
Abstract
Air-purifying full-face masks, such as military chemical–biological–radiological–nuclear masks, might offer superior protection against severe acute respiratory syndrome coronavirus 2 compared to disposable polypropylene P2 or N95 masks. In addition, disposable masks are in short supply, while military chemical–biological–radiological–nuclear masks can be disinfected then reused. It is unknown whether such masks might be appropriate for civilians with minimal training in their use. Accordingly, we compared the Australian Defence Force in-service chemical–biological–radiological–nuclear Low Burden Mask (AirBoss Defense, Newmarket, Canada) with polypropylene N95 masks and non-occlusive glasses worn during simulated tasks performed by civilian clinicians in an Australian tertiary referral hospital intensive care unit. After brief training in the use of the Low Burden Mask, participants undertook a simulated cardiac arrest scenario. Previous training with polypropylene N95 masks had been provided. Evaluation of 10 characteristics of each mask type were recorded, and time to mask application was assessed. Thirty-three participants tested the Low Burden Mask, and 28 evaluated polypropylene N95 masks and glasses. The Low Burden Mask was donned more quickly: mean time 7.0 (standard deviation 2.1) versus 18.3 (standard deviation 6.7) seconds; P = 0.0076. The Low Burden Mask was rated significantly higher in eight of the 10 assessed criteria, including ease of donning, comfort (initially and over a prolonged period), fogging, seal, safety while removing, confidence in protection, and overall. Visibility and communication ability were rated equally highly for both systems. We conclude that this air-purifying full-face mask is acceptable to clinicians in a civilian intensive care unit. It enhances staff confidence, reduces waste, and is likely to be a lower logistical burden during a prolonged pandemic. Formal testing of effectiveness is warranted.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was originally believed to spread only through the inhalation of virus-laden liquid droplets (greater than approximately 5 µm) expelled from the respiratory passages of infected patients, 1 as well as contact with contaminated surfaces on which the virus has been demonstrated to remain infective for up to 72 hours. 2 However, reports of aerosol particles (less than approximately 5 µm) containing SARS-CoV-2 1 along with likely aerosol patient transmission 3 have led some to question the effectiveness of government recommendations 4 that require only droplet precautions when treating patients infected with SARS-CoV-2, reserving airborne personal protective equipment (PPE) for a defined list of aerosol-generating procedures. In Australia, adequate airborne precautions are defined as an Australian and New Zealand Standard AS/NZS 1716 P2 mask (filtering 0.3–0.6 µm particles, similar to the United States (US) N95 standard), in addition to non-occlusive plastic glasses, a long-sleeved fluid-impervious gown and disposable gloves. No head covering or face shield is mandated. Of the 3599 Victorian healthcare workers infected with COVID-19, 73% were acquired in a healthcare setting. 5 Similar guidelines were recommended in Spain, 6 where 13.6% of the country’s doctors became infected with SARS-CoV-2. 7 In a US study of 51 healthcare workers, more than one-third failed a ‘fit test’ of their N95 mask, with more failures associated with extended use or reuse. 8 While there is no evidence that higher levels of protection against aerosol transmission, such as fully occlusive face coverings, reduce the incidence of SARS-CoV-2 transmission to healthcare workers, the Australian Society of Anaesthetists, quoting transmission rates of up to 10% using N95 masks, has stated that full-face protection with, for example, a powered air-purifying respirator (PAPR), ‘may have advantages over N95’. 9 Even if affording no greater protection during wear, the combination of eye and respiratory protection is more convenient, potentially quicker to apply and safer to remove. In addition, although disposable PPE is usually routine practice in developed countries, the SARS-CoV-2 pandemic has led to worldwide shortages, 10 making it unlikely that current recommendations will always be met, even in the developed world.
Under the circumstances described, reusable PPE providing full-face protection that is designed for extended use could be highly desirable. This might be especially true in circumstances in which the resupply of PPE is difficult or impractical, such as in remote communities or developing nations affected by SARS-CoV-2. Several military and industrial air-purifying masks are available, but few have been tested in clinical situations among civilian staff without prior training in their use. Accordingly, we sought to test whether the current in-service Australian Defence Force chemical–biological–radiological–nuclear (CBRN) air-purifying mask could be employed in a civilian hospital, and to evaluate how it compared to standard disposable airborne PPE currently in use in this environment.
