
Abstract
Adverse events associated with failed airway management may have catastrophic consequences, and despite many advances in knowledge, guidelines and equipment, airway incidents and patient harm continue to occur. Patient safety incident reporting systems have been established to facilitate a reduction in incidents. However, it has been found that corrective actions are inadequate and successful safety improvements scarce. The aim of this scoping review was to assess whether the same is true for airway incidents by exploring academic literature that describes system changes in airway management in high-income countries over the last 30 years, based on findings and recommendations from incident reports and closed claims studies. This review followed the most recent guidance from the Joanna Briggs Institute (JBI). PubMed, Ovid MEDLINE and Embase, the JBI database, SCOPUS, the Cochrane Library and websites for anaesthetic societies were searched for eligible articles. Included articles were analysed and data synthesised to address the review’s aim. The initial search yielded 28,492 results, of which 111 articles proceeded to the analysis phase. These included 23 full-text articles, 78 conference abstracts and 10 national guidelines addressing a range of airway initiatives across anaesthesia, intensive care and emergency medicine. While findings and recommendations from airway incident analyses are commonly published, there is a gap in the literature regarding the resulting system changes to reduce the number and severity of adverse airway events. Airway safety management mainly focuses on Safety-I events and thereby does not consider Safety-II principles, potentially missing out on all the information available from situations where airway management went well.
Keywords
Introduction
Adverse events associated with failed airway management can be catastrophic and cause irreversible hypoxic brain injury, prolonged admission to the intensive care unit (ICU), cardiac arrest and death. 1 Airway management is routinely performed by anaesthetists, critical and acute care specialists 1 and less frequently by pre-hospital retrieval services and the military. Despite many guidelines, cognitive aids and an ever-increasing range of new equipment and devices, airway incidents and patient harm continue to occur.1 –5 These incidents are often unexpected and may involve healthy patients who undergo straightforward procedures.6,7
The ability to study airway incidents and their complications in experimental studies is hampered by two significant factors. First, there is a low incidence of adverse events in airway management and therefore randomised controlled trials are not possible. Second, these types of trials would be considered unethical: for example, avoiding interventions for research purposes when a patient is at risk would be negligent. 8 Therefore, much of the available evidence is based on manikin studies, expert opinion, observational research, case reports and local audits.
Observational research may be categorised into two main data sets: data from incident collections2,3,9 –13 and data from events that lead to litigation.6,7,14 Examples of larger databases collecting incidents include the Australian and New Zealand web-based Anaesthetic Incident Reporting System (webAIRS)4,15 and the UK’s Fourth National Audit Project (NAP4). 1 Examples for data from insurance claims are the National Health Service (NHS) Litigation Authority claims data from the UK 14 and the American Society of Anesthesiologists closed claims analyses.6,7,16,17 Both types of databases are used to analyse the frequency of a particular source of patient harm, describe the trends and patterns and explore underlying causation. 18 Significantly, analysis of relevant databases has identified that the incidence of adverse airway events has changed little over the past three decades since detailed data collection commenced.1,4
A critical step across all areas of healthcare in managing safety risks is that of learning from past events and creating pathways to prevent incidents from recurring.18 –25 As healthcare becomes more complex, so too do the concepts of safety management. For example, the principle of ‘Safety-I and Safety-II’ investigates studies of failures (Safety-I) and analysis of success (Safety-II). 26 Safety-I promotes ‘as few things as possible go wrong, and no adverse events happen’, whereas Safety-II ensures that as many things as possible go well.27 –29 In an ideal environment, with a positive culture of reporting, all adverse events, including near misses, would be quickly analysed, managed appropriately, documented and communicated. The findings would be used to implement system changes, including the redesign of policies, processes of care and procedures, and changes in clinical practice and training, leading to a measurable, sustained reduction of risk and the elimination of harm.
The aim when establishing patient safety incident reporting systems is to monitor and report on Safety-I events and, through using these data, reduce the risk of incidents in healthcare. 18 Unfortunately, a recent review by the World Health Organization (WHO) identified a lack of consistently high-level investigation of incidents in healthcare and, consequently, a lack of implemented, effective risk-reduction strategies. 18 The review found that, while collecting, storing and reporting of data is occurring in medicine, corrective actions are too often inadequate, and no formalised links between understanding what went wrong and reducing risk are evident. Examples of successful improvement in patient safety arising from analyses of reported incidents were found to be scarce. 18 To the authors’ knowledge, a systematic review has not been performed to assess whether the same is accurate regarding the response to reported airway incidents. Information obtained from this review may guide advancements in airway incident reporting, their analyses and, consequently, the implementation of successful safety measures.
A formal evaluation and synthesis of systems changes resulting from airway management incident reporting systems has not occurred in a systematic review. Therefore, the aim of this scoping review was to explore academic literature that describes system changes in airway management in high-income countries over the last 30 years, based on findings and recommendations from incident reports and closed claims studies. The objectives of this review were to collate the findings and recommendations across all speciality healthcare providers that perform airway management to understand which system changes have been implemented and to examine their effect.
Methods
The methodology for this review was based on the most recent guidance for scoping reviews outlined by the Joanna Briggs Institute (JBI) 30 and Pollock et al. 31 This guidance suggested the following five phases: (1) specifying the research question, (2) identifying relevant studies, (3) study selection following an extensive literature review, (4) extrapolating the data and (5) collating, summarising and reporting the results.
A scoping review rather than a systematic review approach was chosen because the topic of this study has not yet been extensively studied, and an initial preview of the literature did not identify sufficient evidence for a formal systematic review. Instead, a scoping review aims to identify literature gaps, map the available evidence and provide an overview of the existing literature. Using a ‘Population, Concept and Context (PCC)’ framework, this scoping review sought to answer the question: ‘What is the nature of the response to airway management incidents in high-income countries based on findings from incident reports and closed claims studies, and what are their effects on end users and systems?’ For the purpose of this scoping review, ‘the nature of the response' was defined as the system changes that have been implemented based on findings and recommendations from incident reporting, whereas the ‘effects on end users and systems' describes the results of these implementations on patient safety (Figure 1). An a priori review protocol was developed and registered with Figshare.com. In this final report, the only deviation from the a priori protocol was the removal of local case series and case reports from the inclusion criteria, as the exploration of these did not provide sufficient information to answer the research question.
