
Abstract
A review of the first 4000 reports to the webAIRS anaesthesia incident reporting database was performed to analyse cases reported as difficult or failed intubation. Patient, task, caregiver and system factors were evaluated. Among the 4000 reports, there were 170 incidents of difficult or failed intubation. Difficult or failed intubation incidents were most common in the 40–59 years age group. More than half of cases were not predicted. A total of 40% involved patients with a body mass index >30 kg/m2 and 41% involved emergency cases. A third of the reports described multiple intubation attempts. Of the reports, 18% mentioned equipment problems including endotracheal tube cuff rupture, laryngoscope light failure, dysfunctional capnography and delays with availability of additional equipment to assist with intubation. Immediate outcomes included 40 cases of oxygen desaturation below 85%; of these cases, four required cardiopulmonary resuscitation. The majority of the incidents resulted in no harm or minor harm (45%). However, 12% suffered moderate harm, 3.5% severe harm and there were three deaths (although only one related to the airway incident). Despite advances and significant developments in airway management strategies, difficult and failed intubation still occurs. Although not all incidents are predictable, nor are all preventable, the information provided by this analysis might assist with future planning, preparation and management of difficult intubation.
Keywords
Introduction
Management of the difficult airway, whether expected or unexpected, is a core skill for all anaesthetists. Currently there is no single test of sufficiently high sensitivity and specificity to predict a difficult airway reliably and ‘standard bedside tests' are poorly predictive for a difficult intubation. 1 , 2 Difficult intubation has been reported to occur in about 1%–6.2% of all general anaesthetics3–7 and the incidence of failed intubation is as high as 1 in 1000–2000 general anaesthetics. 1
Preoperative assessment is an integral part of anaesthetic management, which includes an assessment of patient factors, task factors, system factors and caregiver factors. Anaesthetists have a range of fundamentals for advanced airway management equipment at their disposal. Various airway societies worldwide have published algorithms for the management of unexpected difficult intubations, including guidelines for the structured use of airway devices.8–11 Cognitive aids complement and facilitate the use of these existing airway algorithms in real time. 12 Therefore, anaesthesia has become increasingly safe and significant complications of airway management are rare. However, they have the potential to be life-threatening and may cause significant harm, including death.2,13,14
WebAIRS is an internet-based voluntary de-identified anaesthetic incident recording system used by anaesthetists in Australia and New Zealand. It is owned and funded by three organisations: the Australian and New Zealand College of Anaesthetists (ANZCA), the Australian Society of Anaesthetists and the New Zealand Society of Anaesthetists. Registered anaesthetists across Australia and New Zealand have been able to report anaesthetic incidents via the webpage www.anztadc.net since 2009. Data describing the incidents can be entered both via non-mandatory tick boxes and in the form of text, allowing reporters to describe the incident in their own words and providing opportunity for reflections about contributing and mitigating factors.
An overview of the first 4000 incidents was published in 2017. The aim of this paper is to report on the analysis of all incidents coded as ‘Difficult Intubation’ or ‘Failed Intubation’ in the first 4000 reports.
Methods
This study assessed all incidents coded as ‘Difficult Intubation’ or as ‘Failed Intubation’ in the first 4000 reports logged on the webAIRS system. Data were collected in compliance with the National Health and Medical Research Council recommendations for quality assurance data. The methods of de-identified data collection have been reported previously. 15 Multicentre ethics approval is maintained at the Royal Brisbane and Women's Hospital Human Research Ethics Committee (HREC/11/QRBW/311) and the Nepean Blue Mountains Local Health District (HREC/12/NEPEAN/18). In New Zealand, ethics approval has been obtained from the Health and Disability Ethics Committee (MEC/09/17/EXP).
Denominator data are not collected by webAIRS and the numerator data are submitted voluntarily, which precludes absolute risk calculations. However, as described in a previous article, 16 it is possible to use the denominator data from other patient-related incidents (in this case, not difficult or failed intubation incidents) in the webAIRS database as a surrogate denominator, acknowledging that this may not represent population-based denominator data. In effect, demographic data of patients involved in the difficult or failed airway incidents were related to the demographics of patients in the database who were involved in other incidents. In each case, the incidents were drawn from the first 4000 incidents reported. Risk ratios (RR) were then calculated.
The data coded by the reporters as ‘Difficult Intubation’ or as ‘Failed Intubation’ were extracted from the first 4000 reports in the webAIRS database. The reports were assessed and analysed by all authors and reports were excluded based on duplication of data, irrelevance, or insufficient detail for analysis. Two of the 172 reports were identified as duplicates: in both cases they were submitted within a short time frame of each other, had the same age group and gender and had similar descriptions of the incident.
The remaining reports were analysed, assessed and categorised by all authors.
The authors defined an incident as failed intubation if any one of the following three conditions occurred during the attempted intubation.