Materials and methods
Permission to conduct the study was granted by the Executive Director of Medical Services and the director of the intensive care unit (ICU) at the Royal Brisbane and Women’s Hospital. This is considered an acceptable level of ethical review by the Australian National Health and Medical Research Council National Statement on Ethical Conduct in Human Research 2007 (updated 2018) for low-risk research. No patients were involved and no personal data were collected so the study did not fall within the responsibility of the hospital human research ethics committee.
Participants were civilian nursing, medical and allied health staff of the Royal Brisbane and Women’s Hospital ICU, a 36-bed multidisciplinary ICU within the largest public hospital in Queensland (comprising 929 acute care beds). Evaluation sessions were held at the end of the morning nursing shift, with any interested person invited to attend. No compulsion was attached to this invitation and no nominal roll was taken. At the conclusion of the initial briefing in each session, all participants were asked if they were willing to continue with the practical evaluation. Continued participation was taken to mean consent.
Masks
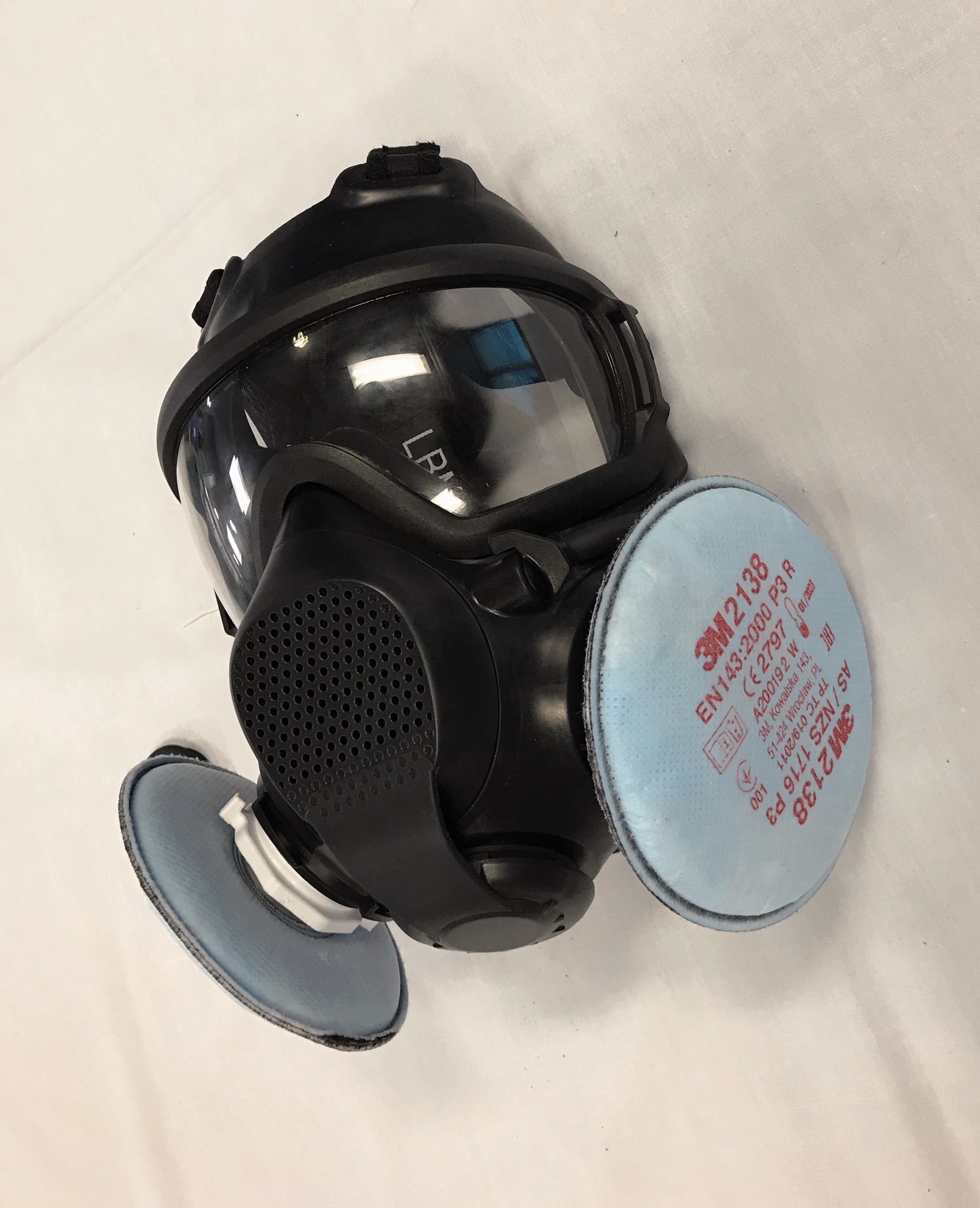
The current in-service Australian Defence Force CBRN air-purifying mask is the Low Burden Mask (LBM) (AirBoss Defense, Newmarket, Canada) (Figure 1).

