
Abstract
More than 300 million surgeries are performed worldwide annually. Established perioperative centres in the UK, USA and Australia have demonstrated the impact of improving perioperative care in reducing costs, increasing patient satisfaction and improving population health. Likewise, the surgical burden of care in Asia is increasing, but with sociocultural, economic and epigenetic differences compared to the west. As Singapore’s largest hospital, the Singapore General Hospital pre-admission perioperative clinic sees about 20,000 patients annually. We aim to illustrate Singapore General Hospital’s perioperative model of care to contribute to the paucity of literature describing perioperative programme implementation within Asia, and to encourage the cross-sharing of perioperative practices internationally. Our perioperative framework navigates risk assessment, risk counselling, and mitigation of health, medical and functional risks to better patients’ perioperative outcomes and population health. We have implemented evidence-based pathways for common conditions such as anaemia and malnutrition, including a multidisciplinary programme for the elderly to tackle frailty and reduce length of stay. We describe how we have enhanced local risk profiling with the Combined Assessment of Risk Encountered in Surgery surgical risk calculator derived locally using a gradient boosting machine learning model. Finally, we report clinical outcomes of these interventions and discuss further challenges and new initiatives at each tier of our perioperative model. Our perioperative care model provides a framework that other centres can adopt to promote value-driven care, while catering for differences in the Asian population, thereby promoting evidence-based improvements in the area of perioperative medicine.
Background
Perioperative mortality is the third leading cause of death after heart disease and cancer globally, with more than 15% of patients who undergo elective surgeries experiencing at least one postoperative complication.1–3 With more than 300 million surgeries performed worldwide every year, the need to improve quality of perioperative care is paramount. Anaesthetists are in the ideal position to orchestrate this during the perioperative period. In particular, the preoperative setting is an excellent opportunity for optimisation programmes to mitigate risks, personalise and prioritise healthcare resources for high-risk groups. Furthermore, it is an important ‘teachable moment’ when healthcare providers can promote better overall health by increasing awareness of beneficial lifestyle changes. 4 High-quality perioperative care can improve patients’ experience, quality, outcomes of care, and promote population health.
Over the years, established centres around the world have invested in multidisciplinary programmes aimed at improving perioperative care. For example, the proactive care of older people undergoing surgery programme was developed at Guy's and St Thomas' National Health Service (NHS) Foundation Trust with the geriatric surgical population in mind, and was incorporated into UK National Institute for Health and Care Excellence (NICE) guidelines. The perioperative surgical home was a similar concept by the American Society of Anesthesiologists (ASA) to embrace the idea of multidisciplinary seamless patient-centred care through the surgical pathway to recovery. 5 In the USA, Duke University (Durham, NC, USA) designed the multidisciplinary perioperative enhancement team model with focused preoperative clinics and coordinated pathways to optimise surgical and anaesthetic risk factors in the perioperative period. These preoperative risk assessments and workflows seamlessly identify high-risk patients with the aim of minimising postoperative adverse outcomes. 6 In addition, Brigham and Women’s Hospital (Boston, MA, USA) Centre for Perioperative Management and Medical Informatics, as well as the Centre for Perioperative Research, actively invest in medical technology and research for perioperative care to improve the efficiency of health systems. 7 The Australian and New Zealand College of Anaesthetists council recently published a framework for perioperative care designed to provide guidance in perioperative medical training, services and research. 8 This is another case in point of how perioperative medicine has become a strategic priority of many western centres and is crucial for value-driven care.
With the rapidly ageing population in Asia, the surgical burden of care is also increasing. Yet, there is a paucity of published literature describing perioperative programme implementations in Asia. This is relevant as sociocultural, economic and epigenetic differences with the west bring about distinctive challenges. Singapore General Hospital (SGH) is the first and largest hospital in Singapore, catering to over 25,000 elective surgical cases a year. 9 As an academic medical centre, we have also successfully established our own perioperative model of care by profiling our local patient population and setting up a comprehensive perioperative medicine centre.