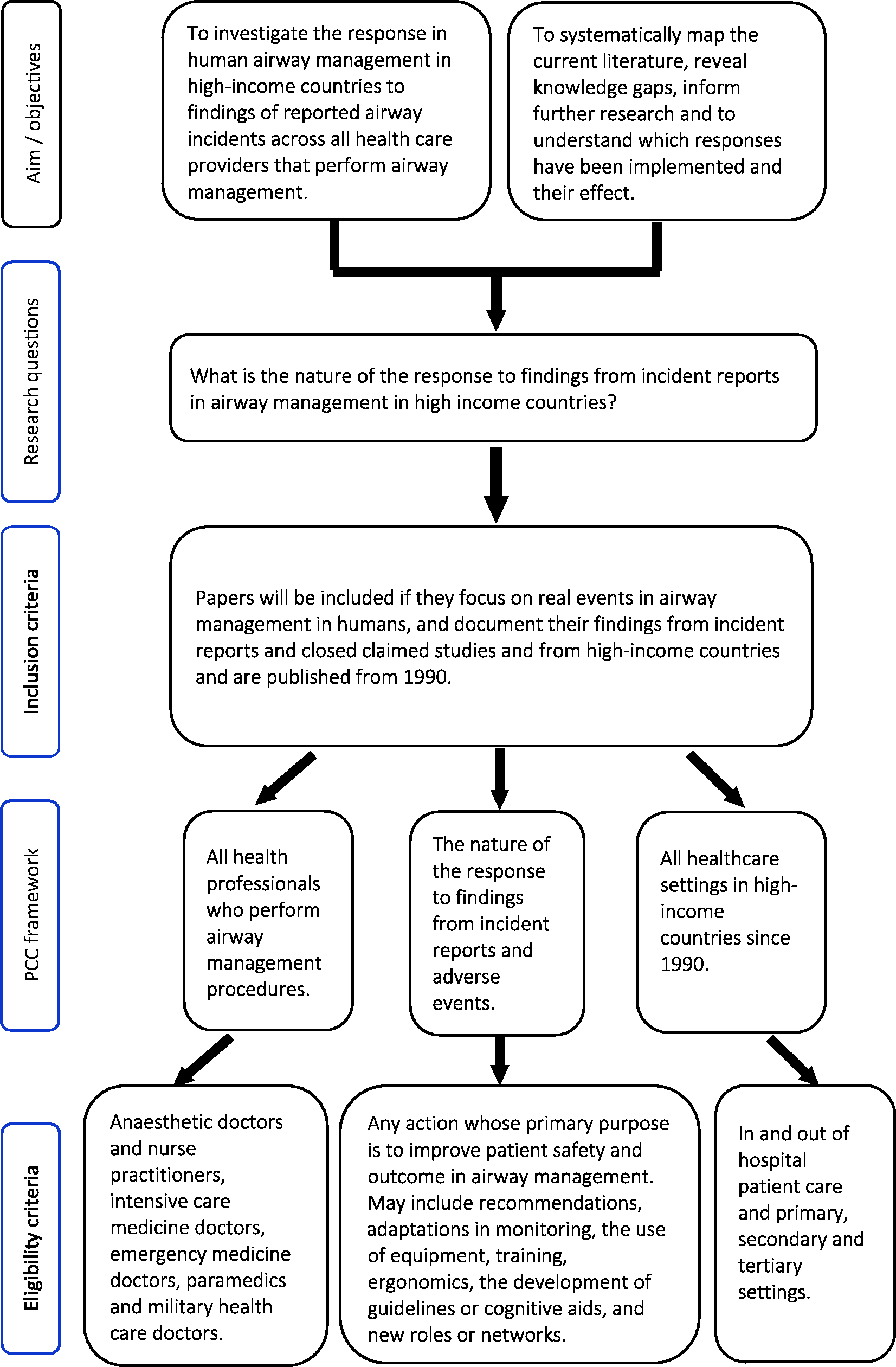
Scoping review overview.
Search strategy and data sources
The literature search was conducted using the following databases: PubMed, Ovid MEDLINE and Embase, the JBI database, SCOPUS and the Cochrane Library. The search terms were developed with the assistance of an academic librarian and included a combination of medical subject headings (MeSH) and keywords (see Appendix 1). Key terms were identified through an iterative process involving the review of target articles. Additionally, websites of airway management societies and groups written in English, and websites of incident reporting systems groups in high-income countries were searched for grey literature and publications.
Study selection
All study designs, including qualitative and quantitative methods, were considered. The titles and abstracts of all identified articles were imported into a referencing program (Endnote™ X9.3.3) and all duplicates were removed. Following this process all articles were uploaded to an abstract and full-text screening program (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia) where the title and abstracts of the remaining articles were independently screened by the first author and one of two co-authors, following the agreed inclusion criteria. All three authors reviewed any conflicts or uncertainties and agreed on a final decision for article inclusion. All authors reviewed the remaining full-text papers and examined their reference lists. Additional articles that met the inclusion criteria were added to the review.
Websites that were searched for grey literature included the following: Difficult Airway Society (UK: https://das.uk.com/), Society of Airway Management (https://samhq.com/), European Airway Management Society (http://eamshq.net/index.php), Safe Airway Society (https://www.safeairwaysociety.org), Anesthesia Incident Reporting System (https://www.aqihq.org/index.aspx), webAIRS (https://www.anztadc.net), Canadian Patient Safety Institute (https://www.patientsafetyinstitute.ca), Australian and New Zealand College of Anaesthetists (http://www.anzca.edu.au), Australian College of Emergency Medicine (https://acem.org.au/), the former European Society of Anaesthesiology (http://www.esahq.org/euroanaesthesia), Canadian Anesthesiologists’ Society (http://www.cas.ca), Scandinavian Society of Anaesthesiology and Intensive Care Medicine (http://ssai.info/guidelines/) and the College of Intensive Care Medicine of Australia and New Zealand (https://www.cicm.org.au) (Figure 2).
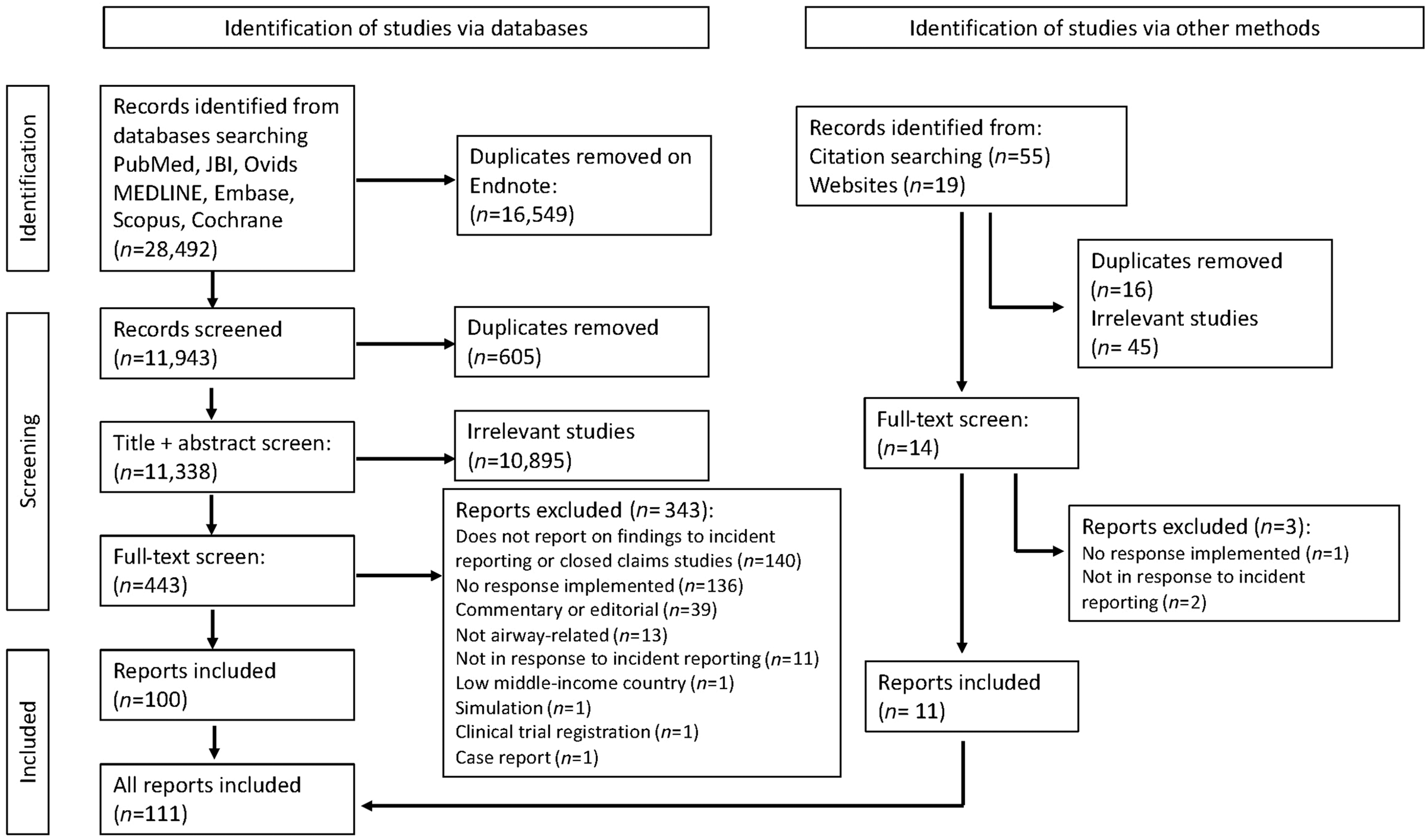
PRISMA flow chart. Identification, screening, eligibility, and inclusion of articles in the systematic scoping review.