The patient had to be woken up, or when the final airway device was either a facemask, a supraglottic airway device (SAD), or a subglottic front-of-neck rescue. Any incident initially involving direct or indirect laryngoscopy techniques but subsequently requiring rescue intubation using a fundamentally different technique such as an intubating laryngeal mask airway (ILMA, Fastrach™, Intavent Ltd, Reading, UK), a fibreoptic intubation (FOI) device, or front-of-neck access (FONA). Unsuccessful elective FOI.
All reports were analysed using paradigm grouping of ‘potential risk factors’, ‘management’ and ‘outcomes’. Analysis of potential risk factors was further divided into ‘patient factors', ‘task factors', ‘caregiver factors' and ‘system factors’. Analysis of management was divided into ‘immediate management', ‘airway technique' and ‘targeted other’, which included the mentioning of cognitive aids, the use of muscle relaxants and optimisation of positioning and facemask ventilation.
These were then examined and assessed by all authors.
Results
Of the 4000 reports, 71 were omitted from this study as they did not involve an individual patient. Of the remaining 3929 webAIRS incidents, 170 reported difficulties encountered during endotracheal intubation. Of these cases, 108 (63.5%) were analysed as ‘difficult intubation' and 62 (36.4%) as ‘failed intubation’. The demographic data from these 170 patients were compared to the demographic data of the remaining patients (3759) to calculate the RR related to specific risk categories.
There was almost even gender distribution (Table 1). As this was also the case with the remainder of the reports in the webAIRS database, the RR for either males or females having a difficult or failed airway event approached one. The American Society of Anesthesiologists physical status (ASA PS) had little effect on the RR of having a difficult or failed airway event (Table 2). The RR for ASA PS 1 was 0.73 and for ASA PS 2 1.33, with ASA PS 3 and ASA PS 4 both within this range. Most patients were ASA PS 2 or 3. The patient age category 40–59 years was associated with an increased RR of a difficult or failed airway event (1.65, Table 3). Age <17 years and >79 years had a reduced RR, but the number of incidents with patients in these age categories was very low. The highest proportion (38%) was for the 40–59 years category followed by 60–79 years (28%) and 17–39 years (20%).
Sex of patients involved in the reports.
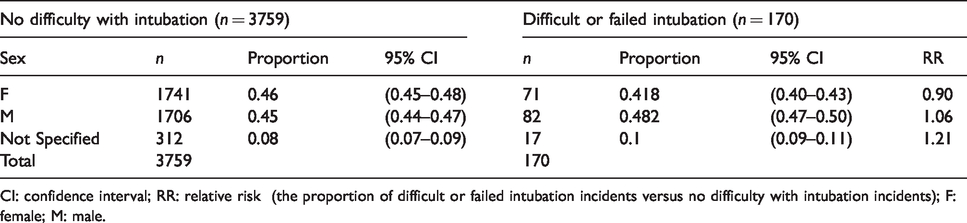
CI: confidence interval; RR: relative risk (the proportion of difficult or failed intubation incidents versus no difficulty with intubation incidents); F: female; M: male.
American Society of Anesthesiologists physical status classification of the patients involved in the reports.
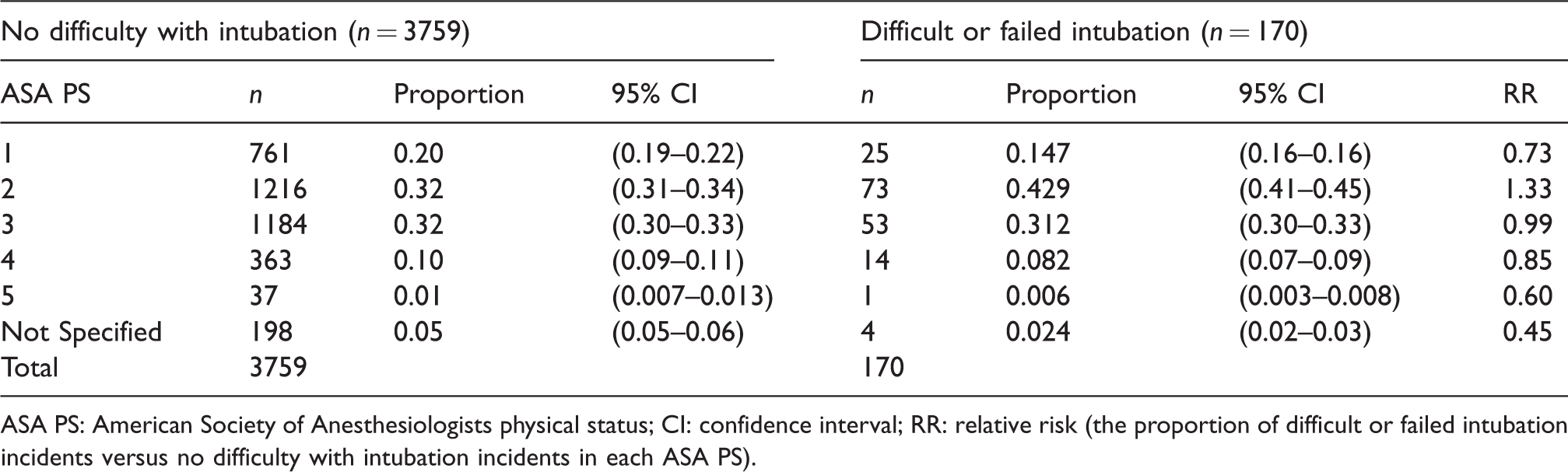
ASA PS: American Society of Anesthesiologists physical status; CI: confidence interval; RR: relative risk (the proportion of difficult or failed intubation incidents versus no difficulty with intubation incidents in each ASA PS).