We aim to describe the transformation of SGH’s perioperative medicine services through best practice care design and comprehensive multidisciplinary programmes. Our perioperative framework navigates key opportunities to better perioperative outcomes and population health, with anaesthetists contributing to ‘high-value, high-quality, patient-centred care’.10,11
Perioperative care model
The SGH pre-admission clinic (PAC) sees about 20,000 patients annually. It is a one-stop integrated clinic that encompasses stations for anaesthesia assessment, internal medicine perioperative clinic, preoperative physiotherapist and dietitian assessments, nurse counselling for specific surgical programmes, intravenous (IV) iron infusion suites, as well as financial counselling for patients (see Figure 1). This was developed over the course of a decade with the support of the hospital administration as it allowed more surgeries to be done as same day admissions, obviating the need for hospital admission one day before surgery for preoperative assessment. This, in turn, helped to save hospital beds and reduced hospital length of stay for elective surgeries. Through targeted risk assessment, risk stratification, risk counselling and risk mitigation (see Figure 2), we redesigned our perioperative services for efficiency and improved clinical outcomes. The PAC has rendered many preoperative inpatient admissions unnecessary, and this is reflected in our same day admission rate of 93% currently. All costs of investigations, referrals and treatment raised at the PAC are subsumed under the inpatient bill that is paid when the patient is discharged from their elective surgery. Hence, patients do not need to pay cash upfront for their PAC visit, which further increases convenience for the patients.
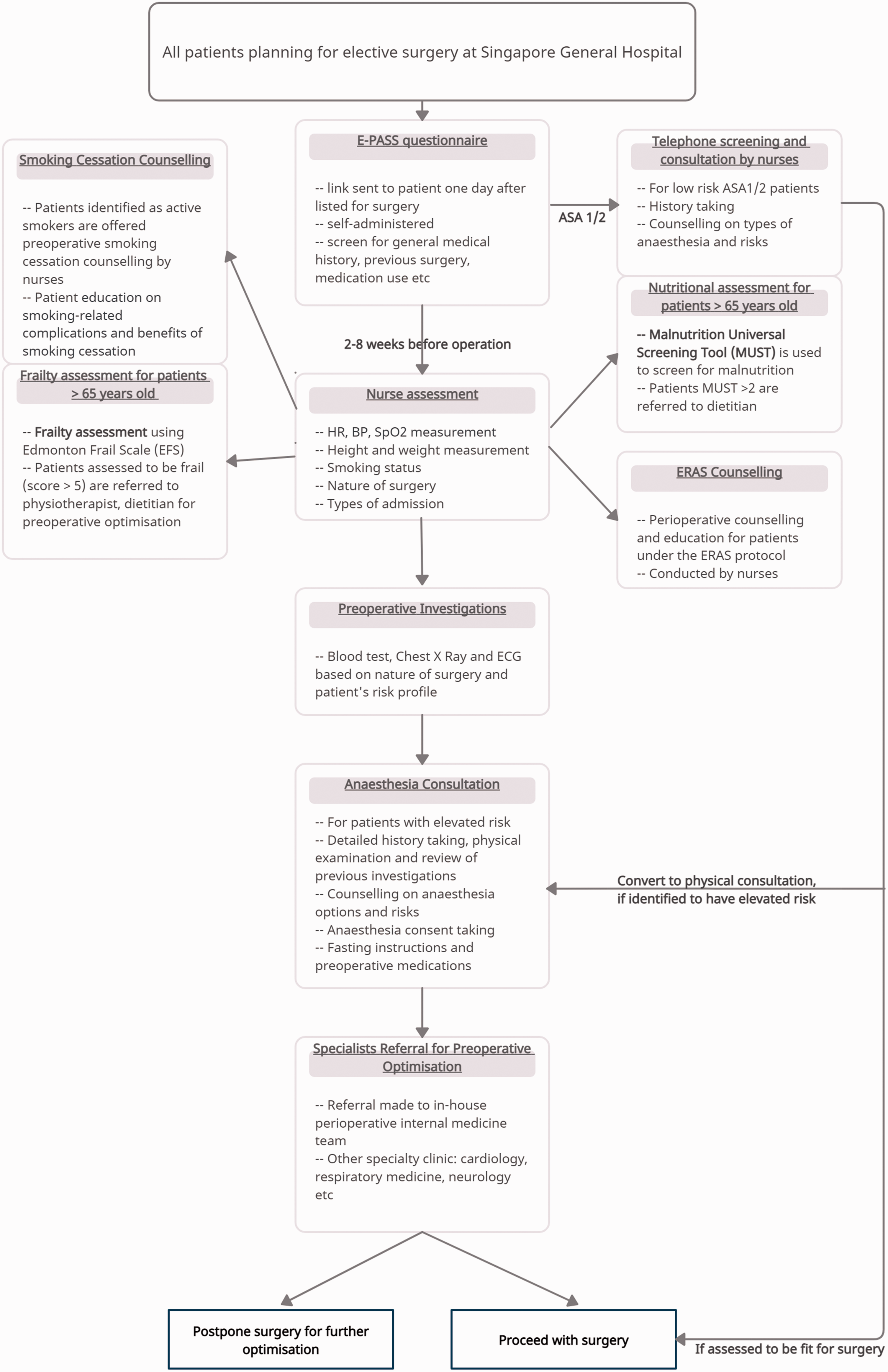
Workflow in pre-admission clinic (PAC). The workflow briefly describes a patient’s preoperative journey of assessment and optimisation in the PAC when planning for elective surgery in Singapore General Hospital. Pre-op: preoperative; periop: perioperative; E-PASS: electronic pre-anaesthesia self-screening; HR: heart rate; BP: blood pressure; SpO2: oxygen saturation; ECG: electrocardiogram; ERAS: enhanced recovery after surgery.