Airboss Low Burden Mask fitted with military chemical–biological–radiological–nuclear (CBRN) filter (AirBoss Defense, Newmarket, Canada).
The LBM has a single panoramic visor, designed to improve vision compared to the earlier bi-ocular S10 mask (Avon Rubber, Melksham, UK); a voice modulator that improves communication in comparison with many industrial masks; and can be fitted with either PAPR or self-contained breathing apparatus attachments, or used in a negative pressure mode. Only the negative pressure configuration was used for this study. All four sizes were available for the trial. The CBRN filters used were the Scott Pro2000 CFR 22 filter (Scott Health and Safety, Skelmersdale, UK) which, when combined with a full-face respirator, meet the requirements specified by AS/NZS 1716 for P3 protection, 11 a higher level of particulate filtering than the N95 standard, and considered sufficient protection against the inhalation of airborne virus. For each participant, masks were either newly removed from the shipping packaging, or had been cleaned using a 1:1000 solution of sodium hypochlorite/calcium hypochlorite, according to Australian Defence Force guidelines. Sodium hypochlorite is known to be an effective viral disinfectant for reusable respirators, 12 and has been shown to have specific effectiveness against SARS-CoV-2. 13 A new CBRN filter was used for each participant. The LBM can be fitted with corrective vision spectacle inserts made for the individual wearer, but these were not available for the trial.
The comparison masks were a mixture of Proshield N95 masks (BSN Medical, Mount Waverley, Victoria, Australia), and Halyard Fluidshield 3 N95 masks (Halyard Health, Milsons Point, New South Wales, Australia), worn either with the participants’ own corrective spectacles (as is usual hospital practice) or disposable plastic glasses from various manufacturers.
Training
Initial training on the use of the LBM for study staff was provided by Australian Army CBRN specialists. Drawing on this, study staff then gave participants an approximately 15 minute briefing on the essential characteristics of the LBM that would be used in the clinical environment, focusing on sizing, leak testing, safe removal without contamination and adjustment for comfort. Training points with primarily military applications, such as donning and filter exchange in a contaminated environment, and use of the drinking straw, were omitted. Training on the polypropylene N95 masks had been provided to all clinical staff over the preceding 10 weeks, and most had worn these mask/glasses ensembles for extended periods while treating ICU patients infected with SARS-CoV-2.
Study procedure
Participants engaged in a simple cardiac arrest scenario using a SimMan 3G (Laerdal Medical, Stavanger, Norway) while observed by one of the study staff nurse educators, taking the roles of chest compressions, airway (intubating the SimMan device if appropriate for their profession) and team leader. They wore the mask for the entire evaluation, lasting approximately 30–40 minutes. A subset of participants was timed in their application of both types of PPE at the start of the cardiac arrest scenario.
Statistical analysis
Data were assessed for normality and compared using parametric or non-parametric statistics as appropriate. The mean difference in the time to apply masks was compared using a paired t-test, and the effect of profession on this result was assessed using linear regression with only mask type and profession as predictors. Evaluations of 10 aspects of each mask type were recorded on Likert scales on de-identified paper forms. Responses on these Likert scales were compared using Mann–Whitney U tests and additionally (for subjects in whom paired evaluations were available) in paired analyses in which each aspect of both masks was categorised as better/worse/the same by each participant. All statistical analyses were performed using Stata 16.0 (StataCorp, College Station, TX, USA).
Qualitative analysis
Free-text comments were sought from all study participants. These were categorised as either positive, negative, or neutral but nonetheless informative. Representative comments, in proportion to those expressed in each of these categories, are presented verbatim.
Assessment of modifications to allow commercial filters
An exploratory engineering study was undertaken to assess whether the LBM could be modified to use commercially available P3 industrial filters.
