
Abstract
A survey sent to fellows of the Australian and New Zealand College of Anaesthetists (ANZCA) aimed to document issues affecting gender equity in the anaesthesia workplace. A response rate of 38% was achieved, with women representing a greater proportion of respondents (64.2%). On average women worked fewer hours than men and spent a larger percentage of time in public practice; however, satisfaction rates were similar between genders. There was a gender pay gap which could not be explained by the number of hours worked or years since achieving fellowship. The rates of bullying and harassment were high among all genders and have not changed in 20 years since the first gender equity survey by Strange Khursandi in 1998. Women perceived that they were more likely to be discriminated against particularly in the presence of other sources of discrimination, and highlighted the importance of the need for diversity and inclusion in anaesthetic workplaces. Furthermore, women reported higher rates of caregiving and unpaid domestic responsibilities, confirming that anaesthetists are not immune to the factors affecting broader society despite our professional status. The overall effect was summarised by half of female respondents reporting that they felt their gender was a barrier to a career in anaesthesia. While unable to be included in statistics due to low numbers, non-binary gendered anaesthetists responded and must be included in all future work. The inequities documented here are evidence that ANZCA’s gender equity subcommittee must continue promoting and implementing policies in workplaces across Australia and New Zealand.
Keywords
Introduction
In 1998, a Queensland anaesthetist published results of a landmark survey ‘Unpacking the burden: gender issues in anaesthesia’ 1 to ask whether gender played a role in an anaesthetist’s career and experiences. She reported hostile attitudes to women working part time and in private practice, and disproportionate career disruption for female anaesthetists due to childbearing, at a time when women constituted 17% of the Australian and New Zealand anaesthesia workforce.
A repeat survey a decade later was presented as a formal project to the Australian and New Zealand College of Anaesthetists (ANZCA) (Smith and Ashes, unpublished data supplied to authors), and published as a brief letter to the British Journal of Anaesthesia; 2 it showed that gender inequity persisted across a range of domains. Since that time, progress has been made as the ANZCA fellowship approaches numerical parity. In 2021, 34% of ANZCA fellows who partook in the fellowship survey were women, 62% were men, 1% were another gender and 3% preferred not to say. 3 There are examples of improved female representation in committee membership and research. 3
However, there are ongoing studies investigating gender inequity in anaesthesia: women are under-represented in departmental leadership and committee chair positions, 4 and are over-represented in uptake of parental leave, 5 and in the experience of bullying, harassment and discrimination.4 –6 While the biennial ANZCA Fellowship surveys capture valuable data about gender representation, there has been no in-depth work since that of Strange Khursandi and Smith and Ashes, exploring contemporary expressions of gender inequity within the Australian and New Zealand anaesthesia workforce.1,2
In 2022, we administered a survey that sought to document longitudinal changes since previous surveys, and cover emerging domains of interest in gender equity. This survey is in alignment with the ANZCA gender equity subcommittee (GESC) position statement and action plan. 7 It was motivated by ANZCA’s belief in the ethical, social and economic benefits of gender equity to its workforce and community. 8
Our study aimed to describe if gender inequity is manifest within current anaesthesia workplaces in Australia and New Zealand, and to identify areas within the anaesthesia workforce where gender equity work might need to be done. The updated survey questions addressed not only whether there are differences in the number of hours worked, location and remuneration for the work performed, but also in career satisfaction. In previous studies, caring roles and childrearing played a key role in determining differences in male and female anaesthetic careers, so we also aimed to document these broader societal issues around relationship status and caring for dependents which affect Australian and New Zealand anaesthetists. In the current survey, questions addressed access to part-time work, afterhours commitments and job sharing, strategies which reflect ANZCA’s commitment to creating flexible and empowering workplaces. Mentoring, leadership and other opportunities for career advancement were also investigated to identify where ANZCA policy may continue to drive improvements for gender equity. Documentation of whether a gender pay gap exists in line with other Australasian workplaces was also sought. 9
Methods
Approval was obtained from the Westmead Hospital Human Research Ethics Committee 2021/PID0524. The survey was designed by a group of six anaesthetists who are all members of the ANZCA GESC. The survey consisted of a combination of Likert scale and multiple-choice questions divided into eight sections, with an option for free-text comments at the end of each section. The survey included some directly repeated questions from previous studies, but updated others to reflect current anaesthetic work practices as well as more contemporary gender influences on anaesthetic careers. The full version of the 34 survey questions can be viewed online as Supplement 1. The survey sections were:
Demographics Anaesthetic career Discrimination, harassment and bullying Leadership, mentors and research Income Relationships Dependents and caregiving Concluding question—‘In 2022, do you believe your gender is a barrier in the pursuit of a career in anaesthesia?’