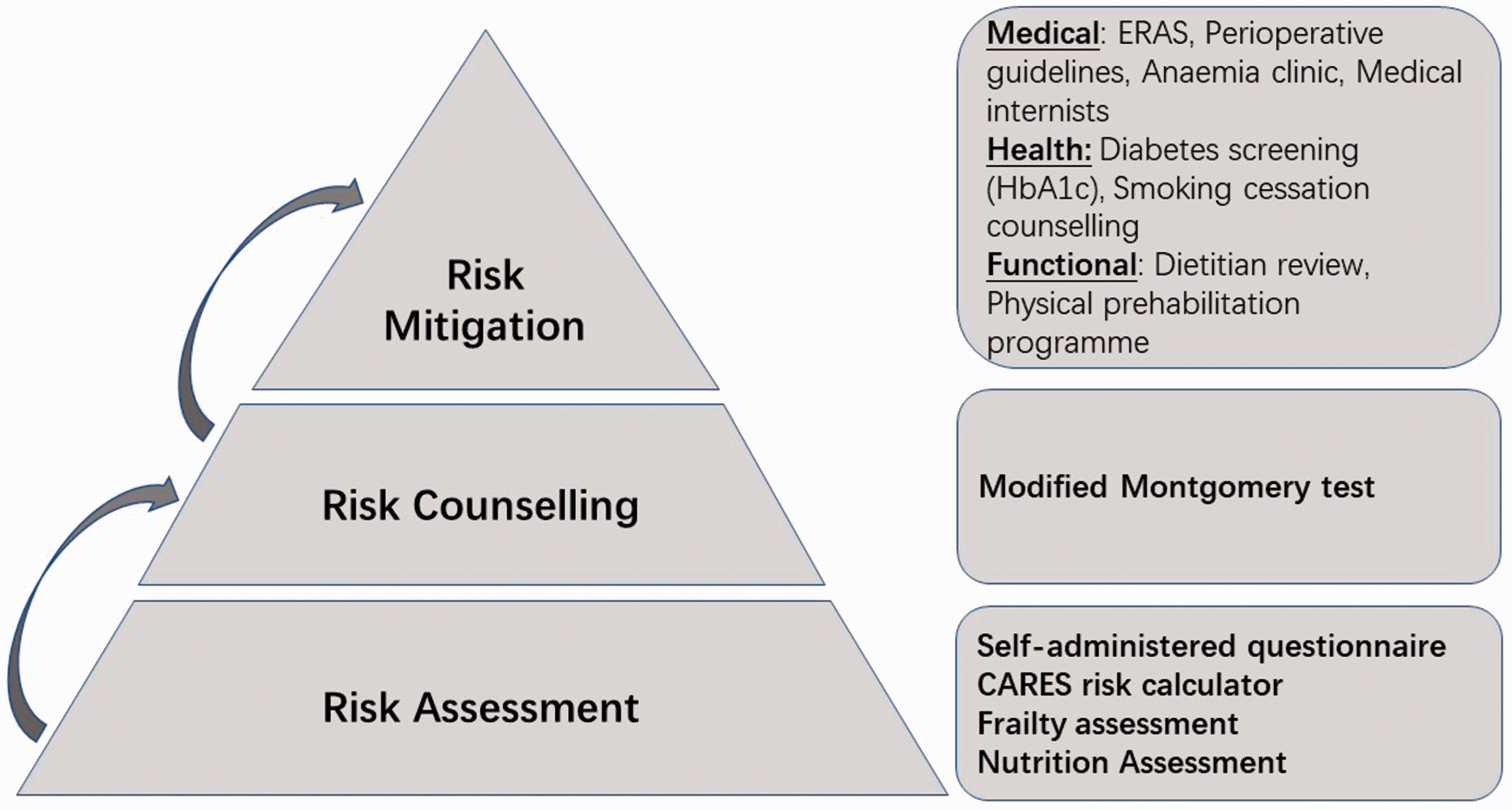
Pyramid of risks. Risk assessment, risk counselling and risk mitigation are the main components of a patient's perioperative journey. This figure describes the relationship between the three components and examples under each category. CARES: combined assessment of risk encountered in surgery score; ERAS: enhanced recovery after surgery; HbA1c: glycated haemoglobin.