Results
All potential participants who attended the initial briefing consented to continue with the practical component of the study. Thirty-three participants tested the LBMs, and 28 reported experience with the polypropylene N95 masks and glasses. Of the 33 who tested the LBMs, 66% were registered nurses, 29% were doctors (including registrars and consultant intensivists) and 6% were allied health professionals. Twenty-seven participants evaluated both masks, allowing a paired comparison of this subset of study subjects to be performed.
The mean time taken to don the LBM mask was less than half that of the polypropylene N95 mask and glasses (7.0 (standard deviation 2.1) versus 18.3 (standard deviation 6.7) seconds, n = 7, 7; P = 0.0076). Profession was not a significant predictor of this result.
Table 1 shows that participants rated the LBM significantly higher in eight of the 10 assessed criteria, including ease of donning, comfort (initially and over a prolonged period), fogging, seal, safety while removing, confidence in protection against SARS-CoV-2 and their overall assessment. There was no difference in visibility and communication ability, which were rated highly for both systems. In the qualitative paired analyses (Figure 2), these same criteria were assessed as superior for the Defence masks. Overall, 18/27 (67%) would prefer to use the LBM for clinical tasks, five out of 27 (19%) had no preference and four out of 27 (15%) would prefer to use the polypropylene N95 masks.
Results of the subjective analysis of various mask characteristics.
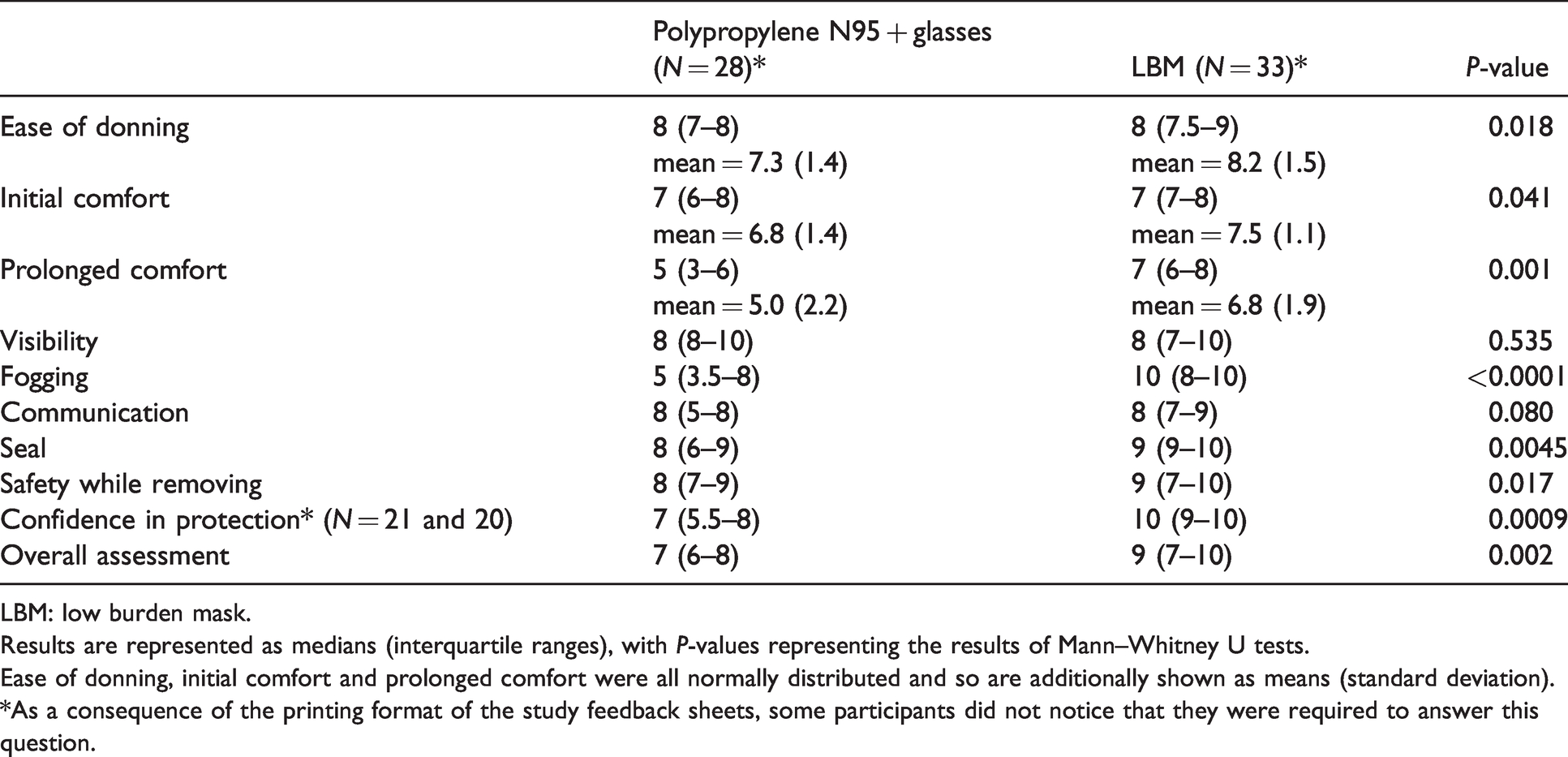
LBM: low burden mask.