Age of the patients involved in the reports.
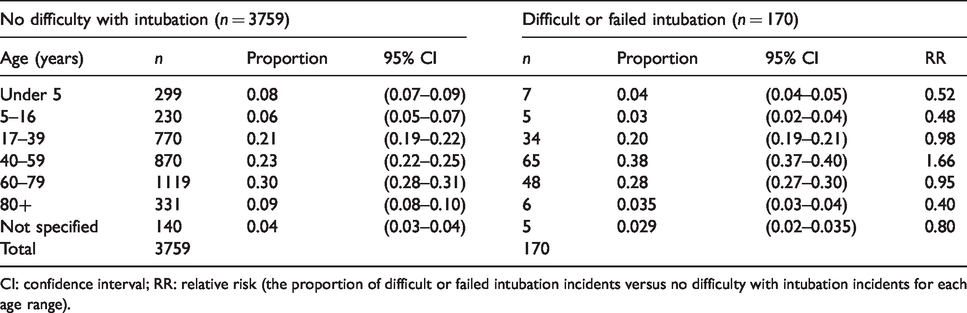
CI: confidence interval; RR: relative risk (the proportion of difficult or failed intubation incidents versus no difficulty with intubation incidents for each age range).
Of the events categorised as difficult or failed intubation cases, 40% occurred in patients with a body mass index (BMI) >30 kg/m2 (Table 4). A total of 14% of the reports did not specify a BMI. The RR of a difficult or failed intubation event for incidents in which patients had a BMI >30 kg/m2 was 1.66 and for patients with a BMI 25–30 kg/m2 was 1.20, suggesting that higher BMI was associated with a higher proportion of difficult and failed intubation compared with patients having other incidents. The Australian Institute for Health and Welfare (AIHW) national BMI data for adults 17 indicate that the proportion of Australians with a BMI >30 kg/m2 for the years 2007–2008, 2011–2012 and 2014–2015 was 24.4%, 27.2% and 27.5% respectively. The webAIRS data were collected over this period (2009 to mid-2016). The average proportion of BMI >30 kg/m2 in the AIHW data was 26.4%, which is numerically close to the proportion of patients with a BMI >30kg/m2 having non-airway events in the first 4000 incidents in the webAIRS database (24%).
Body mass index of patients with and without intubation difficulty.
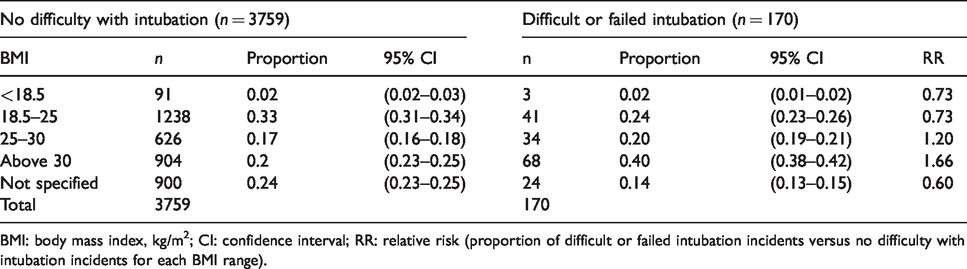
BMI: body mass index, kg/m2; CI: confidence interval; RR: relative risk (proportion of difficult or failed intubation incidents versus no difficulty with intubation incidents for each BMI range).
Of the difficult or failed intubation events, 41% occurred in patients undergoing emergency procedures compared with 33.5% of patients in the remainder of the database undergoing emergency procedures (RR 1.23) (Table 5).
Urgency of the procedure involved.
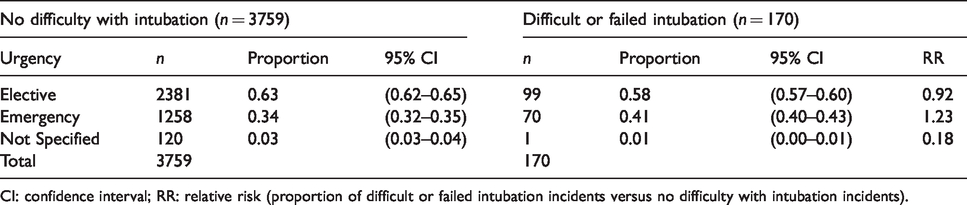
CI: confidence interval; RR: relative risk (proportion of difficult or failed intubation incidents versus no difficulty with intubation incidents).