Risk assessment
Risk assessment is the crucial first step towards impacting patients’ outcomes. In SGH’s PAC, patients are sent a link on their mobile devices to fill out the electronic pre-anaesthesia self-screening questionnaire (E-PASS) that was developed in-house for assessing perioperative risk. Low-risk patients (aged 21–64 years, ASA physical status score 1 based on their E-PASS responses) and planned for low surgical risk procedures are eligible for nurse-led preoperative assessment (NPA) and counselling of their anaesthesia risks. This is done via phone consultation to save the patient an unnecessary clinic visit. High-risk patients will undergo a comprehensive preoperative review by anaesthetists in the PAC. The segregation of patient care based on risk profile prioritises high-risk groups such as the elderly or patients with complex comorbidities to receive closer medical attention. It has also alleviated manpower staffing demands of the PAC on doctors by shifting some of the patient load onto appropriately trained nurses, and helped shorten the waiting time for doctor consultations at the PAC.
Frailty results in diminished physiological reserve and increases vulnerability to adverse outcomes when exposed to stressors such as surgery. 12 It is therefore a crucial part of our preoperative assessment. Our institution uses the Edmonton Frail Scale (EFS) as a surrogate marker of frailty for surgical risk stratification. The EFS is a simple validated performance-based tool for assessing geriatric patients in the primary care and surgical setting. 13 The EFS score was also found to be a significant predictor of postoperative morbidity and predicts both early and 30-day postoperative complications. 14 The estimated prevalence of frailty (EFS ≥ 6) in our elderly surgical population (aged > 65 years) is around 29%. 14
Currently, validated perioperative risk assessment tools have largely been derived from western population data, such as the American College of Surgeons National Surgical Quality Improvement Program Surgical Risk Calculator, 15 the Surgical Outcome Risk Tool, 16 used in the UK, and the nzRISK risk prediction model used in New Zealand. 17 In Singapore, we have developed the Combined Assessment of Risk Encountered in Surgery (CARES) surgical risk calculator based on local data for better applicability. This calculator was derived from a cohort of 79,914 patients in Singapore using a gradient boosting machine learning model and provides prediction for both postoperative mortality within 30 days and likelihood for postoperative intensive care unit admission exceeding 24 hours based on certain scoring variables.18,19 Subsequently, we further investigated how traditional surgical risk predictions can be advanced through machine learning.19,20 Machine learning techniques are capable of harnessing the large number of variables available, such as in the local electronic health records, and offer better predictive performance. 21 The utilisation of locally-derived data and expertise facilitated the deployment process within our electronic medical records system. These robust risk assessments aid the decision of appropriate postoperative monitoring and disposition of our patients.
Risk counselling
Providing information and risks to the patient early provides opportunities for clarification of doubts before surgery. This may alleviate surgical fears, encourage retention of information and is considered the best practice. The patient may feel under duress to proceed if such information is offered only on the day of surgery. 22 Furthermore, surrogate decision-making for older patients is common practice in Asia. Doctors frequently consult the family before discussing serious medical issues and anaesthetic risks with these patients. 23 Consequently, we designed our PAC with enough space to accommodate the involvement of large families. A pre-existing relationship of openness, trust and rapport between doctor, patient and family is crucial, especially if complications are encountered perioperatively.