We sent the survey to a random sample of 1225 ANZCA fellows in line with the ANZCA clinical trials network (CTN) approach for similar surveys in Australia and New Zealand. 10 All 6400 ANZCA fellows were eligible for participation. Members from all genders recorded in the database (male, female, another gender) were included. On the recommendation of the head of the CTN, the survey was sent to 49.5% male, 49.5% female and 1% other gendered fellows per their registration in the database. The selected fellows were invited to participate by email, and non-identifiable data were collected and securely stored using the REDCap platform. Participation in the survey was voluntary, with consent implied when participants chose to click on and complete the study link. No question in the survey was compulsory. The survey remained active for a period of 4 weeks, with reminder emails sent by ANZCA at 2 and 3 weeks.
Statistical analysis was performed using Stata 17.0 (StataCorp LLC, College Station, TX, USA). Likert scales were compared using ordinal logistic regression unless the assumption of proportional odds did not hold, or difference of proportions was deemed to be easier to interpret. Interval regression was used to compare ordinal variables that could be interpreted as continuous variables (e.g. hours worked); the Wilcoxon rank sum test was used to compare ordinal variables that could not. Fisher’s exact test was used to compare non-ordinal categorical variables. The Z-test for proportions was used to compare dichotomous variables. P values and differences are reported with a P value of less than 0.05 considered statistically significant.
Results
Demographics
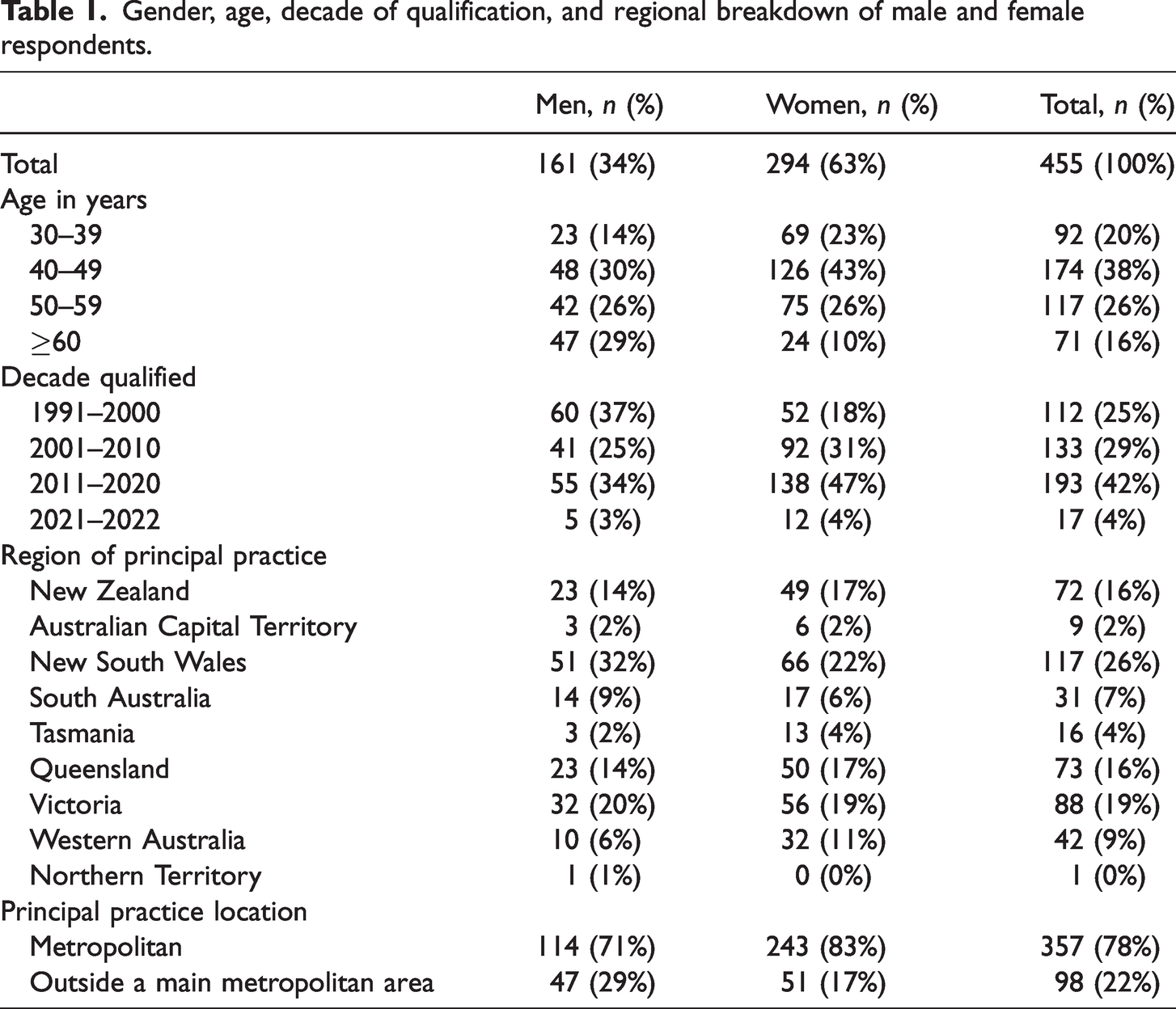