Results are represented as medians (interquartile ranges), with P-values representing the results of Mann–Whitney U tests.
Ease of donning, initial comfort and prolonged comfort were all normally distributed and so are additionally shown as means (standard deviation).
*As a consequence of the printing format of the study feedback sheets, some participants did not notice that they were required to answer this question.
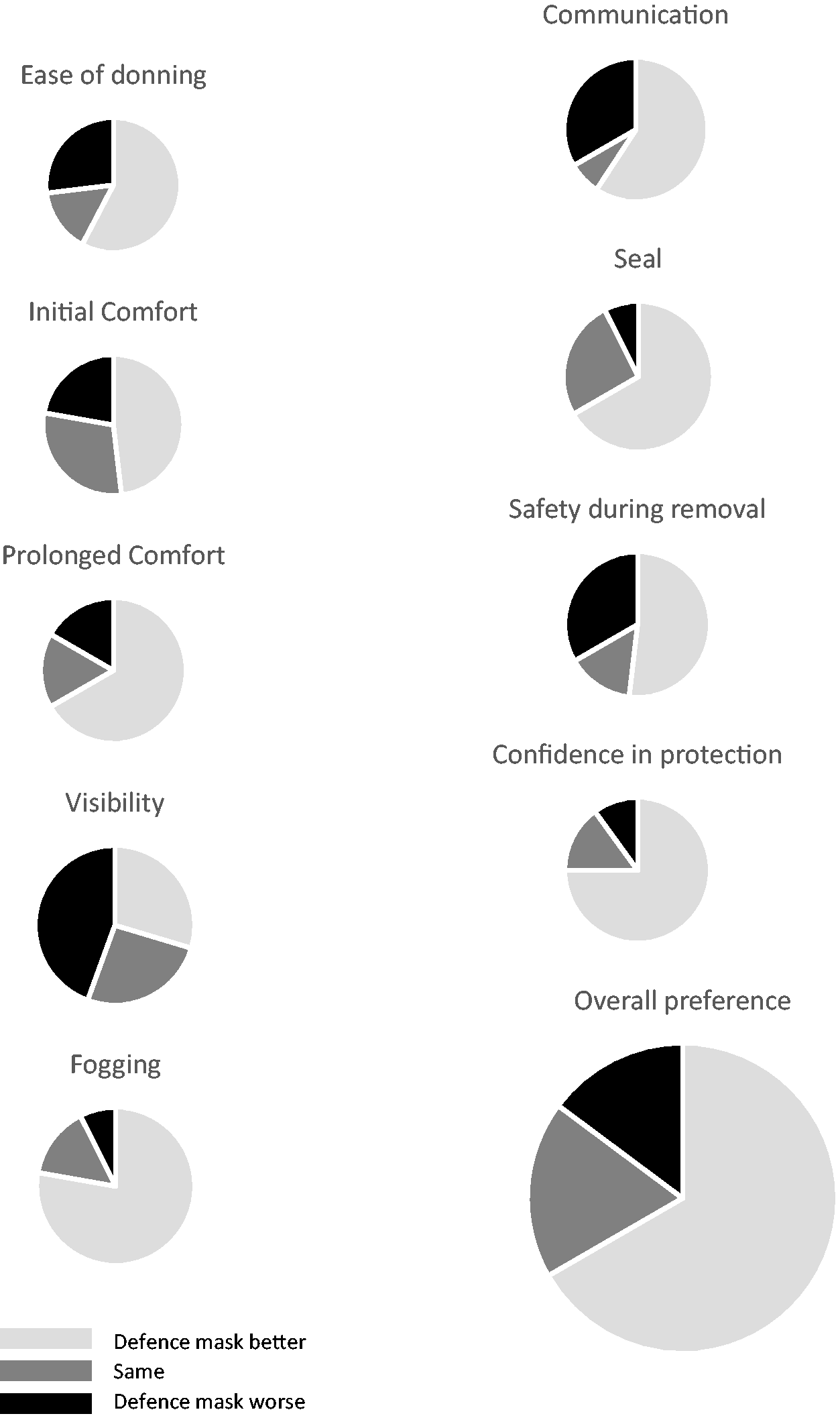
Paired analyses of 10 aspects of mask performance (n = 27 pairs).