The modified Montgomery test passed by the Singapore Court of Appeal fundamentally shifts the emphasis from what a ‘reasonable doctor’ should explain when dispensing medical risks to what a ‘reasonable patient’ would expect to be informed considering one’s unique circumstances. 24 We have established what Singaporeans regard as material risks in the anaesthetic consent-taking process by conducting surveys within our population. 25 For instance, patients have greater concerns about rare but serious or possibly permanent complications, rather than common but minor complications. Asian patients were also more willing to pay to avoid negative emotions than to experience positive ones. 26 Moreover, many patients attributed greater importance to avoiding out-of-pocket payments, such as dental injury. 25 This is perhaps a reflection of our healthcare structure. Dental procedural fees in Singapore may be costly with limited insurance coverage. Hence, dental complications are likely to cost more when compared to treatments for other more unpleasant complications such as nausea, skin or tissue injuries or pain. 27
Through understanding factors that influence medical decision-making, 25 we tailored our structured anaesthetic consent form accordingly and are able to provide relevant information during risk counselling. Patients are also provided a brochure on the surgical journey for home. This brochure contains succinct information pertaining to the anaesthesia, its complications and the usual postoperative recovery trajectory. This is intended to help retain information that was discussed. Through these efforts, we aim to minimise the misalignment of expectations, impart realistic understanding of the proposed surgery and prognosis in a multidisciplinary setting and achieve improved preparedness and outcomes.
Risk mitigation (medical, health and functional risks)
Singapore has fared well in terms of life expectancy and has among the lowest disability-adjusted life years (DALYs) per 100,000 population in the world, according to the Lancet global burden of disease 2019 report. DALY is a summary measure of the years of healthy life lost due to premature mortality and ill health experienced by a population. Despite this, 35% of our DALY burden may be potentially improved by targeting modifiable risk factors early. 28 Hence, we target three areas of risk mitigation at our PAC to reduce this burden: medical risks, health risks and functional risks.
Medical risks
The presence of two or more chronic diseases is considered multimorbidity, and is significantly associated with decreased functional status, 29 reduced quality of life, 30 greater use of healthcare resources, 31 and high mortality rates. 32 We estimate its prevalence at 26.2%. 33 Moreover, a positive correlation exists between multimorbidity and frailty. In particular, diabetes mellitus (DM), chronic kidney disease, previous cerebrovascular accidents or transient ischaemic attack, dementia, depression, peptic ulcer disease and moderate anaemia are some independent factors associated with frailty 34 that should be reviewed before surgery.