A total of 80% of the incidents occurred while under the care of an anaesthetic specialist; 86% of patients were undergoing general anaesthesia for their planned procedure.
Of all incidents, 92% occurred in the operating theatre and 5% in remote areas (in 3% the site was not specified). A rapid sequence induction (RSI) was performed in 30% of incidents, mostly in emergency cases. In a minority of cases, RSI was not mentioned in association with an emergency case. Significant time pressure to secure the airway was described in 21% of incidents.
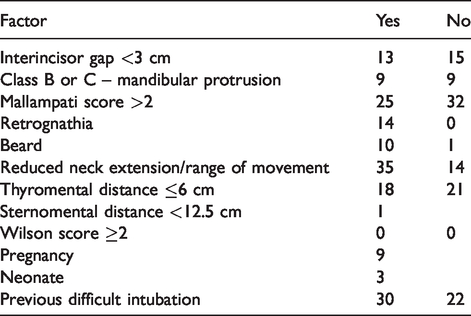
In 66% of incidents, at least one predictive risk factor (based on clinical examination or history) was reported as positive for patients with difficult or failed intubation. In 10% of difficult or failed intubation incidents, no predictors were included in the report, and in 24% no airway assessment was mentioned. In 38% of difficult or failed intubation incidents at least one anatomical risk factor was recorded and in 18% patients had a previous history of a difficult airway (Table 6). In 56% of difficult or failed intubation incidents, the difficult airway was not anticipated.
Predictive risk factors for difficult or failed intubation incidents.
In 14 incidents (8.2%), the anaesthetist had worked for 10–16 hours at the time of the incident. In two incidents the anaesthetist had worked more than 16 hours (Table 7). Fatigue was mentioned in 14% of the reports. A total of 32 incidents (19%) occurred after hours and there was a high RR (1.8) in the time block 22.00 to 07.59 hours (Table 8).
Hours on duty of anaesthetist when incident occurred.
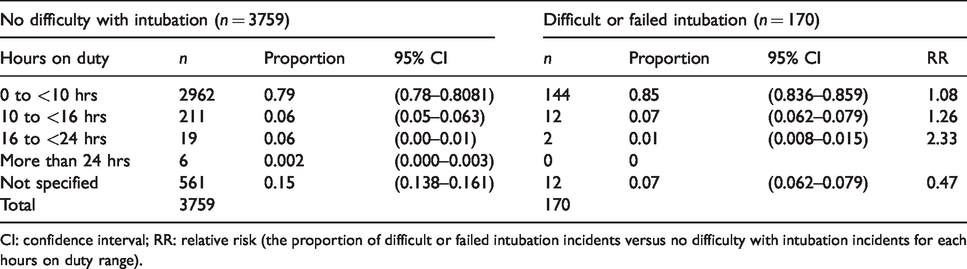
CI: confidence interval; RR: relative risk (the proportion of difficult or failed intubation incidents versus no difficulty with intubation incidents for each hours on duty range).
Time of day of incident.
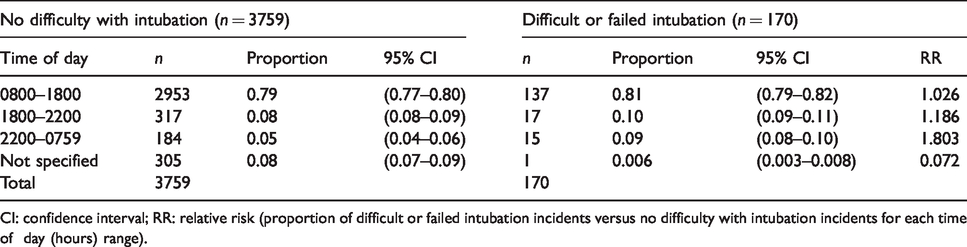
CI: confidence interval; RR: relative risk (proportion of difficult or failed intubation incidents versus no difficulty with intubation incidents for each time of day (hours) range).
Human factors were described in a small proportion of events. A total of 36 reports (21%) described significant pressure to proceed. Of incidents, 31 (18%) reported equipment problems affecting either basic or advanced airway management devices. Requested equipment was unavailable in 13% of incidents. Team and communication issues were reported in 18% of incidents.