We received 470 responses, giving a 38% response rate. Demographics of our survey participants are summarised in Table 1 and were compared with data from the 2021 ANZCA Fellowship Survey. There were some differences between male and female respondents in our survey, notably in age distribution and decade since qualification; however, these did not reach statistical significance, and the survey population is similar to the ANZCA fellowship in all domains except gender. Twelve respondents chose not to disclose their gender, so were unable to be included in further analysis. Despite the survey being disseminated to 611 men (49.9%), 611 women (49.9%) and three non-binary or other (0.2%) ANZCA fellows, the actual respondents were 161 men (35.2%), 294 women (64.2%) and three fellows identifying as non-binary or other (0.6%). The non-binary or other group was too numerically small for statistical evaluation, so this group was excluded from further quantitative analysis. As such, 455 responses were submitted for final quantitative analysis.
Gender, age, decade of qualification, and regional breakdown of male and female respondents.
Anaesthetic career
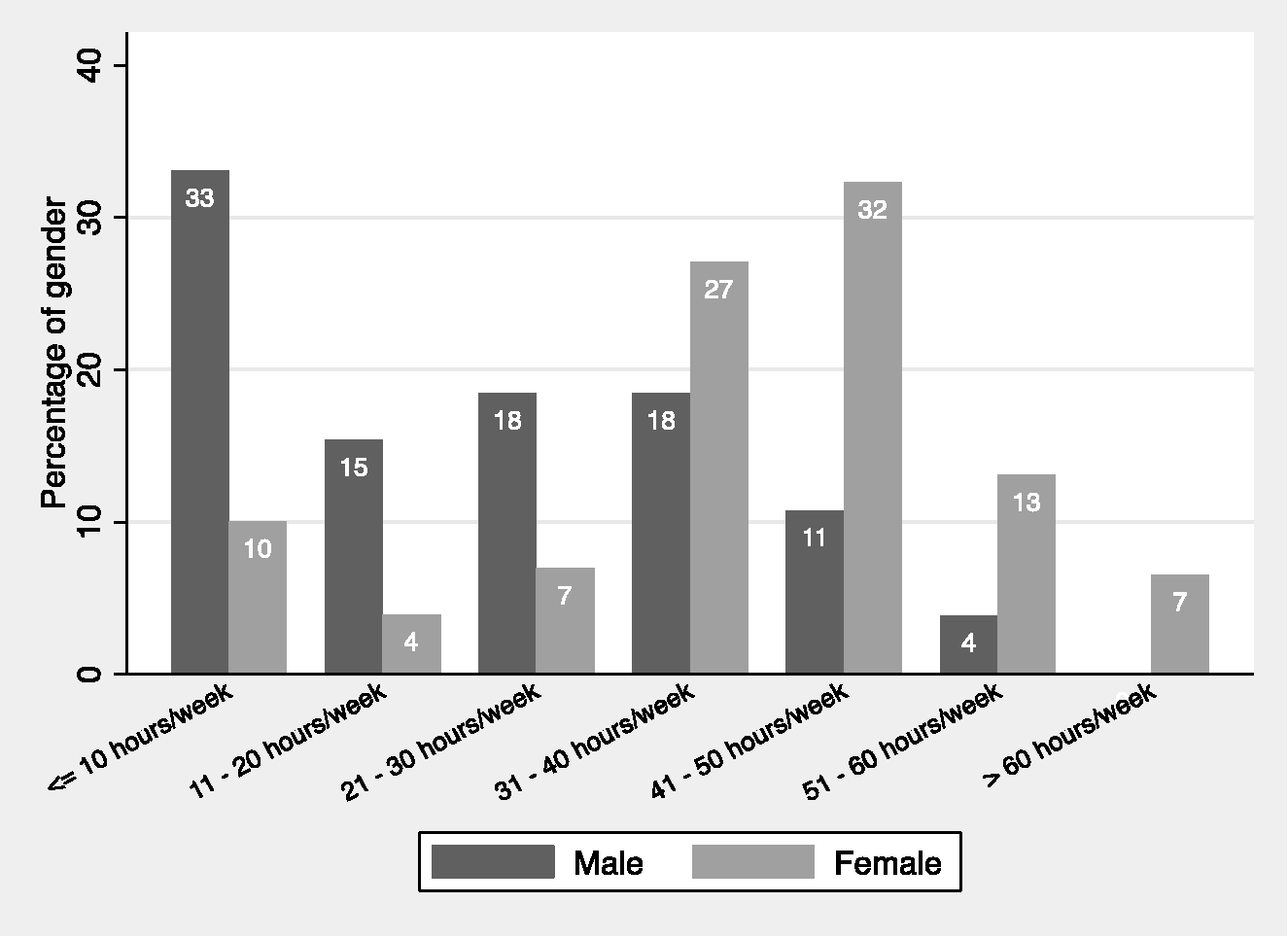
Work patterns differed between men and women respondents. The peak of male respondents (43% of total male respondents) fell into the 41–50 hour per week bracket while the peak for female respondents (41% of total female respondents) fell into the 31–40 hour per week bracket. Using interval regression women on average worked 4 hours less per week than men (95% confidence intervals (CI) 2 to 7, P < 0.001). Women worked a larger percentage of their week in public practice (Wilcoxon rank sum P = 0.02) than men, and correspondingly a lower percentage in private practice (Wilcoxon rank sum P < 0.001). There was no significant difference in hours worked in non-clinical and clinical support work (Wilcoxon rank sum P = 0.79) or unpaid non-clinical work (Wilcoxon rank sum P = 0.73) between the genders.