Our PAC houses medical internists who review referrals from anaesthetic doctors within the same day. These specialists direct further investigations and optimisation of newly diagnosed or poorly controlled chronic conditions that have an impact on anaesthesia outcomes. They also provide continuity of care through outpatient follow-up with these patients after their surgical procedure. We have collaborated with the relevant specialists to produce comprehensive evidence-based guidelines that target modifiable chronic diseases: cardiac evaluation and referral pathway with the cardiologists; thyroid function test interpretation and management with the endocrinologists and cervical spine clearance with the orthopaedic spine specialists.
An example is our anaemia pathway (see Figure 3), which was adapted from international guidelines 35 and was developed in collaboration with the haematologists and internal medicine physicians. Preoperative iron deficiency anaemia, which affects 27.8% of our surgical patients, is associated with increased perioperative morbidity and mortality,36,37 with macrocytosis and high red cell distribution width (> 15.7%) being potential markers. 38 Our department’s iron deficiency anaemia protocol incorporates iron studies into patients’ preoperative tests if they have a history of anaemia or are found to be anaemic on their preoperative full blood count. Patients with iron deficiency anaemia who are suitable for IV iron infusion are further referred to the on-site internists. This is administered within the PAC either on the same day as their PAC visit or the following day. 39
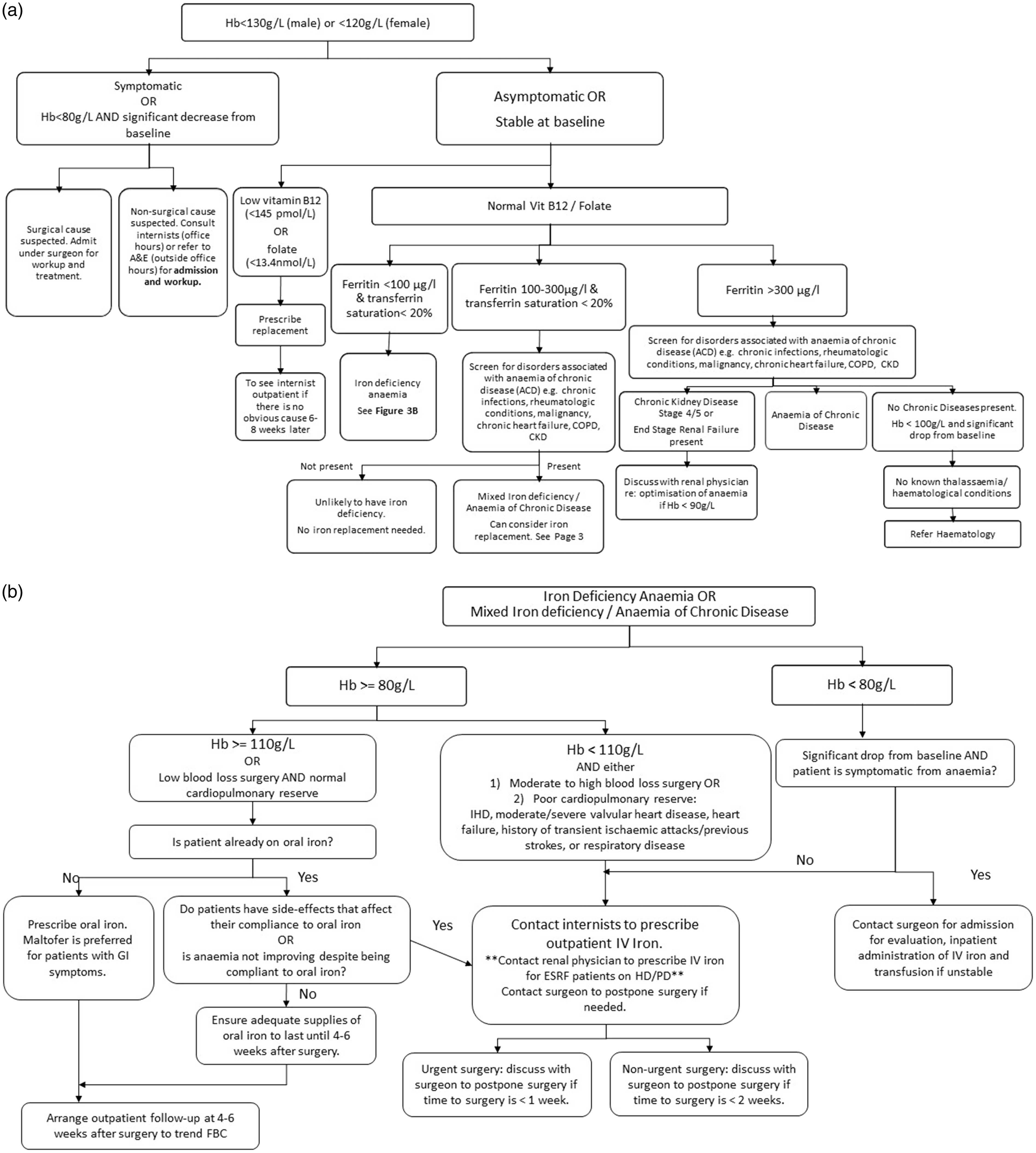
(a) Anaemia pathway. This pathway provides recommendations and triage of anaemic patients undergoing elective surgery, consistent with our hospital’s blood management programme. Hb: haemoglobin; A&E: accident and emergency department; Vit B12: vitamin B12; COPD: chronic obstructive pulmonary disease; CKD: chronic kidney disease; re: regarding and (b) Iron deficiency anaemia pathway. This pathway illustrates how iron deficiency anaemia is optimised preoperatively in patients undergoing elective surgery. Hb: haemoglobin; GI: gastrointestinal; FBC: full blood count; IHD: ischaemic heart disease; CCF: congestive cardiac failure; IV iron: intravenous iron; ESRF: end-stage renal failure; HD: haemodialysis; PD: peritoneal dialysis.
To achieve earlier recovery for patients undergoing major surgery, multimodal Enhanced Recovery After Surgery (ERAS) programmes have been designed for most surgical specialties, such as colorectal, 40 hepatobiliary, orthognathic and orthopaedic surgeries. 41 Implementation of ERAS has replaced different clinician-based practices with standardised evidence-based best practices throughout the perioperative journey.42,43 Anaesthetists play a vital role of steering important aspects of the ERAS pathways such as preoperative patient optimisation, choice of anaesthetic regimen, and fluid and pain management, and therefore facilitate and bridge the gap between pre- and postoperative periods. For orthopaedic, orthognathic and colorectal surgeries, our patients receive extensive face-to-face preoperative counselling by trained nurses to align their expectations and enhance mental preparedness for major surgeries.
