SD), range) increase in costs of providing perioperative care for COVID-19 suspect patients of A$2252 (A$2570, A$315.85–10,398); that is, a mean of 207.5% more than usual care costs. This was primarily due to the increased number of staff and time required to complete these cases with appropriate infection control.
Keywords
Introduction
Prior to widespread access to coronavirus disease 2019 (COVID-19) vaccinations, the pandemic in Australia necessitated significant additional infection control precautions for consumers and the health workforce.1,2 COVID-19 spreads via contact and droplet transmission, and anaesthetic staff were considered to be at increased risk of exposure due to their involvement in particular airway management procedures. COVID-19 is thought to have a reproduction number (R0) of 2.0–2.5, compared with seasonal influenza, which has a R0 range of 0.9–2.1. 3 A systematic review evaluating transmission of severe acute respiratory syndrome (SARS-COV-1) to healthcare personnel in 2003 found an absolute risk increase of 10–15% for transmission of the virus compared with staff who were not exposed to aerosol-generating procedures. 4
COVID-19 was declared a pandemic by the World Health Organization on 11 March 2020. 5 Between May 2020 and February 2021, Australian hospitals implemented protocols determining how patients with suspected or diagnosed COVID-19 were managed in the operating theatre. The protocols detailed patient transport, staff requirements, personal protective equipment (PPE), room setup, cleaning, and patient recovery after anaesthesia.6 –8 These procedures changed the way operating theatre teams delivered patient care.
In 2020, to address the additional costs of caring for patients with COVID-19, the federal and state governments of Australia negotiated new health funding arrangements. 9 An upfront advance payment of A$100 m was divided between the states and territories, proportionate to population. In addition, there was an increase from 45% to 50% in the federal contribution made toward the cost of hospital care for patients with confirmed or suspected COVID-19. In 2021, the Australian health financing systems implemented more specific and clear funding for treating patients with COVID-19. 10
The significant costs of delivering usual care to patients with COVID-19 have only recently been acknowledged by the Australian Federal Government. 11 An understanding of the real costs of delivering care to patients with confirmed or suspected COVID-19 disease is now emerging, through the Activity-Based Funding data systems and the Pricing Framework for Australian Public Hospital Services 2022–23 consultation process. 12 A retrospective Australian study suggested an increase in postoperative complications, length of hospital stay and intensive care unit (ICU) admissions, resulting in an overall increase in hospital costs. 13
There are few true cost analyses conducted in the Australian context regarding the cost of delivering usual patient care to inform the Australian public hospital funding policy. Understanding the funding required to implement COVID-19 operating theatre protocols is important for interpreting healthcare performance during the COVID-19 pandemic as well as planning for future pandemics. We aimed to describe the cost of anaesthetic management of patients with suspected or diagnosed COVID-19. We calculated the costs associated with operating theatre management and compared them with the estimated costs for patients without COVID-19.
Methods
Ethical approval was obtained from the Royal Brisbane and Women’s Hospital (RBWH) Human Research Ethics Committee (LNR/2020/QRBW/63673). Data were prospectively collected between 1 May 2020 and 28 February 2021 relating to all patients with confirmed or suspected COVID-19 infection and presenting for care by anaesthesia staff in the operating theatre complex at the RBWH. The RBWH is a major tertiary hospital in Queensland, Australia and provides care to adult and obstetric patients for all services other than cardiac and transplant surgery. It is the largest hospital in Australia, performing 27,500 surgical interventions annually. 14
Patients were identified by anaesthesia or nursing staff following booking with surgical services. At the time of this study, COVID-19 diagnosis was defined as a patient with a documented nasal or oropharyngeal swab testing positive by polymerase chain reaction (PCR) testing for COVID-19. Rapid antigen tests were not widely available. Patients who were suspected of having COVID-19 were defined according to local criteria at the time, based on epidemiological and clinical criteria (online Supplementary material Table 1). 15
Patient characteristics, COVID-19 testing results and surgical details of the 24 COVID-19 suspect patients requiring surgical and anaesthesia care at the Royal Brisbane and Women’s Hospital.