The initial successful oxygenation method (when the planned airway strategy failed) was facemask ventilation in 71 incidents (41.8%). In 22 (12.9%) it was ventilation via an SAD, in five (3%) it was endotracheal intubation, and subglottic airway access was obtained in two incidents (1.2%). An SAD other than an ILMA was described as part of airway management in 35.3% of reports and was successful in restoring ventilation in 20.6% of incidents. In 12% of reports, attempts at ventilation using an SAD failed. The ILMA was used in 15 of the reports (8.8%) and provided successful ventilation in ten. Blind intubation through an SAD or ILMA was successful in one incident and failed in two. Bronchoscopy-guided intubation via an SAD or ILMA was successful in ten incidents and failed in five.
The final airway device used was an endotracheal tube in 137 incidents, facemask in 11, SAD in 16, and subglottic access in five events. The airway of one patient could not be rescued by any technique and the patient died.
The anaesthetist elected to wake up the patient in 20 incidents, of which three proceeded to an awake fibreoptic intubation and another two were intubated by a different operator. In ten incidents the anaesthetist was able to proceed without an endotracheal tube and in five incidents emergency FONA was required.
More than three intubation attempts were described in 43 incidents (25%) and more than four in 13 (7.6%). In seven reports there were more than five attempts specified. A muscle relaxant was used electively in 136 of the incidents and as part of airway rescue management in five. In 99 incidents (58%) the anaesthetist used at least one type of videolaryngoscope (VL) of which 31 (18.2%) were unsuccessful. A total of 47 reports (27.6%) described the use of a fibreoptic technique, 12 electively (7%) and the remaining 35 (20.6%) unplanned as part of the airway crisis management.
In 40 incidents (23.5%) the oxygen desaturations were reported to fall below 85% during the airway manoeuvres, of which four were associated with cardiac arrest. Patients were reported to suffer from minor harm in 45% of incidents, moderate harm in 12% and severe harm in 3.5%. In 7.6% of reports, whether harm occurred was not specified. There were three deaths. Six patients (3.5%) suffered from a permanent injury as assessed by the authors (based on the information provided in reports). The reporters considered 39% of the incidents preventable.
Discussion
Of the first 4000 incidents reported to webAIRS, 4.25% were coded as difficult or failed intubation. This is similar to the percentage of ‘difficulty with intubation’ incidents published in the AIMS report in 1993. 18 However, neither AIMS nor webAIRS data indicate the risk of an incident occurring. Both systems rely on voluntary reporting so the numerator for any risk calculation cannot be ascertained. Similarly, the denominator is not known. This is because the incidents are de-identified and data on the number of episodes of anaesthesia care performed by individual anaesthetists reporting across sites is not known. Nevertheless, the webAIRS data suggest the number of incidents categorised as difficult or failed intubation still require attention. As expected, the majority of reported incidents occurred while under the care of a specialist anaesthetist and most occurred when patients were undergoing general anaesthesia. However, incidents often remain unpredictable and many are not preventable. Outcomes range from near misses and minor harm, to severe harm in a minority of cases and even death.
Difficult versus failed intubation
Various airway societies worldwide have published slightly different definitions of what constitutes a ‘Difficult intubation’ and what is defined as a ‘Failed intubation’. 6 ,8–11 Assessment of the narratives showed there was inconsistency in the definition by reporters as well. Therefore, the authors decided to create a definition that was not ambiguous for the purpose of this analysis. The definition was designed to detect a failure of any method that constituted the initial intubation plan and required rescue by a different technique or operator. The incident was counted as a failed intubation if the final airway device was not an endotracheal tube or if the patient had to be woken as part of unsuccessful intubation attempts, irrespective of the initial method chosen. Equally, any incident where direct or indirect laryngoscopy guided intubation attempts were unsuccessful and subsequently required asleep airway rescue using a different technique such as an ILMA, FOI or FONA. Conversely, there were also cases of elective FOI methods that failed and were rescued by different methods of oral intubation.
Demographic predictors: Gender ASA PS and age
There was no apparent gender bias (Table 1). The ASA PS had little influence, although there were very few incidents in the ASA 4 and 5 categories (total 15) to adequately assess these potential predictors. Most of the difficult and failed airway intubation incidents occurred in patients between 40 and 59 years of age (38.2%). The RR of a difficult or failed intubation incident occurring in this age range versus non-airway incidents occurring in this age range was 1.65, possibly indicating this age group might be at higher risk of airway events. There were too few patients in the below 5 years and >80 years age range (seven and six respectively) to adequately assess the influence of these potential predictors. Airway management in paediatric patients is usually considered straightforward unless there are congenital abnormalities or acute injuries or infections affecting the airway. In this cohort, all but one of the paediatric patients was either suffering from a congenital syndrome, had undergone surgeries on the head or neck, or presented with acute airway bleeding or swelling. Three of the patients were neonates requiring urgent resuscitation and intubation.