Fourteen participants expressed free-text comments, of which nine were positive towards the LBM and five negative. Of these, positive comments included ‘I felt so much safer in the Defence mask’, ‘the military CBRN mask was more comfortable if wearing for a prolonged period’, ‘the Defence mask spreads pressure over the whole face so was more comfortable’ and ‘the polypropylene N95 mask moves during use, risking losing the seal, and is less comfortable during a 7 hour shift’. Negative comments included ‘the military CBRN mask was heavy because of the filter, which also restricted movement of the head to the left’ and ‘the Defence mask made it harder to hear each other during cardiopulmonary resuscitation’, although this last view was contradicted by others.
It was possible to achieve a tight seal between the 40 mm North Atlantic Treaty Organisation (NATO) screw connector for the cartridge filter on the LBM and a commercially available, substantially lighter P3 filter (Figure 3) using a three-dimensional (3D) printed adaptor made using freely available specifications (www.thingiverse.com/thing:4245358) (Figure 4). It was necessary to interpose a silicone washer between the hard plastic adaptor and the butyl rubber mask to optimise the quality of this seal (Figure 5). The integrity of this seal appeared tight, but the study participants did not provide their opinions on the mask in this configuration. Formal testing would be required to ensure that the filters and mask would perform as intended, and that the 3D printed component was sufficiently robust for clinical use and repeated cleaning.
Commercially available 3M 2138 P3 filters (3M Australia, North Ryde, New South Wales) fitted to the Low Burden Mask (LBM) (AirBoss Defense, Newmarket, Canada) using locally three-dimensional (3D) printed adaptors.

Three-dimensional (3D) printed connector to adapt the 40 mm North Atlantic Treaty Organisation (NATO) fitting on the Low Burden Mask for a commercial 3M filter (3M Australia, North Ryde, New South Wales).
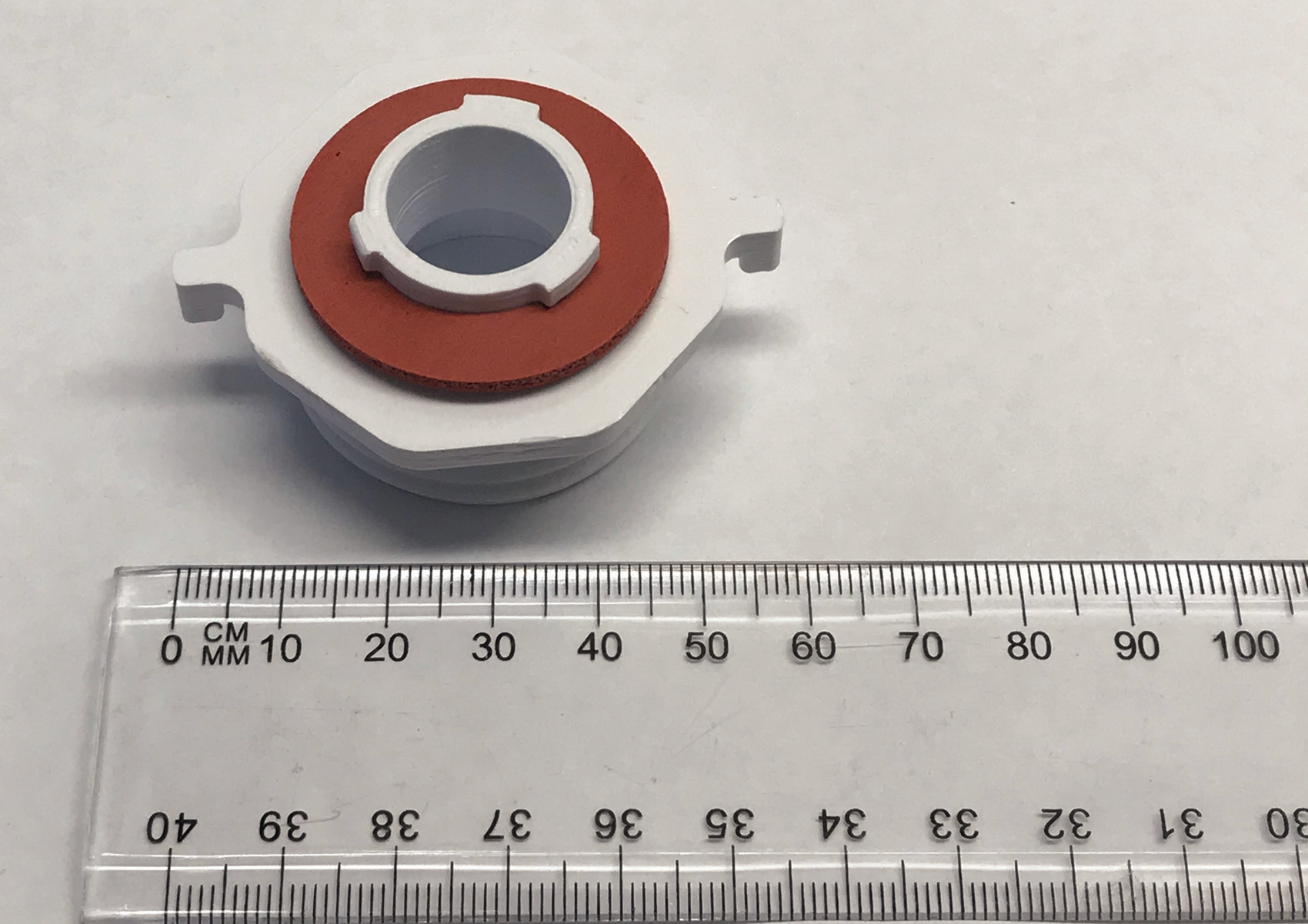
Silicone washer fitted to three-dimensional (3D) printed connector, enhancing the seal with the 3M 2138 P3 filter (3M Australia, North Ryde, New South Wales).