Inclusion criteria (PCC framework)
Population
The population included all health professionals who perform airway management procedures; examples are anaesthetic doctors and nurse practitioners, intensive care medicine doctors, emergency medicine doctors, paramedics and military healthcare doctors.
Concept
The responses to findings and recommendations from incident reports and closed claims studies were analysed. Responses included system changes whose primary purpose was to improve patient safety and outcomes in airway management. These included adaptations in monitoring, the use of different or additional equipment, training, ergonomics, the development of guidelines or cognitive aids, changes in practice and the development of new roles or networks.
Context
This review included all healthcare settings in high-income countries including in-hospital and out-of-hospital patient care and primary, secondary and tertiary settings.
Exclusion criteria
Editorials, case reports, case series and trial registrations were excluded from the analysis.
Data extraction
Data were sorted and extracted into an Excel spreadsheet, using the same categories for both conference abstract and full-text analysis (Supplementary material online). The details of the authors, type of article, the incident reporting or closed claims analysis leading to the paper, and the aims and details of the intervention and their effect were extracted by the first author and all extractions were confirmed by one of the second authors. Discrepancies were discussed and resolved with all three authors.
Data synthesis
The extracted data were separated into three main categories: full-text articles, conference abstracts, national guidelines. These categories were reviewed separately using descriptive analytical methods. Where quantitative data were present, for example sample size, and data relating to interventions, descriptive statistical analysis was performed and reported in tables, figures and text. Where descriptions of interventions and outcomes were present, data were iteratively categorised and reported where appropriate and in response to the overarching aims of the study.
Results
The initial search in all databases yielded 28,492 results. After removing 17,154 duplicates, 11,338 titles and abstracts were screened and resulted in 443 articles for review. A total of 100 articles met initial eligibility criteria. Eleven additional full-text articles were included after being identified through the reference review. The review of airway societies and incident reporting websites identified articles that were extracted through the literature review or the citation review. This led to a total of 111 articles proceeding to data extraction, of which 23 were full-text articles, 78 conference abstracts and 10 national guidelines. The analyses of these three types of article were performed separately and are reported as such below. A summary of all results is provided towards the end of this results section.
Full-text articles
The full-text articles included in this review were published between 1992 and 2021 (Figure 3).32 –54 As presented in Table 1, the highest proportion of full-text articles originated in the USA (n = 10; 43%), followed by the UK and Australia (n = 4; 17% from each country). The sample sizes varied significantly, ranging from 28 to 64,718. Six full-text articles had fewer than 100 participants,33,34,38,44,46,53 six had between 101 and 500 participants32,35,39,43,49,52 and one article had 665 participants. 36 In five articles, there were between 2000 and 10,000 participants. These included a multi-centre study, 51 studies running over multiple years37,47,48 and prospective before and after studies across a major tertiary centre. 45 One article included 64,718 perioperative dental incidents collected from a countrywide database from 2010 to 2013. 40
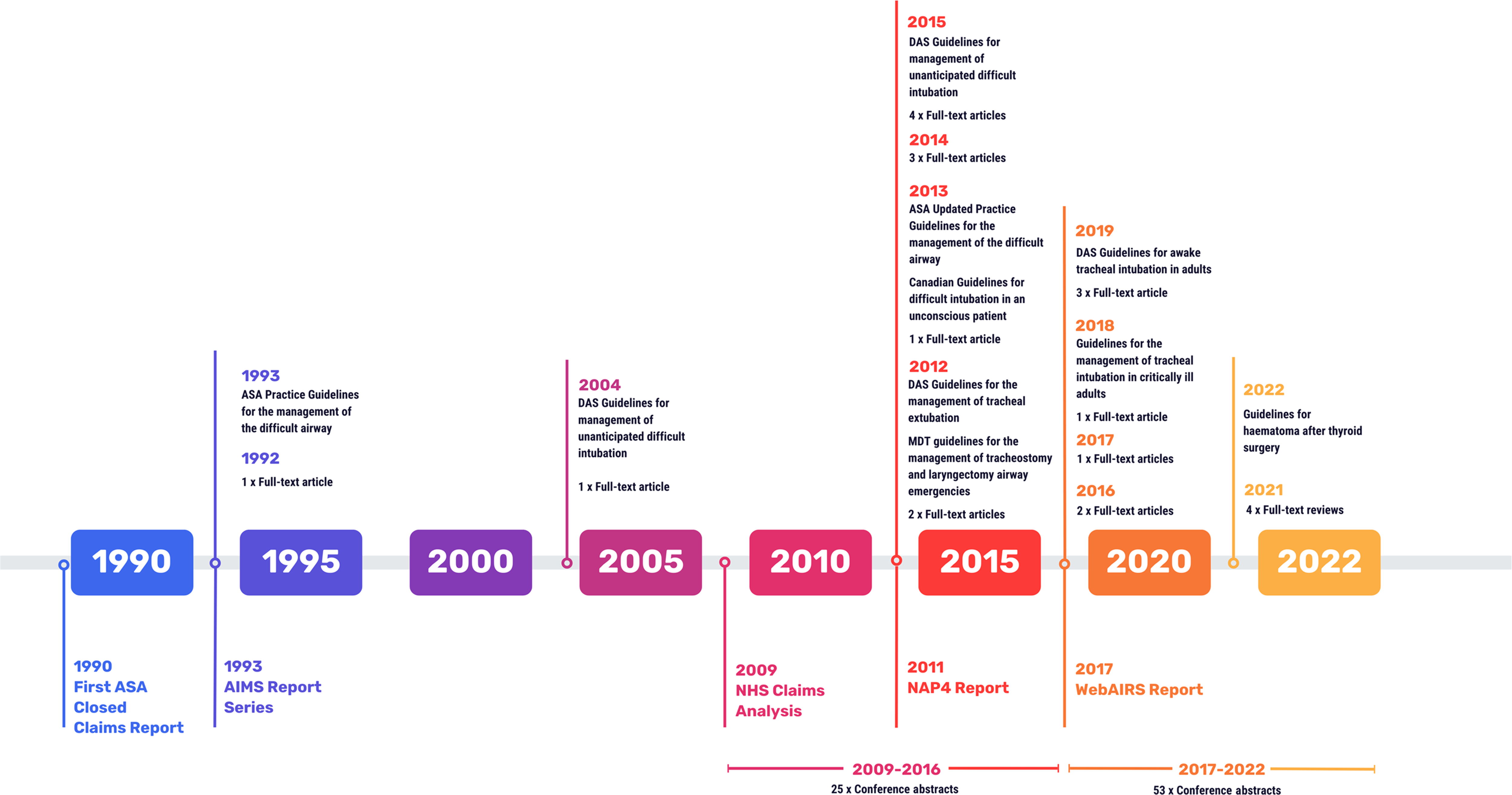
Timeline of publications.