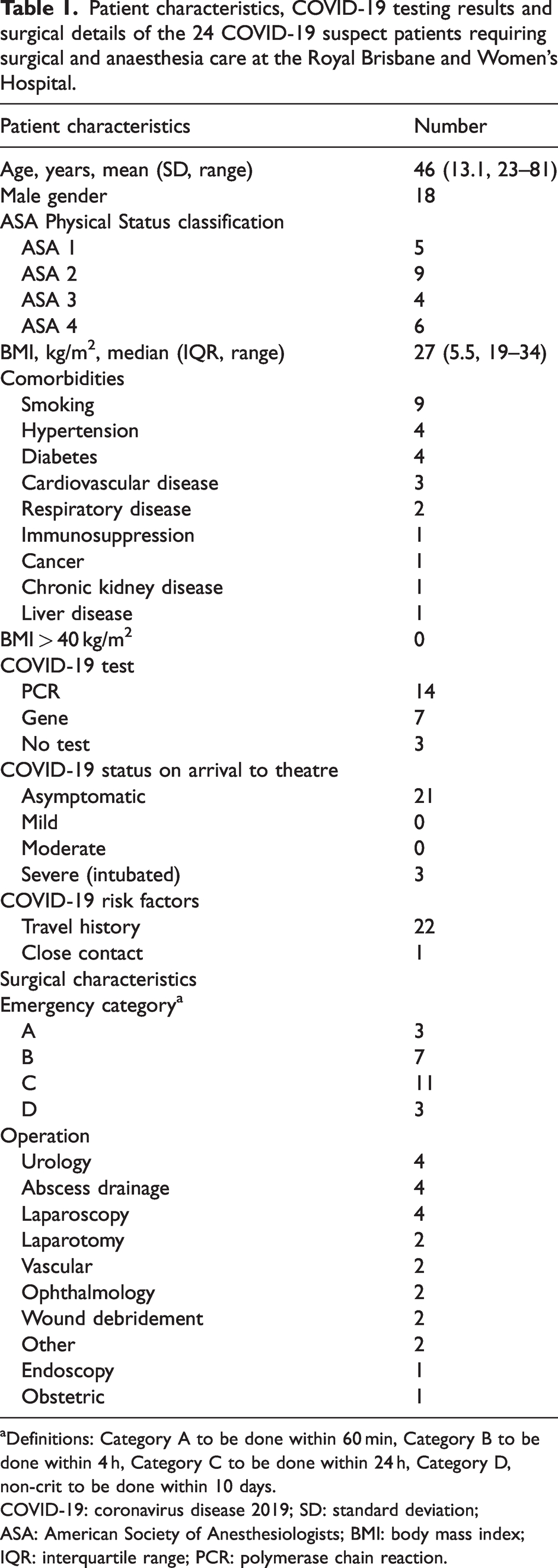
Definitions: Category A to be done within 60 min, Category B to be done within 4 h, Category C to be done within 24 h, Category D, non-crit to be done within 10 days.
COVID-19: coronavirus disease 2019; SD: standard deviation; ASA: American Society of Anesthesiologists; BMI: body mass index; IQR: interquartile range; PCR: polymerase chain reaction.