Discussion
This study has demonstrated that the current in-service Australian Defence Force military CBRN mask can be used by civilian ICU clinical staff after minimal training to undertake complex clinical tasks. They preferred it to the PPE currently available for use in their hospital. They applied it more rapidly, had greater confidence that it would protect them against the transmission of SARS-CoV-2, and thought that it would be more comfortable to wear over a prolonged period by the bedside of an ICU patient during an entire shift. The LBM can be cleaned to Defence standards using materials commonly available in any public hospital.
Previous investigators have studied the performance of clinical tasks while wearing military CBRN PPE. Castle et al. 14 used the full ensemble of CBRN PPE employed by the UK civilian National Health Service in a simulation study involving 66 paramedic students. CBRN PPE significantly slowed the process of intubation and reduced the overall success rate. No device achieved 100% success, even after attempts lasting 150 seconds. However, degradation of performance was thought to be due to loss of dexterity caused by thick butyl rubber gloves, irrelevant in the context of SARS-CoV-2. The same criticism applies to most other studies of anaesthetic procedures performed while wearing CBRN PPE.15–18 The most comparable study to that presented in this paper is that of Brinker et al., 19 which evaluated CBRN masks (with no other PPE) in a resuscitation scenario involving 14 UK paramedics. The time taken to complete the treatment algorithm was unaffected by the mask.
We found that the LBM was applied significantly more rapidly than the polypropylene N95 mask and glasses. It is unlikely that an approximately 11 second difference will be clinically relevant in most situations. However, in responding to a cardiac arrest (for example), the LBM alone could be donned in approximately seven seconds, affording the wearer protection during the performance of the intervention. Hospital clothing could then be removed for washing and a decontamination shower taken with the CBRN mask still in place, as is military practice when leaving a contaminated environment.