Full-text articles.
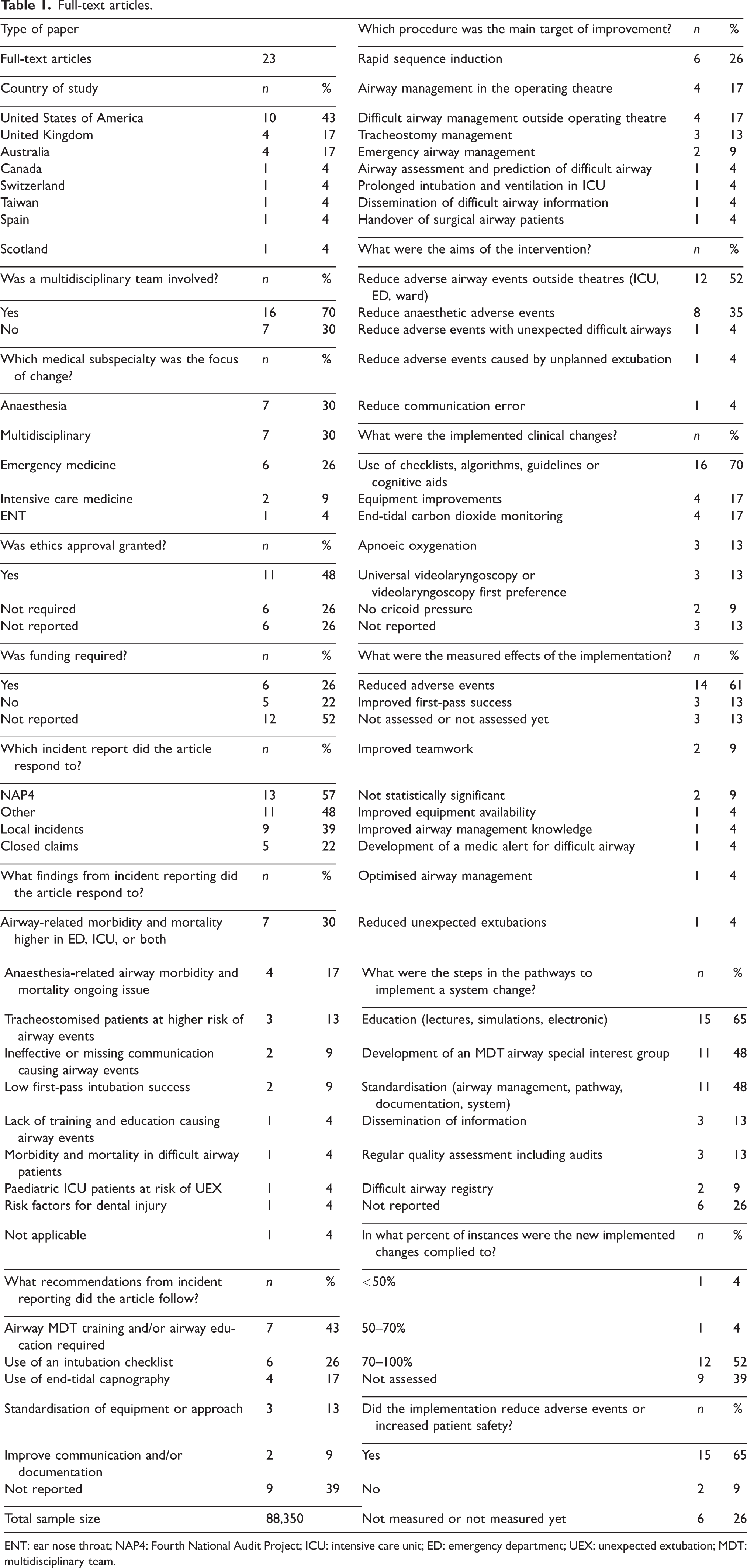
ENT: ear nose throat; NAP4: Fourth National Audit Project; ICU: intensive care unit; ED: emergency department; UEX: unexpected extubation; MDT: multidisciplinary team.
The majority of the studies were undertaken in response to the findings and recommendations of NAP4 (13 of 23 full-text articles; 57%).32 –36,41,43,45,46,51 –54 Examples of recommendations from NAP4 and other incident reports that were responded to included using checklists,34 –36,41,53,54 increasing airway management-related education,32,34,41 –43,47,52 using end-tidal capnography,34,41,46,54, standardising equipment, 32 standardising the approach or algorithm to airway management,34,41 and multidisciplinary team (MDT) training.34,41,43 The most common steps in the pathways to introduce system changes involved MDT special interest groups32 –34,37 –39,41,44,46,47,49 who oversaw structured education programs, improved collecting and disseminating of airway management-related information and organised regular quality assessments and ongoing audit programs.
Most implemented system changes aimed to reduce airway-related adverse events in the ICU, the emergency department (ED) and patient wards, and under anaesthetic care (21 of 23; 91%). One article addressed reducing adverse events caused by unplanned extubations 47 and one aimed to reduce communication errors. 39
More than one-quarter of the full-text articles (n = 6; 26%) addressed rapid sequence inductions in the ED,35,36,38,48,53,54 in addition to improving general airway management in this setting. Anaesthetic airway management and the management of tracheostomies43,44,46 have been identified as other areas requiring improvement. In the ICU, recurring themes that were addressed included increasing the safety of intubation in the critically ill patient 34 and ensuring safe continuous ventilation by avoiding unplanned extubations. 47
Implemented system changes involved the development of standardised algorithms and protocols for airway management, equipment availability, documentation and pathways.
Examples are the implementation of evidence-based care packages and the introduction and consistent use of checklists.34 –36,38,39,45,53,54 Other full-text articles described system changes aiming to improve communication via standardised handover procedures, 39 debriefing protocols 33 and improving dissemination of critical information.42,44,49 Technical aspects addressed included the introduction and consistent use of end-tidal carbon dioxide monitoring for airway management interventions,34,38,41,50,54 apnoeic oxygenation,36,45,48 the universal use of videolaryngoscopy36,48 and a standardised technique to reduce variability in rapid sequence induction. 36 Other articles addressed the changes in equipment availability and the introduction of advanced airway-management devices. Some articles measured compliance with adhering to the newly introduced system changes, which was successful in more than 50% of the included articles.32,33,35 –39,47 –50,52,53
System changes were described in all reports, but their effect on improving patient safety and reducing the number or severity of adverse events was only measured in 17 of the 23 reports,32 –40,43 –45,47,48,50 –52 and successful system changes were found in 15 (65%) of these.32 –40,43 –45,47,48,50 The majority of successful system changes were based on a combination of evidence-based implementation practices and structured and multifaceted education programs led by an MDT and fine-tuned based on clinicians’ feedback, with their effects monitored via an ongoing quality assurance cycle.