Airway assessment and prediction of difficult intubation
More than half of the difficult intubations identified in this study were not predicted. As reporters did not need to provide details of airway assessment, it is not possible to comment on the relationship between pre-operative airway assessment and the likelihood of incidents. However, 30 patients had documentation describing previous difficult airway management. Findings from the Danish Anaesthesia Database have shown that previous difficult tracheal intubation is associated with a six-fold increase in the likelihood of being difficult again and a previous failed intubation is associated with a 22-fold increase in the likelihood of failed intubation in future procedures. 19
Body Mass Index
Patients with a high BMI were highly represented in the reports. About 40% of the incidents were reported in patients with a BMI >30 kg/m2. The RR of a difficult or failed intubation incident occurring in patients with a BMI >30 kg/m2 versus non-airway events occurring in patients with a BMI >30 kg/m2 was 1.66. The proportion of BMI >30 kg/m2 in the AIHW 17 national health surveys during the same period of the webAIRS incidents reports was an average of 26.4%, which is close to the 24% across the 4000 webAIRS reports.
A previous review of 50,000 anaesthetics described a BMI >25 kg/m2 as an independent risk factor for difficult facemask ventilation. 20 Results were similar in this report. Of the 170 patients (60%), 102 had a BMI >25 kg/m2. Airway management was difficult in 64 and intubation failed in 38 of these 102 patients. A third of these patients then suffered from adverse sequelae resulting from airway management, ranging in severity from minor airway trauma to aspiration, to intensive care unit (ICU) admission and FONA access. Although obesity alone may not be considered a standalone predictor of difficult tracheal intubation, 21 this series shows it is still prevalent across difficult and failed airway incidents.
Emergency and urgent cases
A proportion of the procedures were performed under stressful conditions, with 36 reports describing significant pressure to proceed. Most of these pressured circumstances, difficulties in teamwork and poor communications were reported. It was a recurrent issue that findings of a previous airway assessment were not communicated or missed by the treating anaesthetist.
A high percentage (41%) of the incidents coded as difficult and failed intubation were classified as emergency cases. This is consistent with other studies; previous literature has shown that rates of airway complications, including difficult intubation and the risk of aspiration, are increased in emergency cases. 2 , 13 , 14 , 16 The RR of a difficult or failed airway incident occurring during an emergency procedure versus a non-airway incident occurring during an emergency procedure was 1.23. However, it is likely that emergency procedures are more highly represented than elective procedures across the webAIRS database.
Fatigue is known to affect performance reducing vigilance and the accuracy of response, thereby contributing to adverse events.22–26 Fatigue was reported in 14% of incidents as a contributing factor. Although most of the incidents occurred during daylight hours, about 19% occurred after-hours (1800–0759 hours), compared with 13.3% of non-airway incidents occurring in this time of day range (RR 1.41). A total of 10% of the incidents occurred when anaesthetists had been working 10–16 hours. The RR of a difficult or failed intubation incident occurring in this duration of work range compared to non-airway incidents occurring in this duration of work range was 1.4. Although it is not possible to calculate the absolute risk in this study, one can assume the majority of procedures are performed during normal business hours (0800–1759).
Intubation attempts
Analysis of the narratives have shown that a third of the reports described multiple intubation attempts and some of these required a significant amount of time until intubation was finally successful. The incidents in this study were reported in a time frame from 2009 to 2016. In 2011, the Fourth National Audit Project (NAP4) was published in the United Kingdom 14 and the results were released, which resulted in the development of the new Difficult Airway Society’s difficult intubation guidelines in 2014. 8 The use of a cognitive aid in airway management, the Vortex, was introduced in 2016 12 and has gained significant popularity. These guidelines and cognitive aids aim to take human factors into account, including techniques and guidance to avoid fixation error and encourage no more than three intubation attempts. Nevertheless, our data show that from 2009 to 2016, there had been a large number of incidents where anaesthetists repeated intubation attempts several times. In only a minority of the patients, successful oxygenation via facemask or SAD was used as an opportunity to wake up the patient.
The largest number of intubation attempts described in this cohort was eight attempts or more in two separate incidents. One event was an after-hours intubation as part of the preparation for transporting an unwell neonate. Direct intubation was attempted by different operators until successful. The other patient suffered from a significant congenital underlying mid-facial abnormality and was scheduled to undergo elective surgery. The procedure was abandoned after multiple failed intubation attempts and the patient was woken up breathing spontaneously through an SAD.
Equipment issues
A total of 31 incidents (18%) reported equipment problems. Six reports mentioned endotracheal tube cuff failure requiring reintubation. The laryngoscope light was not functioning or insufficient in four incidents, causing a delay in securing a definitive airway. Monitoring issues, including dysfunctional capnography, were mentioned in five incidents, resulting in additional intubation attempts. Several incidents reported advanced airway equipment, including VLs, failing during rescue intubations, with five incidents reporting light or system failures, whereas the setup time for emergent bronchoscopes was ‘taking too long' or ‘too difficult' in two of the incidents. Urgently required equipment was unavailable in 13% of incidents. Specifically, fibreoptic bronchoscopes were missing from the difficult intubation trolley in four incidents. The lack of equipment was usually noticed late during the procedure when airway manoeuvres had already commenced. These incidents emphasise the importance of thorough preoperative checking and planning of the availability of potentially needed airway equipment.