Local COVID-19 protocols and guidelines at the time mandated that patients entered the operating theatre directly, without entering the induction rooms. Strict donning and doffing procedures and additional staff ‘runners’ outside the operating theatre were required. Anaesthesia protocols recommended airway management with a plastic barrier sheet between the anaesthetist and patient, and modified rapid sequence induction with endotracheal intubation performed by the most senior anaesthetist. Recovery staff entered the operating theatre following the end of anaesthesia care to provide post-anaesthesia care. 7
Patient characteristics and demographics were documented including age, gender, body mass index, American Society of Anesthesiologists Physical Status Classification and presence of comorbidities. Details of PCR testing, presence and severity of COVID-19 symptoms, travel history and occupation were obtained. Surgical details included the name of the procedure and the urgency category (A–D: Category A to be done within 60 min, Category B to be done within 4 h, Category C to be done within 24 h, Category D non-critical to be done within 10 days). The time of day was categorised as ‘in hours’ if it was commenced between the hours of 07:30 and 18:00 and the location was categorised as ‘dedicated COVID-19 theatre’ or other. Anaesthesia details included type of anaesthesia (sedation, general anaesthesia, regional anaesthesia or a combination of these), airway management (rapid sequence or standard induction, endotracheal tube, supraglottic airway, Hudson mask, nasal prongs, no additional oxygen, airway adjuncts, and videolaryngoscopy), extubation management, complications during intubation or extubation, and equipment problems. The type of PPE used and whether donning and doffing ‘spotters’ were present was recorded. Hospital length of stay was measured in days and where appropriate the number of days in ICU was recorded as per the Australian and New Zealand Intensive Care Society Adult Patient Database definitions for admission and discharge. 16
Detailed theatre utilisation and timing were recorded; this included anaesthetic assessment time (patient arrival to anaesthetic monitoring/procedures started), knife-to-skin (KTS) time (anaesthetic start time to KTS), anaesthesia time (anaesthetic start time to patient extubated or ready for recovery), surgical time (KTS to surgical completion), anaesthesia recovery time (patient extubated to recovery nurse arrival), recovery time (recovery nurse arrival time to patient left theatre) and total time patient in theatre (patient arrival to patient left theatre). During the study period the recovery process evolved to having recovery staff remain outside the operating theatre until 20 min post-extubation. This allowed multiple room volume air exchanges to reduce the airborne viral load within the theatre. Theatres were then quarantined until a thorough COVID-19 decontamination clean took place with cleaning staff donning full PPE. The number and category of staff involved (anaesthetic consultant or registrar, anaesthetic assistant, surgical consultant or training registrar, resident medical officer, scrub nurse, scout nurse, theatre orderlies and additional nursing or allied health staff), patient recovery and postoperative care were documented.
Data were recorded in a secure online database. The age and gender of patients who were provided with anaesthesia care in the operating theatre during the data collection period (but not included in our cohort) were compared with the age and gender of included patients to assess for bias.
Data collection was ceased after a 10-month period in February 2021 due to an extended period of zero cases of community transmission of COVID-19 cases in Queensland due to ongoing border closures, strict quarantine requirements for travellers and city-wide lockdowns to control outbreaks. This coincided with COVID-19 vaccine distribution in Queensland which began on 22 February 2021. 17
Cost analysis
Data were collected on variable costs and staff salary costs. Hospital costs are either fixed or variable, and categorising costs depends on the setting. Fixed costs include buildings, equipment and some salaried labour costs, items which the hospital still needs to pay for in the short term whether a patient is occupying a bed or not. Variable costs are those that change with output and can be saved by the hospital if a service is not provided. 18 For this study, we categorised staff salary costs as a variable cost, as we were interested in costs attributed to activity that could be shifted within the department. The staffing costs calculated were virtual for each COVID-19 case as no additional staff were employed by the health service.
To determine the additional costs of caring caring for confirmed and suspected COVID-19 patients in the perioperative setting, the usual care costs were established for each patient. The Australian Refined-Diagnosis Related Group classification version 10.0 (AR-DRG V10) 19 was identified for each patient, and a ‘usual care’ price for each DRG was determined. The 2021–2022 Australian National Efficient Price of A$5597 was adjusted according to the relevant price weights 10 to establish a full cost per weighted case for an average length of stay. This cost was further adjusted to exclude postoperative care costs.