The measured effect of the implementation was a combination of a reduction of adverse events (61%),32 –40,43 –45,48,50 improved first-pass intubation success (13%),35,36,48 improved teamwork (9%)36,44 and better equipment availability. 34 The effect of the clinical implementation was not measured in three articles (13%)41,53,54 and was considered insignificant in two (9%).51,52 The number or severity of adverse events was reduced in 15 of these articles (65%),32 –40,43 –45,47,48,50 not measured in six (26%)41,42,46,49,53,54 and unsuccessful or statistically not significant in two (9%).51,52
One article that had unsuccessful results aimed to reduce unexpected difficult intubations by developing an algorithm to improve preoperative airway assessment. Adherence to the new algorithm was found to be less than 50%. 51 The other article, where an implemented change was found to be unsuccessful in achieving its aims, was attempting to reduce the number of adverse events through introducing the Difficult Airway Society (DAS) guidelines to their MDT theatre team via an education program. 52 While initially there was an increase in knowledge and confidence, a re-audit showed no sustained knowledge retention. Consequently, the authors of the study suggested increasing the frequency of delivery of education programs (Table 2).
Full-text articles that described a reduction in adverse airway events.
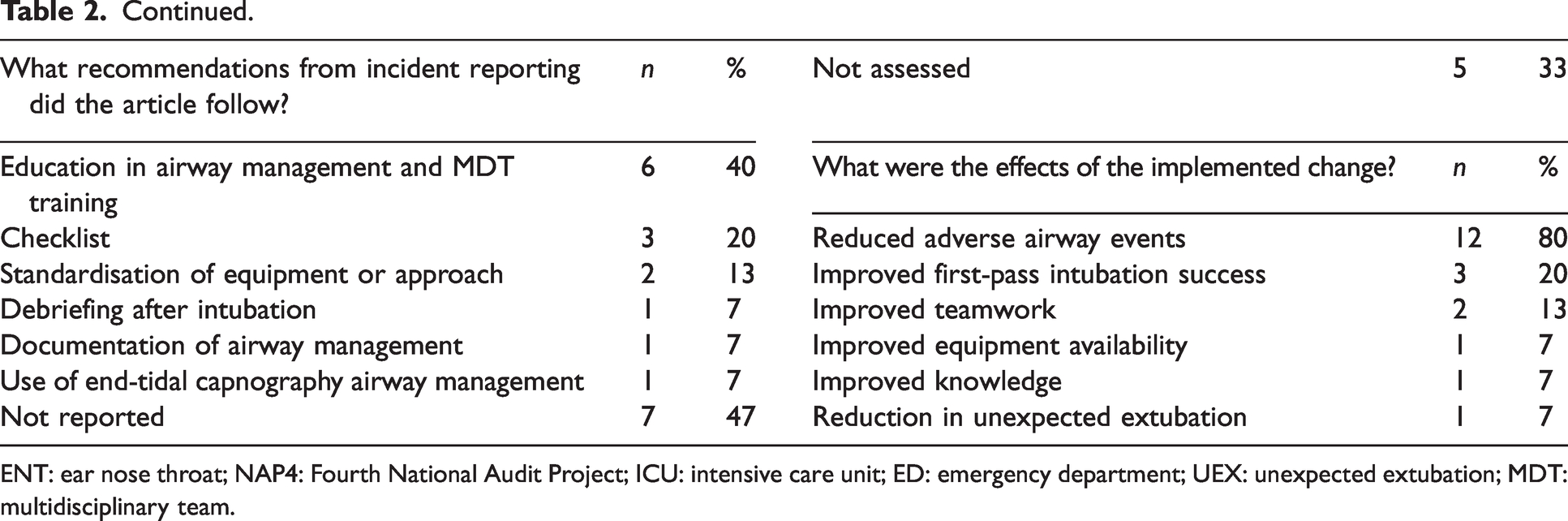
ENT: ear nose throat; NAP4: Fourth National Audit Project; ICU: intensive care unit; ED: emergency department; UEX: unexpected extubation; MDT: multidisciplinary team.
Conference abstracts
There were 78 conference abstracts addressing system changes in airway management. The country in which these studies were undertaken was not reported in over half of the abstracts (n = 42; 54%). Thirty-four (44%) abstracts were from the UK and there was one each from Canada and the USA. Information provided in these abstracts was limited; for example, the sample size was not reported in 24 of the 78 studies. Most of the abstracts reported directly responding to NAP4 data or recommendations (n = 70; 90%) (Table 3).
Conference abstracts.
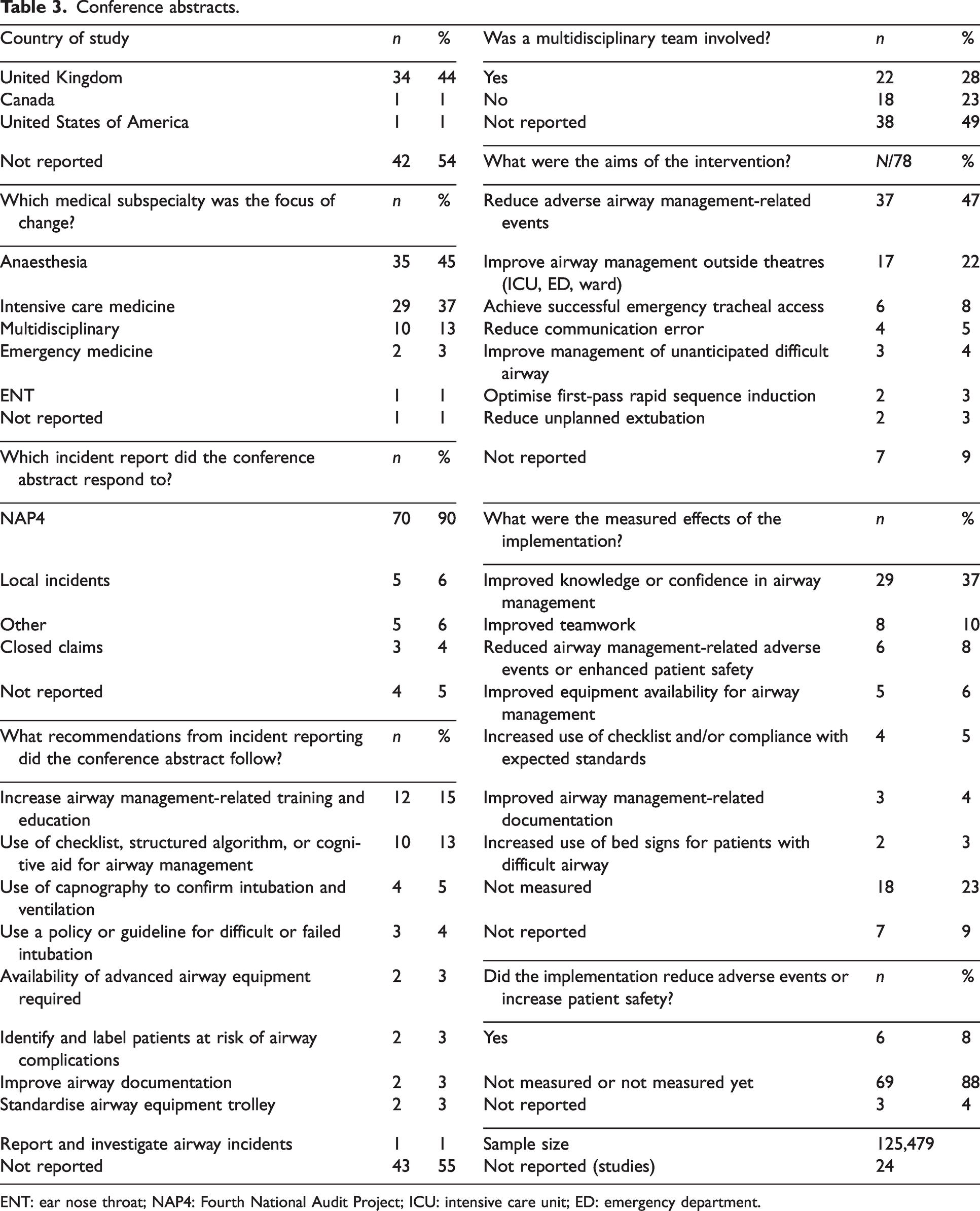
ENT: ear nose throat; NAP4: Fourth National Audit Project; ICU: intensive care unit; ED: emergency department.