Airway rescue devices
The most successful rescue device across the incidents reported, after other techniques at oxygenation had failed, was facemask ventilation (71, 41.8%). Once successful ventilation was obtained, only 20 anaesthetists elected to wake their patient as part of their failed initial airway management. Two of these incidents described patients undergoing emergency after hours procedures when initial intubation attempts by an anaesthetic trainee failed. One of these patients was a known difficult airway, but previous records were reported as not available. Both times the senior anaesthetist who was called back for rescue decided against an awake FOI (AFOI) and re-induced anaesthesia in the patient and attempted a similar intubation technique as that used initially. This resulted in significant difficulties in securing the airway, including multiple attempts with different airway devices until intubation was finally successful. As a result, one patient required ICU admission until airway swelling subsided.
It is of note that both patients were at high risk of aspiration due to their underlying pathology and both had predictors of potentially being a difficult intubation.
SADs have been advocated as a rescue device for failed intubation in national and international difficult airway guidelines and cognitive aids.8–12 The literature on their success and failure rates is sparse, but first-time insertion success rates have been described as being as high as 90%–100%, depending on the device used.27–29 In the 170 difficult and failed incidents reported, an SAD had been part of airway management in 60 incidents (35.3%) of which 35 (20.6%) were successful in restoring ventilation. However, in 21 incidents (12.4%), rescue using an SAD failed. In a significant proportion of these failures, attempts at providing oxygenation via facemask ventilation also proved difficult or unsuccessful. Ventilation via the ILMA was attempted in 15 incidents (8.8%) and ventilation was successful in ten of these incidents (5.9%). A successful blind intubation technique through the ILMA was described in only one incident. There were two reports of failed blind intubation attempts, including one using an ILMA. In both of these incidents the reporters had multiple failed attempts at rescuing the patient’s airway using a range of different equipment and techniques. One of these two patients was woken up after significant desaturation and the other patient required a rescue FONA. In contrast, bronchoscopy-guided intubations using an SAD during difficult airway management were successful in ten incidents, using a range of different SADs and the support of intubating catheters in some. One reporter mentioned difficulties in lifting the elevator bar of the ILMA with the flexible bronchoscope, which was solved by advancing the endotracheal tube first.
The use of the blind intubation technique might compromise an already tenuous airway, and the widespread availability of fibreoptic scopes might make this technique redundant in the future.
The analysis of the data exemplifies that attempts at securing the airway using a range of different techniques and devices yielded varying success rates. This supports observations from large studies examining airway management, describing that when one airway technique is difficult or fails, the risk of other techniques being difficult or failing is considerably increased. 27
Video Laryngoscopes
A wide variety of VLs offer alternatives to direct laryngoscopy and have been the topic of multiple publications and research. 30 Some hospitals in Europe have moved to ‘universal videolaryngoscopy’ in recent years, thereby replacing their standard direct laryngoscopes with VLs for all intubations. 31 , 32 Although this is not the case in most institutions across Australia and New Zealand, the use of VLs seems to be increasing, and their immediate availability is now considered a standard of care in most hospitals. Even though a large number of reports in this study (99, 58.2%) described the use of at least one type of VL during their airway management, a significant percentage did not describe the use of a VL as part of their airway strategy at all. There is evidence that videolaryngoscopy improves the view and intubation success when direct laryngoscopy fails while reducing intubation difficulties and trauma. 30 However, in this cohort the use of a VL was not successful in nearly a third of the attempts (31 of 99). Difficulties visualising airway structures, equipment failures and the unsuccessful use of introducer adjuncts were commonly described in these incidents. Often the VL was used as a rescue device after multiple other upper airway attempts had failed. The data were collected from 2009 until 2016, some at a time where the routine use of VLs was still in its developing stages. The authors speculate that inexperience and lack of immediate availability contributed to this high number of late and consequently failed VL attempts.
Fibreoptic intubation
In the past, AFOI was regarded by many as the gold standard technique for difficult airway management. 2 Since the introduction of VLs, the use of awake tracheal intubation techniques seems to have declined. The NAP4 audit also described multiple events where an AFOI was not performed when indicated. 14 Failure rates from 1.5% to as high as 11%33–36 have been reported in various studies. Of all the incidents in the current report, 47 (27.6%) involved the use of a fibreoptic technique and a third of all the fibreoptic intubation attempts failed. The majority of the fibreoptic intubations were performed unplanned and asleep during unexpected difficult airway management. During difficult intubation and airway rescue, the highest success rates were reported when a laryngeal mask functioned as a conduit for the fibreoptic scope. This is in line with the current literature, reporting success rates of up to 98% for this technique. 37 However, some reporters encountered difficulties during this technique, including cuff damage and inability to advance the endotracheal tube into the trachea, requiring multiple attempts until successfully securing the airway. The reporters decided to perform an elective FOI only in a small number of incidents, of which five failed. Four of these five were performed with the patient anaesthetised, of which one required rescue by an ear, nose and throat surgeon, another two had to be woken up and one required rescue intubation using direct laryngoscopy.