Surgical and anaesthetic procedure-level costs for non-COVID-19 patients (‘usual care’) were determined by assuming conservatively that 16% of full costs per weighted case are true variable costs, 2.5% of these costs are to operate theatres, and 45.7% can be attributed to the salary of healthcare professionals delivering patient care. 18 The cost for a single day of care, rather than the full cost, was determined by dividing the variable cost proportion by the average length of stay. This is an established method as hospital costs remain fairly constant over the duration of a patient’s stay. 20
The usual care costs were then compared with the costs of surgery for patients included in this study who had confirmed or suspected COVID-19. Salary costs for each episode were determined from the number of staff, their roles and the amount of time taken to deliver patient care. Assuming salary costs account for 45.7% of the total cost of patient care, an adjustment was then applied to calculate the total cost of looking after each suspected COVID-19 episode of care. The cost of PPE consumables for each staff member in attendance was added to the total cost of caring for COVID-19-suspect cases.
Statistical analysis
Descriptive statistics were used; continuous variables are reported as mean and standard deviation (SD), and categorical variables are reported as frequencies and percentages. Age and gender of the sample were compared with the rest of the population cared for during the same time period based on data extracted from the Operating Room Management Information System. Statistical analysis was performed using the t-test for continuous variables, and the chi-squared test for categorical variables. P-values of <0.05 were considered statistically significant.
Results
Patient characteristics
Twenty-four cases were recorded during the study period and all were included for analysis. The characteristics of the patients are listed in Table 1. There was no statistically significant difference in age or gender between the cohort of patients without COVID-19 (n = 19,862) or suspected COVID-19 (n = 24) treated during the study period. The mean (SD, range) length of stay was 20.2 (26.0, 1.9–63.9) days and number of days in ICU was 5.9 (3.2, 1.1–7.9) and there was no mortality related to COVID-19 in this cohort.
COVID-19 testing
Twenty-one (88%) patients with suspected COVID-19 were tested prior to attending the operating theatre (Table 1). Three (12%) patients were not tested for COVID-19 prior to presenting for theatre and were managed as suspected COVID-19, based on clinical criteria. All patients included in the cohort subsequently tested negative for COVID-19 infection.
Anaesthesia and surgery