While the most common aim identified in conference abstracts was to reduce adverse events, the most common reported effect of the implementations was improved knowledge or confidence in airway management (29 of 78 abstracts; 37.2%). The effect was not measured or reported in 25 (32.1%) of the conference abstracts. The introduced system changes directly improved patient safety in six reports, of which five described a reduction in adverse events and one enhanced patient safety. These six reports addressed changes in emergency medicine and intensive care medicine. The implemented changes included developing and integrating an intubation bundle including a checklist, measures to reduce unplanned extubations, and the use of capnography. Structured and ongoing education plans supported these changes. However, detailed information about the system changes, their implementation pathways and their effects were missing from all conference abstracts (Table 4).
Conference abstracts that described a reduction in adverse airway events.
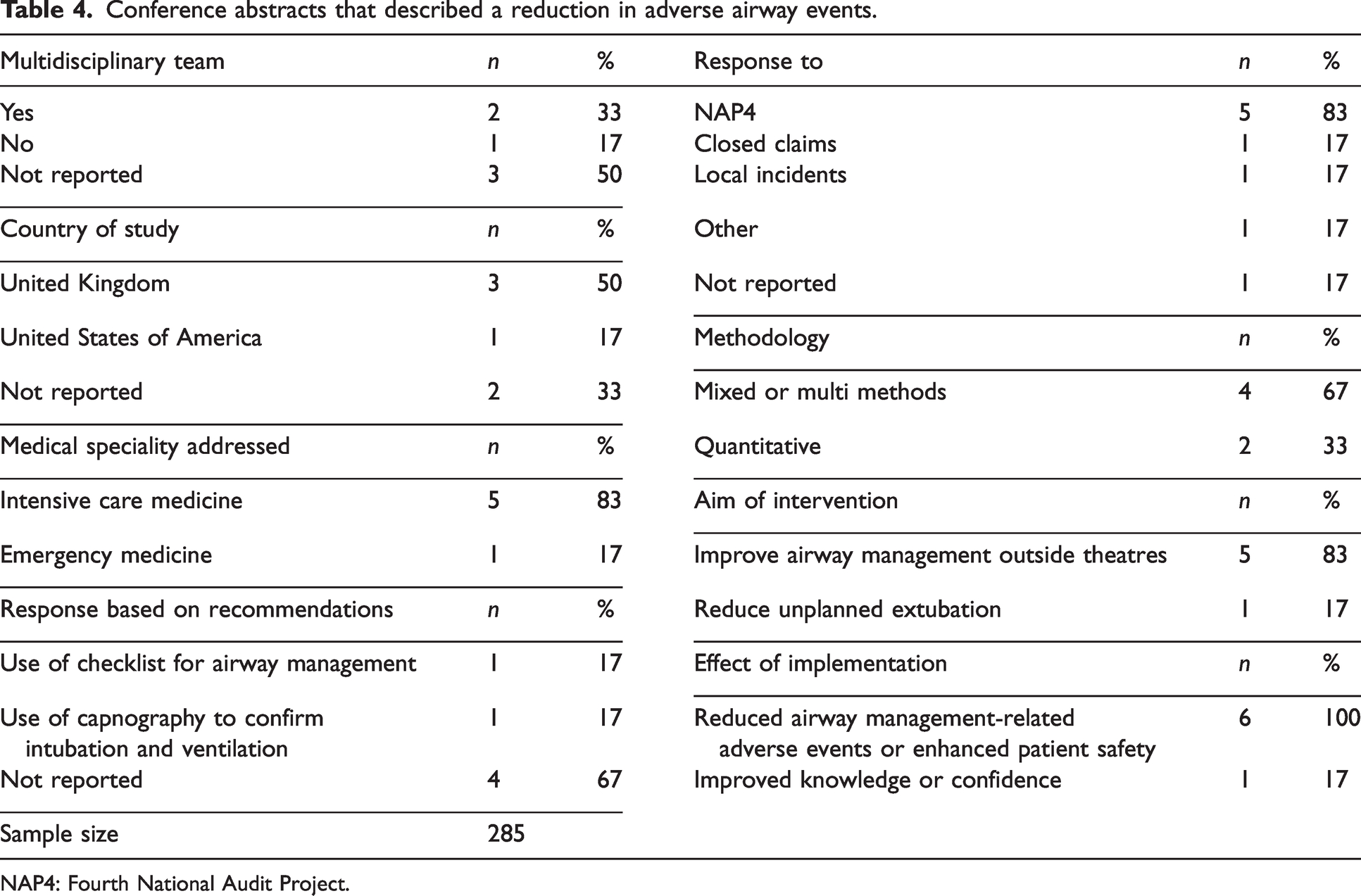
NAP4: Fourth National Audit Project.
Airway management guidelines
This review includes 10 airway management guidelines. The first guideline included was published by the American Society of Anesthesiologists in 1993 55 as a response to findings from closed claims studies. The first DAS guidelines were published in 2004, 56 also following findings from closed claims studies. The remaining eight guidelines were all published within the last 10 (2012 to 2022).57 –64 All guidelines were identified via citation review or searches of airway society websites. Some updated guidelines, not in response to incident reporting, were excluded from this review. Five guidelines published across the USA, UK and Canada addressed difficult or unexpected difficult intubations in anaesthetised patients.55,56,58,60,63 One guideline focuses on the management of extubation, 59 another on awake tracheal intubation techniques, 57 one on the intubation of critically ill patients in ICU, 61 one on the management of post thyroid surgery haematomas 62 and one guideline on the multidisciplinary management of tracheostomy and laryngectomy patients. 64
In this scoping review, the identified guidelines are considered a response to incident reporting or closed claims analyses. However, the measurement of their effects on healthcare systems was outside the scope of this review and would warrant a separate systematic review. Therefore, they have not been included in the detailed analysis.
Discussion
The aim of this scoping review was to explore academic literature that describes system changes in airway management in high-income countries over the last 30 years, based on findings and recommendations from incident reports and closed claims studies. A total of 111 reports were included in the review comprising 23 full-text articles, 10 airway management guidelines and 78 conference abstracts. The outcomes of responses and interventions that addressed data from incident reports and closed claims studies was measured in 1732–40,43 –45,47,48,50 –52 of the full-text articles and reported to be successful in 15 of these.