Health risks
It is important to tackle population health risks early so as to deter the progression to chronic health issues. These modifiable risk factors include smoking, poor diet, low physical activity, high blood pressure, high fasting plasma glucose level, high body mass index and high low-density lipoprotein (cholesterol) level. 28 Preoperative obstructive sleep apnoea (OSA) screening through the use of the STOP-Bang questionnaire, 44 type 2 DM screening using glycated haemoglobin (HbA1c), smoking cessation pathway, and direct echocardiogram referrals have been implemented to detect undiagnosed health risks and address them before surgery and beyond.
There is a high prevalence of DM especially in the Asian populations, and this contributes to more than 60% of the world’s diabetes population. 45 HbA1c is a validated surrogate marker, and in our recent study of 888 patients, 21% of elective non-cardiac surgical patients had HbA1c of 6.1% or greater. Thirty-seven (4.2%) of these patients did not have a diagnosis of pre-DM or DM, implying that the perioperative encounter could be utilised as a screening opportunity. 46 At-risk elective surgical patients include patients aged 60 years and above, Indian ethnicity and body mass index greater than 27.5. 46 While HbA1c is more costly than blood glucose testing, the focused use of healthcare resources on at-risk patients can reduce eventual healthcare costs by early detection.
There is strong evidence that the perioperative period is a teachable moment, and preoperative smoking interventions including nicotine replacement therapy increase short-term smoking cessation and may reduce postoperative morbidity. 47 We are currently in the process of establishing an intensive multidisciplinary perioperative smoking cessation programme to ensure more smokers achieve long-term smoking cessation. 48 Among 3362 patients surveyed, 10.4% were current smokers. Only 59% were aware of related postoperative complications, but most showed interest in quitting preoperatively when educated on the benefits. 48 We now identify receptive smokers for cessation counselling by our trained nurses. Patients who are ready to take further steps towards cessation would be referred on to smoking cessation counsellors for detailed discussions on the appropriate strategies and need for pharmacological aids. There is an ongoing study to evaluate the efficacy of our intensive perioperative smoking cessation programme.
Functional risks
In our perioperative care model, functional risks include functional capacity (or cardiopulmonary fitness), which overlaps with muscular strength, balance and frailty. Functional capacity is an ‘integrated physiological response’ 49 that reflects an individual's ability to respond to physiological stress such as surgery, while frailty results in increased susceptibility to poorer outcomes secondary to existing comorbidities and age-related decline. 49 We attempt to mitigate functional risks through our perioperative programme for elderly (PREPARE) workflow programme 50 that tackles both frailty and malnutrition in the elderly. PREPARE encompasses dietitian referrals for preoperative nutrition optimisation, as well as physiotherapy review. Interventions by the physiotherapists include preoperative education, physical evaluation, prescription of home exercise programmes to improve strength and aerobic capacity, and the issuance of an inspiratory muscle trainer for patients with low maximal inspiratory pressure for respiratory muscle training. Our PREPARE workflow was designed to reduce length of hospital stay and enhance general health and wellbeing of frail elderly patients before they undergo major surgery. Patients planned for major surgery who are deemed at the PAC to be frail (EFS score greater than or equal to 6) or have physical frailty (functional score (combined independence and performance scores) greater than or equal to 3) will be referred to the programme.
In our surgical population, 11.9% are at risk of malnutrition. We realise that interventions are necessary to tackle this modifiable risk factor as malnutrition increases the risk of poor wound healing and postoperative complications.51–53 The Malnutrition Universal Screening Tool (MUST) has been validated for inpatient assessment of malnutrition,54,55 and has been adopted for inpatient screening in our institution. Based on the recommendation from our institution’s dietitians, our PAC nurses also use this to screen for malnutrition for patients above 65 years of age. Patients at risk of malnutrition (MUST score ≥ 2), and undergoing cancer surgery or vascular surgery with distal leg wounds are referred to dietitians for nutritional education and prescription of preoperative enteral nutrition supplementation when appropriate.
Clinical outcomes
All patients listed for elective surgery under anaesthetic care at SGH are now referred to the PAC. We see an average of 20,000 patients a year, with 16% of our patients labelled as ASA classification class 1, 67% ASA 2, 15% ASA 3 and less than 1% ASA 4. From recent audits, about 57% of patients who fulfilled the clinical criteria (low-risk patients aged 21–64 years, ASA 1 and planned for low surgical risk procedures) and responded to the E-PASS questionnaire received NPA. The remainder were excluded due to medical conditions that were unearthed in the questionnaire. The use of E-PASS dovetailed with the adoption of telemedicine as a result of the COVID-19 pandemic.