There was no significant difference in work satisfaction levels between men and women, with less than 6% of both genders reporting they had too little or far too little overall work. There was no difference in genders regarding their access to work in a subspeciality or area of special interest. Five percent of women reported being ‘very dissatisfied’ with their afterhours commitments compared to less than 1% of men, but the overall distributions of satisfaction with afterhours commitments were not statistically significant (ordinal odds ratio (OR) 0.93 (95% CI 0.66 to 1.31); P = 0.676). A greater proportion of women reported being ‘very satisfied’ or ‘satisfied’ with part-time work opportunities than men (logistic OR 1.62 (95% CI 1.09 to 2.42); P = 0.017). Women were more likely than men to be dissatisfied or very dissatisfied with leadership opportunities in clinical or administrative domains (logistic OR 0.61 (95% CI 0.42 to 0.91); P = 0.014).
Discrimination, harassment and bullying
We asked respondents to comment on discrimination in the workplace perceived as related to their gender, ethnicity, relationship status, age, sexual orientation and religion. We did not provide a definition of discrimination for respondents, instead accepting that any perception by the individual of discrimination is valid. The summary of results is given in Table 2, where analysis has been performed for male and female respondents in each domain. Women reported higher rates of perceived discrimination in all domains, but this was only statistically significant for gender (P < 0.001), relationship status (P < 0.001) and age (P = 0.012). Furthermore, 108 of 242 women (45%) (95% CI 38% to 51%) agreed or strongly agreed that they were discriminated against due to their pregnancy status.