While 111 reports fitted the inclusion criteria for this review, only 23 were full-text articles describing implemented system changes based on findings and recommendations from incident reporting. Therefore, considering that the literature search spanned over 30 years and airway management is a fundamental skill in anaesthetic, acute and critical care medicine, the findings of this review suggest that system responses related to incident reports and closed claim studies are under-represented in the academic literature. Given that full-text articles linked to conference abstracts could not be located, it is also likely that interventions mounted by health services in response to incident reports are instead conducted as internal quality improvement projects and therefore published only on institutional websites, not easily accessible to the wider community. These observations are supported by Cook et al., who published a survey in 2015 9 measuring the degree to which departmental-level recommendations made in the NAP4 report were implemented nationally in NHS hospitals in the UK. The team reported that the NAP4 led to significant changes across broad areas of anaesthetic, ICU and ED airway practice in more than 90% of the respondents’ hospitals (response rate was 62%). These survey results, combined with the findings of this scoping review, indicate that while there might be implemented system changes based on incident reports, they are not published and distributed in peer-reviewed journals. Consequently, both successful and unsuccessful implementation pathways are not reported to the broader medical community.
These observations have also been highlighted by a recent review from the WHO, 18 which found that publications derived from patient safety incident reporting and learning systems in healthcare mainly focus on recording what went wrong and fail to translate this knowledge into feasible action plans or system changes that are effective.
Conference abstracts were included in the search parameters and the analysis of this review to understand, as comprehensively as possible, what has been reported on this topic. As demonstrated by the proportion of included conference abstracts in this review, it is apparent that a large number of responses to incident reporting were presented at professional conferences. However, while a lot of conference abstracts are published in journals, the information in these abstracts was commonly limited and did not provide sufficient detail for replication of the study, nor a deep analysis of methods or results. While conference presentations are valuable for conveying information, this is only done to a selected group of people at one moment in time, and the broader community cannot access the full context of the studies. Additionally, while the information in the accompanying presentations might be comprehensive, it is often not available to anyone beyond the conference attendees. The lack of distribution of this information is a missed opportunity for other health networks and providers to learn and benefit from the experiences of other health institutions. Sharing of information is an essential part of healthcare safety. There needs to be a mechanism for these local implementation studies to provide insights and information to the larger community. Given that they are most likely written by clinicians, partnering with academics and universities could be considered to enable better distribution of data, resources and implementation strategies to the medical community.
Research has consistently demonstrated that gaps exist between current knowledge of best practice and actual clinical practice. 65 Prerequisites to successfully implementing evidence-based practice include a deep understanding of systems, teams and resources. 65 While most clinicians are experts in patient care, not all are experts in implementation principles and therefore not always best placed to implement changes based on, for example, incident reports. For system learnings to be extracted from incident reports, and successful clinical and system changes to be implemented, a whole-of-system approach is likely always going to be required.
Safety-I and Safety-II principles
There are benefits to analysing incident reporting systems and closed claims analyses. The primary idea behind incident reporting is learning from adverse events and near misses, which has been described as one of the core principles of patient safety management. Furthermore, the findings of incident reporting may reveal weaknesses of the systems involved. Incident analyses can lead to the root causes of errors, which consequently can form the basis of quality improvement actions. Closing the loop by reanalysing adverse events after a system change has occurred can also indicate the effectiveness of the implemented changes. The responses in this scoping review were to findings and recommendations from the NAP4, various other airway incident reporting systems, local reporting systems and closed claims analyses. The findings of those were that airway-related morbidity and mortality are higher in events outside the operating theatres and that airway incidents in anaesthesia are still an ongoing issue. Recommendations were to initiate multidisciplinary airway-related education and training, use intubation checklists and end-tidal capnography, and standardise practice, algorithms and equipment. Consequently, most studies described in full-text articles aimed to reduce adverse airway events by introducing these recommendations into their respective health systems, targeting various areas of airway management.
Successful implementation pathways included the introduction of bundles involving standardised airway management algorithms and equipment, enforced by a variety of ongoing multidisciplinary education and training sessions that were supported and overseen by specifically established MDT airway special interest groups. These responses are categorised as adhering to Safety-I principles. 26 The focus lies on what went wrong, by analysing mechanisms that led to these incidents and aspiring to identify solutions to prevent these incidents from reoccurring.
Over the last 30 years, reports on airway incidents have focused on finding and improving the parts of airway management that went wrong and providing solutions, suggestions, recommendations and guidelines to prevent these incidents from happening again.1 –5,7,10 –17,66 –72 Multiple models have been used to explain how airway management might go wrong, with a well-known example being Reason’s Swiss cheese model.1,23 The aim is to prevent the transition from a safe and controlled situation to an unsafe, uncontrolled situation. Standardised processes, including intubation checklists and protocols, including difficult airway management guidelines, have been developed and are recommended to be established system-wide.48,53,55 –59,64,73 The results of analyses following Safety-I principles provide information on how airway incidents happened and recommendations about what must be done to prevent these incidents from happening again. This approach has been classified as the ‘find and fix’ approach, and the number of adverse events defines the measure of safety when focusing on Safety-I principles.26 –29,74 Closing the loop after establishing Safety-I-derived solutions requires measuring the effect of the implementations, which are deemed successful if the number or severity of adverse events has reduced.
This scoping review did not identify any reports relating to Safety-II events in airway management, likely due to the focus on incident reporting. These are instances where airway management went well or when clinicians adjusted their strategy to undesirable conditions or unexpected events, and the patient did not come to harm. It is remarkable how often airway management is successful, despite the ever-increasing complexity of patient comorbidities and surgeries, and the ongoing development of new standards, pathways, surgical procedures and requirements for airway management. Safety-II analysis is learning from success and realising that performance variability in airway management is required, omnipresent, and therefore not interpreted negatively. 26 As airway management possibilities continue to expand with new guidelines, equipment and complex surgeries, these adjustments become increasingly crucial for safe airway management and therefore present both a challenge and an opportunity for safe patient care. Reviewing Safety-II events contradicts the traditional focus on failures and errors and has received less attention in the current literature.26 –29,74 However, airway incidents are rare1 –3,8,10,11,13,14,16 and by focusing only on Safety-I principles, analysers miss out on information provided by the many more events that went well. Safety-II events could be explored by interrogating incident reporting systems for no-harm events, unsafe condition events or near misses. Two recent reviews of airway incidents across Australia and New Zealand using the webAIRS incident database2,3 included such events where the patient did not come to harm. In one of the reviews, 18 (16.2%) ‘unsafe conditions’, defined as any circumstance that increases the probability of a patient safety event but did not progress to such, were mentioned.
Another option to include Safety-II principles in airway management would be to expand incident reporting systems to include information about every airway intervention, thereby creating an airway management registry or database.
Safety-I and Safety-II principles complement each other and therefore complete the concept of airway incident analysis. Thus, research should not only find and address errors (Safety-I) but also look for successful variations of practice (Safety-II) to understand how airway management commonly goes well, and to form a basis for explaining how occasionally events go wrong.
Recommendations
After reviewing the available literature, we make three recommendations. First, we encourage clinicians involved in airway management to partner with researchers and academic institutions to facilitate the design and investigation of implementation strategies for the improvement of system responses to airway management. Second, we recommended that action plans, implementation projects and system changes based on findings and recommendations from airway incident analyses are published, whether successful or unsuccessful, in accessible peer-reviewed journals. Third, we encourage the formal and systematic exploration of both Safety-I and Safety-II principles in the analyses of airway management incident reports and databases.