Twenty-four patients underwent emergency surgical operations. Four (17%) patients had laparoscopic surgery, two (8%) cases involved major surgery in a single patient with necrotising fasciitis, two cases involved major vascular surgery (Table 1). General anaesthesia was administered in 18 (75%) of the cases, neuraxial anaesthesia in four (17%) and regional anaesthesia in three (13%), including a femoral nerve block administered in combination with general anaesthesia. Full details relating to airway management, ventilation and reported process problems are listed in Table 2.
Anaesthesia characteristics of the 24 COVID-19 suspect patients requiring surgical and anaesthesia care at the Royal Brisbane and Women’s Hospital.
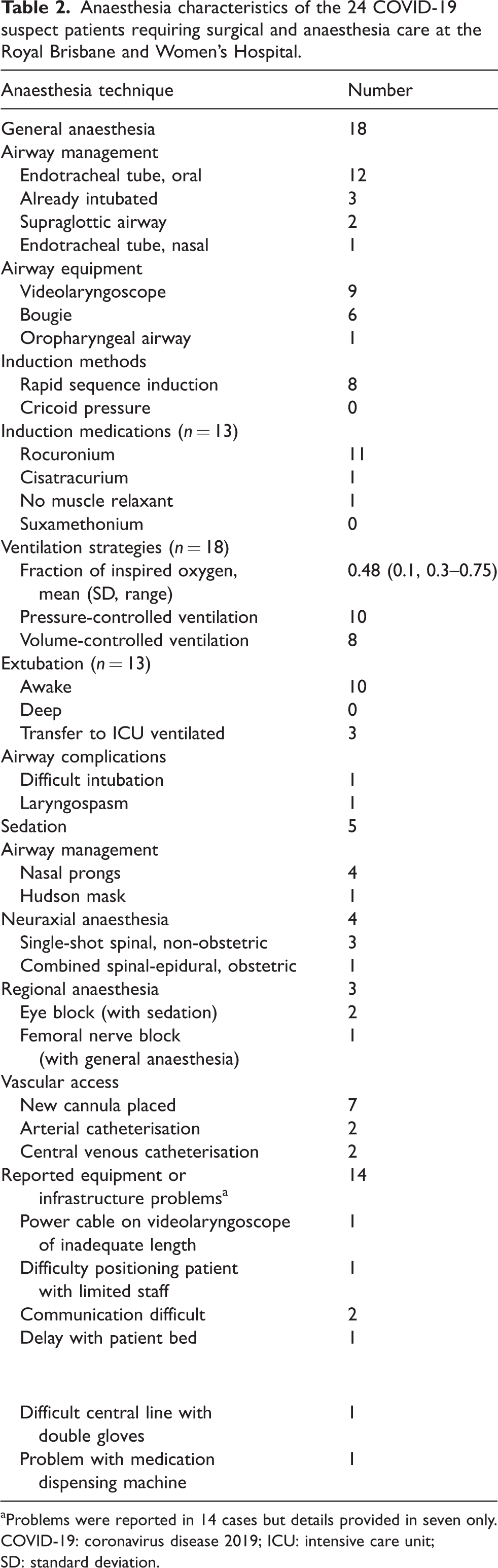
Problems were reported in 14 cases but details provided in seven only.
COVID-19: coronavirus disease 2019; ICU: intensive care unit; SD: standard deviation.
Staff
A consultant anaesthetist was present in 21 (88%) cases. A second anaesthetic medical officer (consultant or registrar) was available to assist in 19 (79%) cases. An anaesthetic assistant was present in theatre for 22 (92%) cases and a second assistant was available for 21 cases (88%). A consultant surgeon was in attendance for 14 (58%) cases and a surgical registrar was the most senior proceduralist in the remaining 10 cases (42%). One case necessitated the attendance of an interventional radiologist to place a nephrostomy tube.
PPE
In all cases, double gloves, N95 face mask, protective gown and hairnet were worn by all anaesthetic staff. A face shield was used in 20 (83%) cases, and eye goggles alone in the remaining four (17%) cases. Six (25%) cases utilised a plastic sheet over the patient’s head during airway management. Twenty-three (96%) cases had a dedicated spotter during donning of PPE, with 21 (88%) having a spotter during doffing. Four cases reported concerns over PPE equipment. Two cases (8%) reported no availability of a correctly fitted N95 mask. Table 3 lists the details of theatre utilisation for the 24 cases. The mean (SD, range) surgical time was 69.8 (60.1, 8–223) min and total anaesthetic time was 113.3 (69.2, 31–311) min.
Theatre time utilisation for 24 COVID-19 suspect patients requiring surgical and anaesthesia care at the Royal Brisbane and Women’s Hospital.
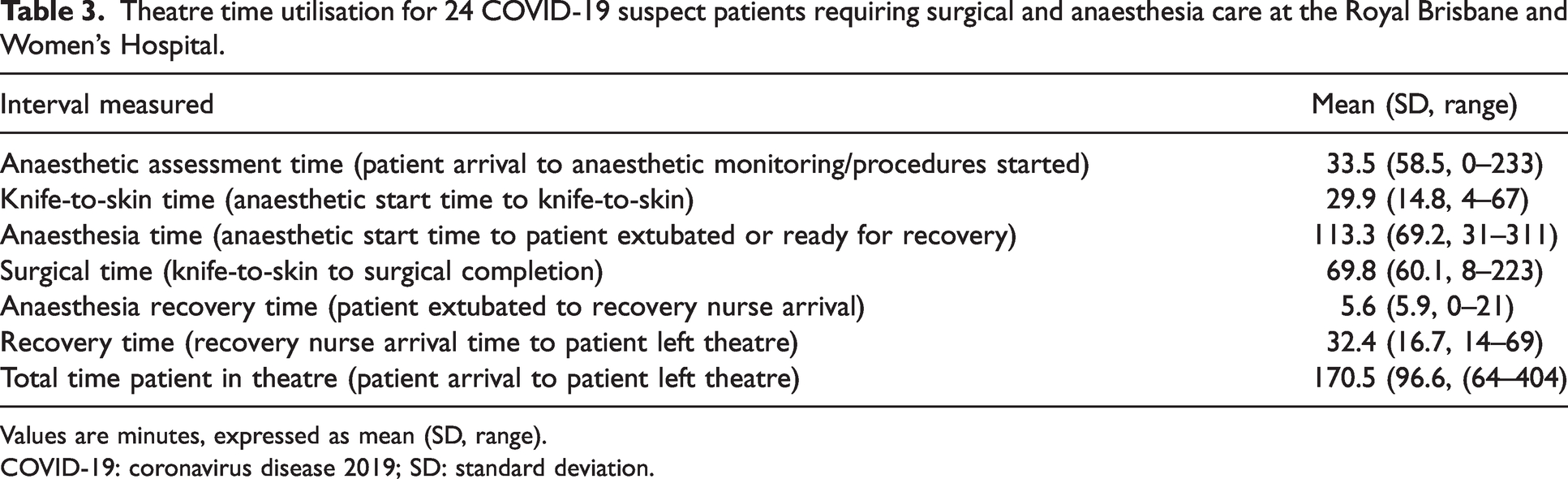
Values are minutes, expressed as mean (SD, range).
COVID-19: coronavirus disease 2019; SD: standard deviation.
Cost analysis