There was only one failure of an elective AFOI, when the patient regurgitated and vomited during unsuccessful attempts and had to be rescued using an RSI with a VL technique. It appears there may be a reluctance to perform AFOI. It is possible that limited exposure to AFOI during anaesthesia training and the increased availability and comfort in the use of VL (and the resulting unfamiliarity with the technique) may explain its reduced use. Similar trends had been reported in Europe, which has led to the recent development of guidelines for awake tracheal intubation. 35 , 36 These findings suggest the need for more frequent practical education sessions in the use of both asleep and awake FOI techniques.
Remote areas
The lack of advanced airway equipment, including VL, especially in remote areas, was mentioned in several incidents. A current ANZCA recommendation is that all anaesthetising locations should have immediate access to adequate emergency airway equipment wherever airways are managed. 38 A flexible bronchoscope including a portable light source is recommended to be available within five minutes. 38 As many difficult airways are unpredictable, it is the authors’ opinion that VL equally should be immediately available in remote locations. A lack of essential basic airway equipment, including stylets and bougies, was mentioned when airway management was performed out of the theatre as, for example, in the emergency department, gastroenterology or radiology unit and neonatal ICU.
Outcomes of difficult and failed intubation
The reports indicate the majority of incidents resulted in no harm (37.6%) or only minor harm (44.7%). However, 12.4% of incidents resulted in moderate harm, 3.5% in severe harm, and there were three deaths.
Hypoxia ≤85% and cardiopulmonary resuscitation (CPR):
A total of 40 patients (23.5%) suffered from hypoxia below 85% during their airway incident. Of these, four required CPR and one died. More than half of the patients who suffered from hypoxia below 85% had no or only minor sequelae at the time of reporting. Four patients developed cardiac arrhythmias requiring CPR. Two of these patients presented already in extremis due to multiple injuries, sepsis and multi-organ failure. The other two were paediatric patients, one with underlying congenital cardiac disease. Severe hypoxia was frequently present in patients who died in the NAP4 audit 14 and various patient outcomes ranging from severe harm and death to full recovery without sequelae were reported. The NAP4 audit reassuringly estimates death from airway management as 1 in 180,000. 14
Death
Although three patients died, only one death was likely due to failed airway management. The patient presented for an after-hours emergency procedure. An RSI was performed but failed and the patient regurgitated and aspirated. The anaesthetist reporting this incident had been on prolonged duty and considered this to be a contributing factor to the incident. Aspiration remains a feared occurrence in anaesthetic practice and has just recently again been reported as being associated with significant harm and death. 16 ANZCA has also recently released a professional document highlighting the importance of fatigue management. 39
Limitations
WebAIRS is a voluntary de-identified incident reporting system. Data are collected via tick-boxes and narrative text boxes from entries by anaesthetists across Australia and New Zealand. The tick-box entries allow for rapid data extrapolation and the narratives allow the assessors to understand the event properly and in more detail. Although the combination is expected to provide a complete picture of an incident, the entry fields in webAIRS are not mandatory and it is possible some information is not entered. Similar to other incident reporting systems, it is difficult to collect accurate denominator data representing the Australian and New Zealand surgical population. Denominator data were not collected by webAIRS and the numerator data were submitted voluntarily, which precluded absolute risk calculations. The webAIRS database was used as a source of surrogate denominator data. A limitation of this approach is that the denominator data in the webAIRS database may not necessarily be comparable with the wider surgical population.
Conclusions
Despite advances and significant developments in airway management strategies, difficult and failed intubation incidents still occur. The data indicate that not all incidents are predictable, nor are all of them preventable. Difficult and failed airway management can occur in any patient age and with any ASA PS. Patients with a BMI >30 kg/m2 and those undergoing emergency procedures appear to have a higher risk of difficult or failed intubation incidents. Human factors, lack of planning, lack of checking equipment, fatigue, poor communication and teamwork issues continue to be contributing factors. Although increased BMI and the emergent nature of specific procedures remain unmodifiable in the acute setting, attention to preoperative assessment, improving ease of access to past medical and anaesthetic history and the adoption and maintenance of equipment standards are all within the purview of anaesthetists and their organisations to improve planning, preparation and, fundamentally, the execution of difficult airway management.
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MC is Medical Director of the Australian and New Zealand Tripartite Data Committee (ANZTADC). YE is a committee member of ANZTADC. No conflicting interests exist for the remaining authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The webAIRS database is jointly funded by the ANZCA, the Australian Society of Anaesthetists and the New Zealand Society of Anaesthetists. The present study received no additional funding.