Answers to the question ‘During my anaesthetic career I have experienced discrimination due to my gender, ethnicity, relationship status, age, sexual orientation or religion’ using logistic regression where agree and strongly agree is compared with neutral, disagree and strongly disagree.
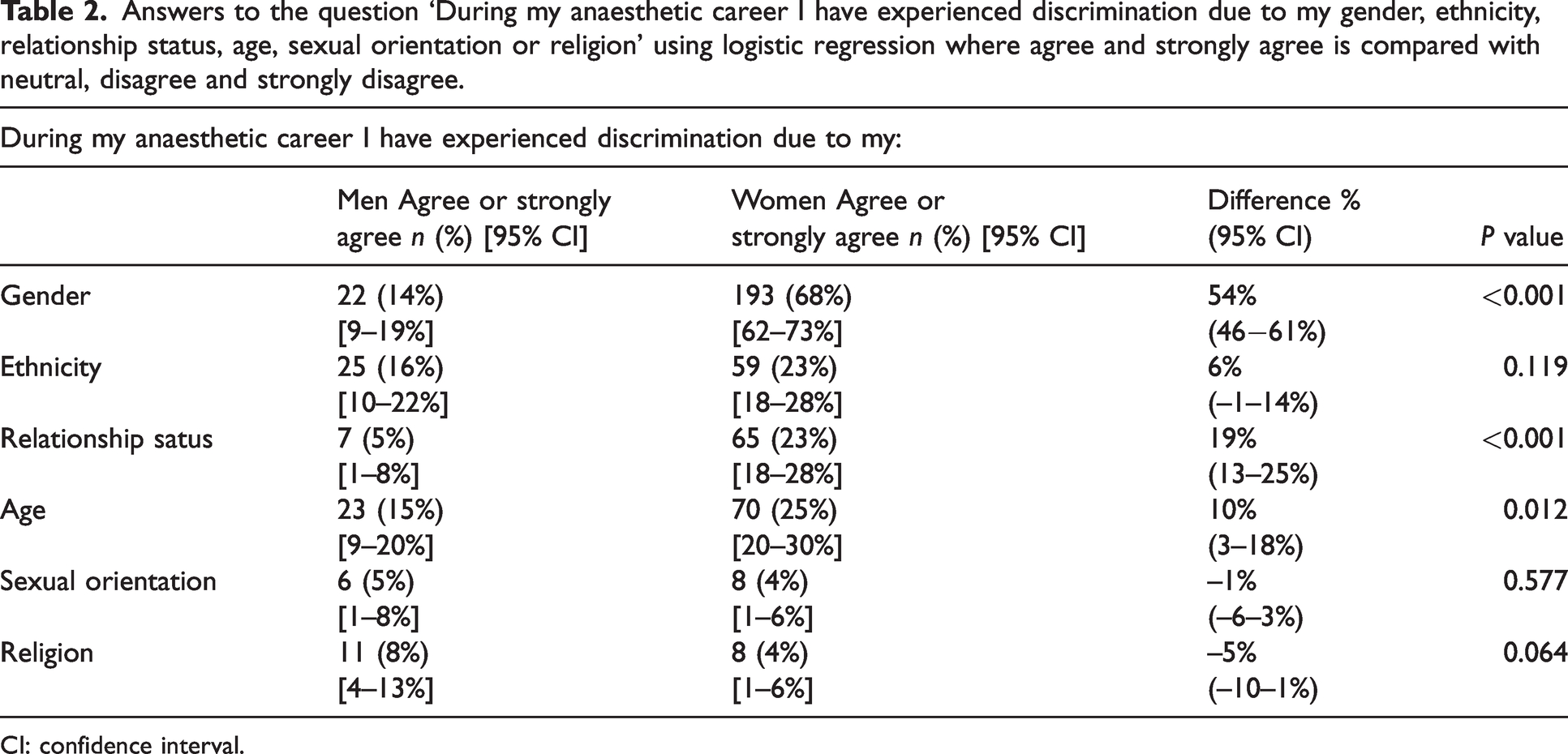
CI: confidence interval.