In our efforts for risk mitigation, 453 and 258 patients received outpatient IV iron therapy in the years 2019 and 2020, respectively at PAC. To address frailty, our PREPARE programme has seen about 262 patients undergoing physiotherapy prehabilitation and 107 patients were referred to dietitians from the PAC last year. These figures are likely to increase as elective caseloads were disrupted during the COVID-19 pandemic. Although we offer supervised exercise programmes in our hospital’s outpatient physiotherapy department to our patients who have adequate time to surgery (i.e. more than two weeks), the take-up rate for this has been low at 7%. At present, we are conducting a randomised controlled trial to compare the efficiency of the current standard of care in improving functional capacity, which is the unsupervised home exercise programme, against a new initiative that sees our physiotherapists conduct home visits to guide our patients with exercises in the convenient setting of their homes (clinical trials registration: NCT04892368). The results of this study should be available at the end of 2023.
Challenges and the future
We have established our tiered transformational model, and designed unique systems and processes built on existing published models that largely represent western societies. A workable perioperative model has to consider the construct of our healthcare system and patient epigenetics, as well as contextualise the society it exists within. We have earlier touched on what makes the Asian perspective unique and will elaborate further. Singapore’s government-run healthcare system is financed through a combination of direct government subsidies, compulsory comprehensive individual saving schemes, national healthcare insurance, cost sharing and optional private insurance. This is in contrast to the tax-funded NHS in the UK where healthcare services are free at the point of delivery for residents, and the predominantly publicly financed private delivery system in the USA. With an emphasis on co-payment, our patients’ expectations of healthcare extend beyond just treatment of their medical conditions. Moreover, this co-payment model may motivate patients to be responsible for their health, increasing the impact of utilising the perioperative period as a teachable moment. Also, differences in epigenetics impact clinical practice and protocols. For example, in patients with OSA, Asians were found to be less obese but have greater severity of OSA compared to the Caucasian population, possibly due to differences in obesity and craniofacial features. 56 Another example is the higher prevalence of dementia among Asians, especially among ethnic Malays and Indians. 57 Finally, cultural norms dictate that healthcare decision-making in Asia tends to be heavily influenced by the patients’ families, 58 which differs markedly from the social ethos of western nations where the competent patient usually decides.
In terms of challenges and future prospects, the perioperative medicine landscape is constantly evolving with new initiatives introduced at every tier of the perioperative model. Hence, all members of the perioperative team have to keep up with the latest recommendations and evidence bodies to provide cost-effective and best clinical care.
Furthermore, risk modifications often rely on behavioural changes. These include compliance with medications for optimisation with health risks, and lifestyle changes such as smoking and alcohol cessation. Poor lifestyle choices and unwillingness to change are well recognised barriers to achieving the desired results. 59 This is compounded by the limited time window before surgery to effect such changes. In order to increase the efficiency of the preoperative process from listing to surgery, we have consolidated the surgical listing and financial counselling processes under one preoperative services team. Thus, we are able to collaborate closely with the administrative staff at the preoperative services team continually to monitor the lead time from surgical listing to PAC date, to surgery date. This optimises the appointment creation algorithm, ensuring that high-risk patients will be reviewed earlier at the PAC, allowing more time for preoperative optimisation. Providing educational resources, easy accessibility and continued follow-up have also been shown to be key enablers in patient engagement for lifestyle modification programmes. 60
Finally, as with all ageing societies, we expect to encounter more geriatric surgical patients with complex comorbidities and frailty. Dedicated perioperative physicians are crucial in coordinating and optimising these comorbidities. ERAS society guidelines will also be contextualised locally, as increased variety of surgeries are performed. Importantly, the PAC visit should continue to serve as a ‘pause point’, engaging high-risk patients and their families on their health goals, values and preferences preoperatively. 61
Conclusion
In conclusion, we have described our perioperative continuum of care that incorporates evidence-based strategies and value-driven care models that have been adapted from the western experience for our Asian population. A patient’s sentinel surgical encounter is a valuable touchpoint for proactively practising population health, for example, through smoking cessation programmes and various health screening interventions. Through the development of local screening tools and workflows for preoperative risk assessment and optimisation, our clinicians are able better to prepare patients for surgery through counselling and personalised risk mitigation as illustrated. Finally, the successful implementation of any holistic pathway in the perioperative setting requires the coordinated and concerted effort of all clinicians, nurses, allied health members such as dietitians, physiotherapists and administrative staff, as well as hospital leadership to bring these programmes to fruition.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to thank the nurses in the perioperative clinic and the team of medical internists who have worked closely with them.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.