Our study adds to the existing body of knowledge by demonstrating that civilian ICU clinicians of various professions can be taught to use a military CBRN mask effectively in very little time by civilian instructors who themselves have received only brief training. Furthermore, it demonstrates for the first time that these clinicians prefer the LBM to the polypropylene N95 mask and disposable glasses for many reasons, including ease of donning, comfort, and confidence in its protection against aerosol infection.
Our study has several limitations. Our participants were self-selected, rather than chosen at random from the ICU staff. They might have had an unrepresentative bias against the current in-service glasses and N95 mask. We simulated only one clinical task, and we did not perform a detailed evaluation of the time taken to perform the components of that task (such as intubation or insertion of an intravenous cannula) or the success of each attempt. We ceased timing mask application when it was clear the LBM was donned significantly more quickly; however, this might have reduced our ability to observe the significance of any independent predictor of the time to mask application, such as profession. We allowed only a very brief period for the fitting of the LBMs and the training in their use, but we believe this would be no different if they were employed in most civilian hospitals. We only tested one type of air-purifying mask; many others are available both for military and industrial use. We did not test the effectiveness of the seal produced by the 3D printed adaptor for the lighter commercial P3 filter, or the robustness of the adaptor in repeated clinical use. However, this readily produced component did appear to result in a tight seal, and would permit the use of lighter filters that might be more readily available. Most importantly, we could not provide corrective vision spectacles for those participants who required them. Nonetheless, the favourable assessment of the masks was achieved despite this limitation.
Several questions were not answered by this study. Although the LBM has been tested by its manufacturer to meet the relevant Australian and New Zealand standard for protection against airborne viral particles, we did not test the actual effectiveness of either the LBM or the polypropylene N95 mask at filtering particulates, or preventing viral transmission to staff in the clinical environment. A prospective comparison of the effectiveness of each mask type in protecting staff from the transmission of infection from patients, of either randomised or observational design, was clearly outside the scope of our study. A useful preliminary investigation before such a trial would be to compare fit-test results with the two mask types under experimental conditions. Our study has shown this would be a worthwhile endeavour. We have not explored whether the LBM would optimally be used for a full clinical shift in a high-risk environment, or only when performing aerosol-generating procedures. This would be partly determined by the service life of the Scott Pro2000 CFR 22 filter canister, which (in the absence of chemical contamination) the manufacturer recommends to be 50 hours of constant use. In a typical hospital shift work pattern, this could be a full week of nursing shifts at a patient’s bedside. While we cleaned the masks between use using bleach to prevent any possibility of infection transmission between different wearers, if an individual were to be issued their own mask, this would not be necessary. All that would be required would be to decontaminate the outside of the mask (e.g. using Viraclean; Whiteley Corp., North Sydney, New South Wales) between wearing. Such procedures would require a separate empirical evaluation.
This study has two major implications for those writing policy for the use of PPE during the SARS-CoV-2 pandemic. First, while there is no convincing evidence that full-face masks such as the LBM offer greater protection than polypropylene N95 masks and glasses, there is equally no evidence that this is not the case. High infection rates among healthcare staff during the SARS-CoV-2 pandemic 5 , 7 suggest that even theoretical concerns should be addressed. PAPRs are expensive, inhibit communication and require extensive training to ensure safety from contamination during removal, and are in short supply, leading to recommendations against their use except in specific circumstances. 4 Air-purifying full-face masks such as those described in this study might offer an intermediate solution. Second, localised shortages of disposable PPE are likely to remain, and a predominantly disposable approach to PPE is likely to have an enormous environmental impact. 20 If subsequent fit-testing yields positive results, this study has shown air-purifying full-face masks such as the LBM would be an acceptable alternative.
The Australian Defence Force in-service CBRN LBM is suitable for use by civilian hospital ICU staff after minimal training. It is superior in many respects to the polypropylene N95/plastic non-occlusive glasses currently used in the civilian hospital, not least in that many of the staff expressed a greater level of confidence in the protection it afforded against aerosol-transmitted infection. Whether or not this is true, confidence itself is an important characteristic of PPE. As a reusable alternative to disposable PPE that is proving difficult to supply to many parts of the world during the SARS-CoV-2 pandemic, the LBM, and many similar masks that are commercially available, should be considered for further evaluation in high-risk environments.
Footnotes
Acknowledgements
The author(s) thank the officers and soldiers of the 2nd Combat Engineer Regiment of the Australian Army who provided instruction on the use and decontamination of the LBMs employed in this study.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.