Limitations of this study
There are several potential limitations to this scoping review. First, although the authors followed evidence-based methods, it is possible that relevant studies were missed as a result of the search terms and databases that were used. Additionally, reports highlighting institutional system changes might be published in grey literature or on local reporting websites. While the authors searched relevant websites, it is possible that some information was missed or not accessible. Second, this review aimed to identify responses to incident reports and closed claims reports; it did not include the responses to airway registries, examples being the National Emergency Airway Registry for Children 75 or the Australian and New Zealand Emergency Department Airway Registry. 76 Also, while some single case reports, like Elaine Bromiley’s death, 77 triggered significant airway management changes, they were equally excluded in this scoping review. Finally, a large proportion of extracted articles were conference abstracts. As a result, the information and content provided were inconsistent and often insufficient to extract meaningful results. Consequently, the main focus of this review was on studies that were reported in full-text articles.
Conclusion
Incident reporting and analysis is well established in high-risk industries including aviation, in nuclear power plants, scuba diving and healthcare.20,21,23,25 The main reason for reporting incidents is to learn from incidents and near misses and establish action plans to reduce the risk of patient harm and its occurrence. 18 However, this review has shown that while findings and recommendations from airway incident analyses are commonly published, there is a gap in the literature regarding the resulting action plans, successful implementation projects and system changes that reduce adverse events in airway management. Closure of this gap is required to disseminate this valuable information to improve healthcare processes and enhance Safety-I.
Currently, airway safety management mainly focuses on the few adverse events rather than all of the interventions where no harm has occurred, thereby not considering Safety-II principles. Hollnagel et al. state in their white paper: ‘Focusing on the lack of safety does not show us which direction to take to improve safety.’ 26
By responding only to incidents and adverse events, the healthcare community is neglecting all of the information available from situations where airway management went well, potentially missing out on a significant opportunity to improve patient safety and care.
Supplemental Material
sj-xlsx-1-aic-10.1177_0310057X241227238 - Supplemental material for The nature of the response to airway management incident reports in high income countries: A scoping review
Supplemental material, sj-xlsx-1-aic-10.1177_0310057X241227238 for The nature of the response to airway management incident reports in high income countries: A scoping review by Yasmin Endlich, Ellen L Davies and Janet Kelly in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The authors thank Professor Pam Macintyre, Dr Martin Culwick, Dr Chris Acott and Dr Simon Macklin for their review and comments on this article. The authors would also like to acknowledge the support of Vikki Langton (University of Adelaide) with the literature search. Finally, we would like to acknowledge all the clinicians reporting, analysing and responding to incidents in the interest of greater patient safety.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or pub- lication of this article: YE is Medical Director of the Australian and New Zealand Tripartite Data Committee (ANZTADC) managing webAIRS. No conflicting interests exist for the remaining authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix 1. Literature search parameters.
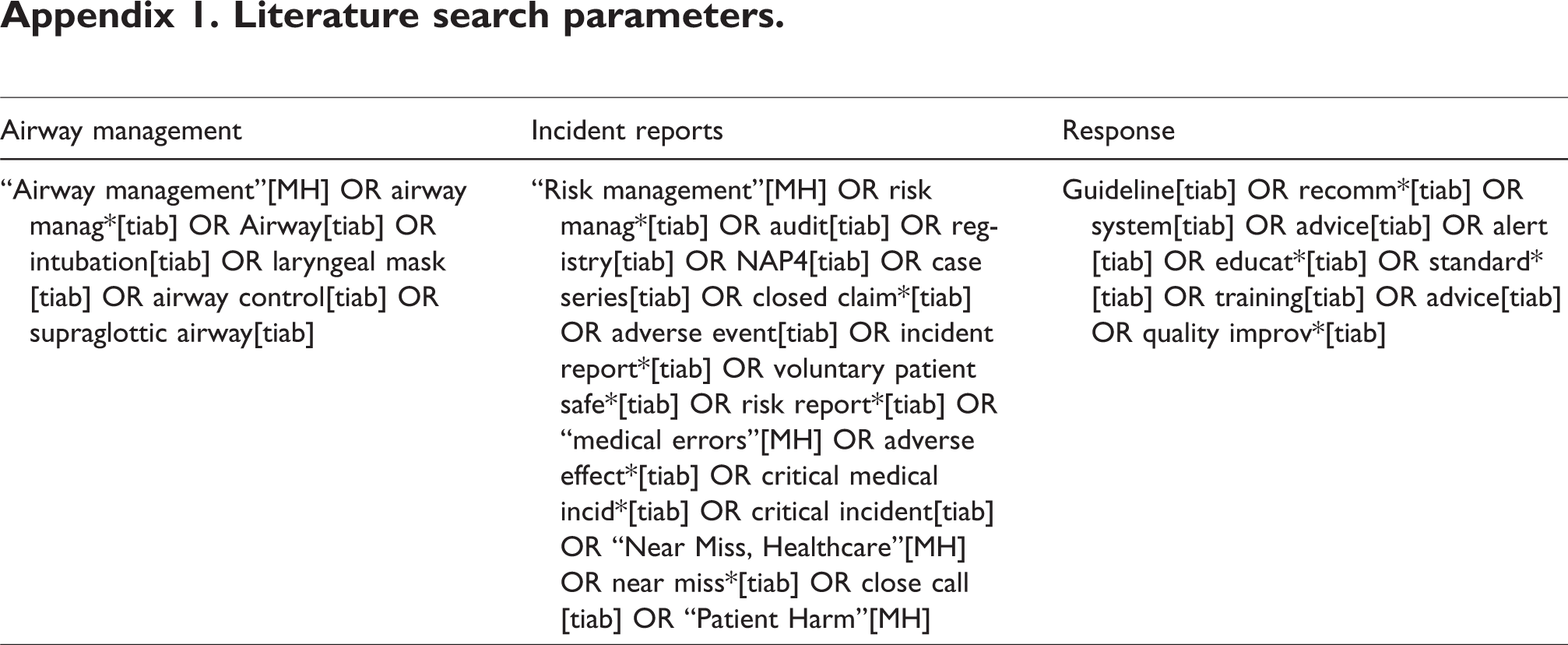
| Airway management | Incident reports | Response |
|---|---|---|
| “Airway management”[MH] OR airway manag*[tiab] OR Airway[tiab] OR intubation[tiab] OR laryngeal mask[tiab] OR airway control[tiab] OR supraglottic airway[tiab] | “Risk management”[MH] OR risk manag*[tiab] OR audit[tiab] OR registry[tiab] OR NAP4[tiab] OR case series[tiab] OR closed claim*[tiab] OR adverse event[tiab] OR incident report*[tiab] OR voluntary patient safe*[tiab] OR risk report*[tiab] OR “medical errors”[MH] OR adverse effect*[tiab] OR critical medical incid*[tiab] OR critical incident[tiab] OR “Near Miss, Healthcare”[MH] OR near miss*[tiab] OR close call[tiab] OR “Patient Harm”[MH] | Guideline[tiab] OR recomm*[tiab] OR system[tiab] OR advice[tiab] OR alert[tiab] OR educat*[tiab] OR standard*[tiab] OR training[tiab] OR advice[tiab] OR quality improv*[tiab] |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.