Table 3 lists the results for rates of sexual harassment, bullying and perceived difficulties obtaining a consultant position according to gender. Twenty-one percent of women respondents reported experiencing sexual harassment which was 11% (95% CI 4% to 17%) higher than men (P = 0.0045). Reports of bullying were more common among female anaesthetists (P = 0.0074), but were relatively frequent within both genders (48% of women; 34% of men). Women responded at higher frequency that the experience of obtaining a consultant position was more difficult due to their gender (36% of women; 3% of men) (P < 0.001).
Reported rates of sexual harassment, bullying and perceived difficulties obtaining a consultant position according to the gender of the respondent.
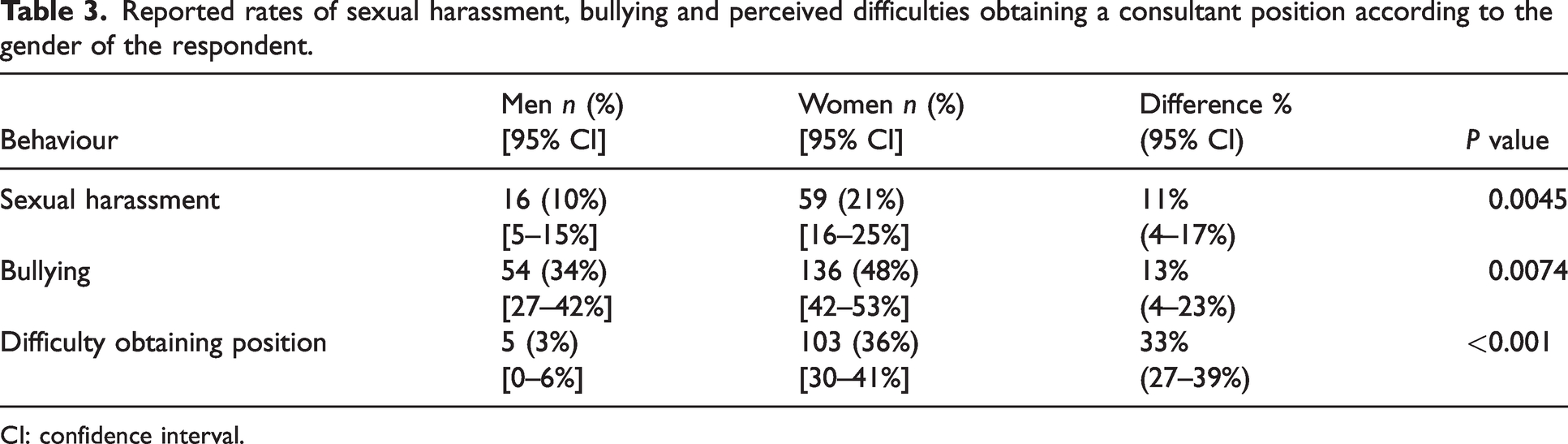
CI: confidence interval.
Mentors, research and leadership
When examining the role of mentors in the careers of respondents, minimal differences were observed based on gender. However, a lower percentage of women than men reported ease in finding meaningful research opportunities (ordinal OR 0.51, 95% CI 0.36 to 0.73).
Female respondents observed that decision-making roles or roles of influence within public departments were unequally distributed between genders (ordinal OR 0.43, 95% CI 0.29 to 0.65), whereas most men perceived no gender-based differences. Fifty-six men (35%) and 127 women (45%) stated they have obtained or are enrolled in a postgraduate qualification. This represents a 10% difference between genders (95% CI 0% to 19%, P = 0.0515).
Income
Figure 1 displays respondents’ reported salaries according to gender. In the Australian private healthcare system, individual practitioners provide services as contractors and bill patients or their health fund directly. There is no regulation that governs the rate of pay, but guidelines are provided by Medicare, the private health insurers and the Australian Medical Association (AMA). The mode of billing was recorded to assess whether the gender pay gap reflected a difference in billing practices, but there was no significant difference in mode of billing in private practice between genders (Fisher’s exact P = 0.379). Using interval regression, women earn $118,000 (95% CI $75,000 to $161,000, P < 0.001) per annum less than men. A difference of $67,000 (95% CI $28,000 to $107,000, P = 0.001) still existed when hours worked, age, region and decade of ANZCA fellowship qualification were added to the model. Adding percentage of public work to the model reduced the sample size from 411 to 368; however, a difference of $60,000 (95% CI $26,000 to $93,000, P < 0.001) persisted.