The cost analysis is presented in Table 4. The mean (SD, range) increase in costs of providing perioperative care for COVID-19 suspect patients was A$2252 (A$2570, A$315.85–10,398). This equated to a 207.5% average increase in cost, which was contributed to by additional staff requirements and provision of PPE. Two patients were identified as requiring lower than usual care costs. One case was a removal of misplaced central line from the carotid artery. The patient was already intubated and had a short procedure and anaesthetic time. The second case was an uncomplicated laparoscopic appendicectomy in a healthy patient with a high-risk travel history and clinical care was provided afterhours by less senior staff. Cases that had the greatest impact on cost of care were more complex surgical patients requiring intensive care transfer and additional senior staff.
Comparison of the cost of surgical and anaesthetic care for non-COVID-19 patients (‘usual care’) versus COVID-suspect patients for each operation at the Royal Brisbane and Women’s Hospital.

Values are in Australian dollars (A$).
COVID-19: coronavirus disease 2019; AR-DRG V10.0: Australian Refined Diagnosis Related Groups classification version 10.0; W GIs: with gastrointestinal surgery.
Discussion
The operating theatre costs for caring for COVID-19 patient during the pandemic were more than two times that of usual care. This amounted to a mean additional cost of A$2252. These costs were driven largely by additional staff requirements and lengthy operating theatre preparation and recovery times. Senior anaesthesia staff were present for nearly all cases and compliance with PPE was high.
The COVID-19 pandemic caused disruption and profound uncertainty to the delivery of surgical services, which had significant implications to the delivery of healthcare. At the Royal Brisbane and Women’s Hospital, the implemented protocols delayed theatre start times and monopolised a number of staff members, whilst waiting for patients to enter the operating theatre. Additional staff members were not employed to provide perioperative care; however, COVID-19 protocols resulted in the cancellation of elective surgery and deployment of staff members to other areas of healthcare delivery. While PPE guidance and compliance was high, the use of higher-level PPE is likely to have contributed to delays in commencing surgery. Senior anaesthesia staff were present in over 90% of cases, compared with senior surgical staff, who were present in 63% of cases. Two cases (8%) were performed without an anaesthetic technician within the theatre in full PPE for the duration of the case. Although they were involved in preparation and present immediately outside the theatre, they were not included in costings.
Testing for COVID-19 has evolved. During the study period, PCR testing was gold standard. These assays required complex laboratory equipment and trained technicians and took several hours. Typically, anaesthesia care was required prior to receiving the result. In addition, due to local policies, patients were still treated as suspected COVID-19 for 14 days despite a negative test, requiring full compliance with infection control protocols in the operating theatre.
Aggressive workflow modifications were introduced into the hospital in recognition of the danger to anaesthesia staff of being exposed to a large inoculum of COVID-19 virus during aerosol-generating procedures. Strategies to prevent infection of healthcare workers included fit-testing of N95 masks for all staff. In addition, those involved in the perioperative management of COVID-19 suspected patients were required to participate in an arduous process of donning enhanced PPE followed by a demanding decontamination doffing sequence under the watchful eye of a trained colleague to ensure correct compliance. The low case numbers and limited community transmission also allowed time to adopt lessons from colleagues around the world to mitigate against contaminating healthcare providers, minimising healthcare worker infection with COVID-19 prior to the widespread access to vaccinations.
Limitations of this study include the small sample size, with data collected during a period of time in which the management of the pandemic continued to change and evolve. It is likely that there were additional cases cared for that were missed during the data collection period. Our results are from a single centre and are not generalisable to other institutions. There was on average only one COVID-19 suspect case per surgical category therefore the results may not be representative of the larger surgical cohort. Usual care costs were calculated based on the DRG identified for each presentation and the National Efficient Price Determinations to establish a full cost per weighted case. The average length of stay was then used to calculate the cost of a single day of care. This method may underestimate the usual care costs of operating theatre care during which time patients require increased staffing and resources to facilitate their surgical procedure. We have not considered the costs related to other patients who had their care delayed or cancelled due to re-allocation of staff and resources to care for COVID-19 suspect patients.
Whilst a number of staff were redeployed to frontline services during the pandemic, the reduction in elective surgery allowed more surgical and theatre staff to be available for treating COVID-19 positive or suspect patients. As such the increased staffing costs and salary estimates are a virtual representation as opposed to additional true costs to the hospital and health service. These virtual staffing costs are valid as the extra staffing required for the additional cost COVID-19 cases required postponements and cancellations of elective surgical cases. Cancelling elective surgery ultimately results in additional costs to the health service owing to a reduction in activity-based funding that the hospital receives, and through later patient presentations which may lead to more complex and lengthy surgical procedures.
Our single-centre study fills a gap in identifying and detailing the additional costs associated with the delivery of surgical services to patients with confirmed or suspected COVID-19. Our data were collected early in the pandemic prior to the influx of COVID-19 positive patients into our hospital and respiratory ward. Our study does not aim to determine the cost of treating COVID-19 patients as a proportion of the total operating budget. The comparison of costs against usual care during the early phases of the pandemic aims to highlight the increased resources and personnel required to adhere to important infection control practices. Whilst the anaesthetic management costs were increased compared with usual care, there were only 24 COVID-19 cases treated amongst a total surgical population of 19,000 during the 10-month period. Thus, the total additional costs were relatively small as a proportion of the total anaesthetic expenditure during the study period. The results are still relevant, however, as they can be used in planning for future pandemics and to guide future health funding agreements to address shortfalls in hospital funding.
Our institution demonstrated that to maintain high quality care whilst minimising infection risk to personnel, patients treated under COVID-19 precautions required additional and more senior staff, and longer operating times. The 207.5% increase in cost of operating theatre care calculated in this cohort of COVID-19 positive and suspect patients suggests that the federal government funding increase from 45% to 50% provided early in the pandemic was insufficient to cover the cost of increased staff and resources. This cost analysis presents challenges to government departments for planning and preparing for future pandemics.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X241272108 - Supplemental material for A cost analysis of the anaesthetic management of patients with confirmed or suspected coronavirus disease 2019 (COVID-19) in a tertiary referral hospital in Queensland, Australia
Supplemental material, sj-pdf-1-aic-10.1177_0310057X241272108 for A cost analysis of the anaesthetic management of patients with confirmed or suspected coronavirus disease 2019 (COVID-19) in a tertiary referral hospital in Queensland, Australia by Anthony T Hodge, Angela R Tognolini, Elizabeth K Martin and Victoria A Eley in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.