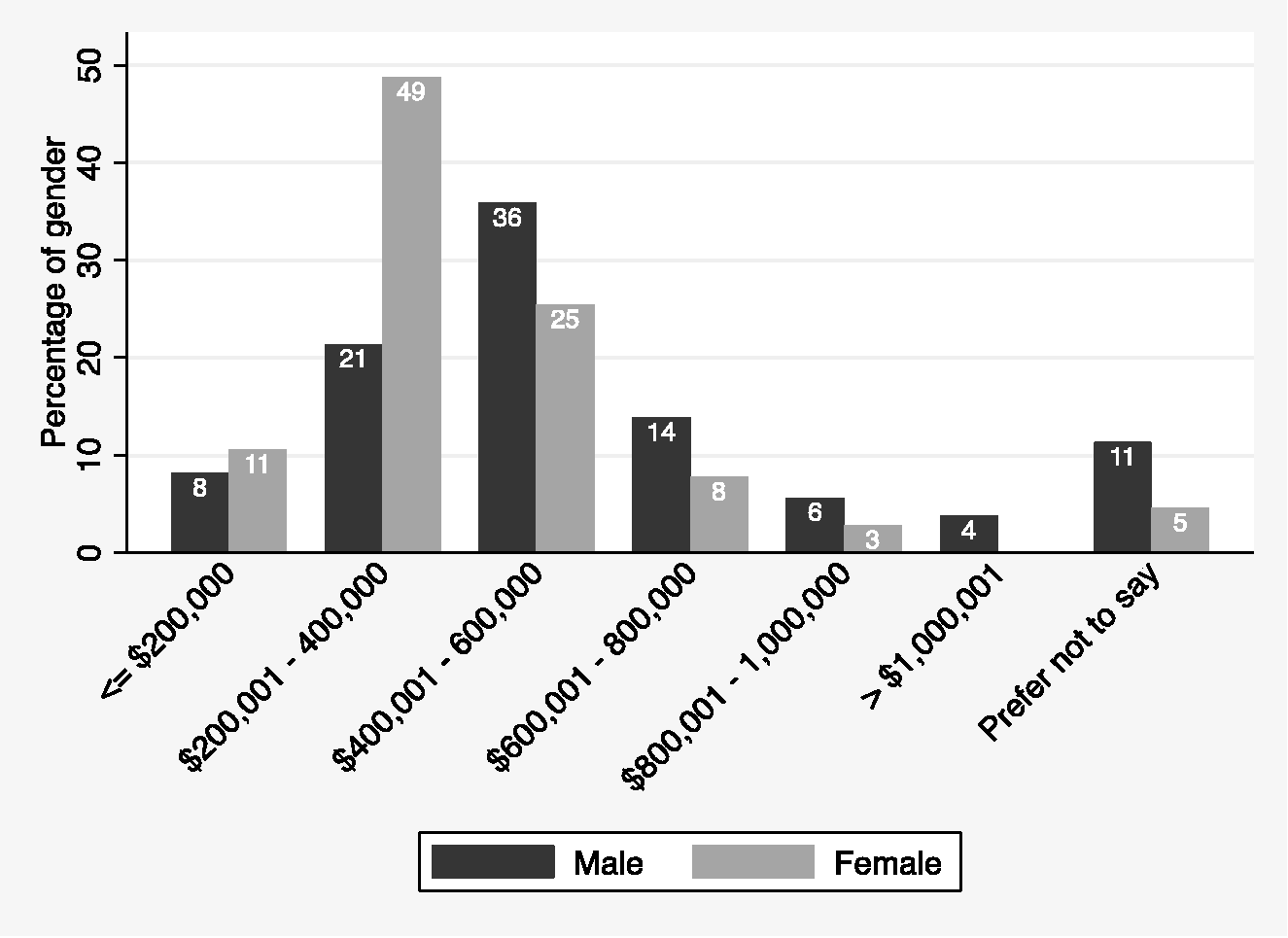
Answers to the question ‘What are your annual billings/salary (pre-tax) from anaesthesia-related work?’ as answered according to the gender of the respondent.
Relationships
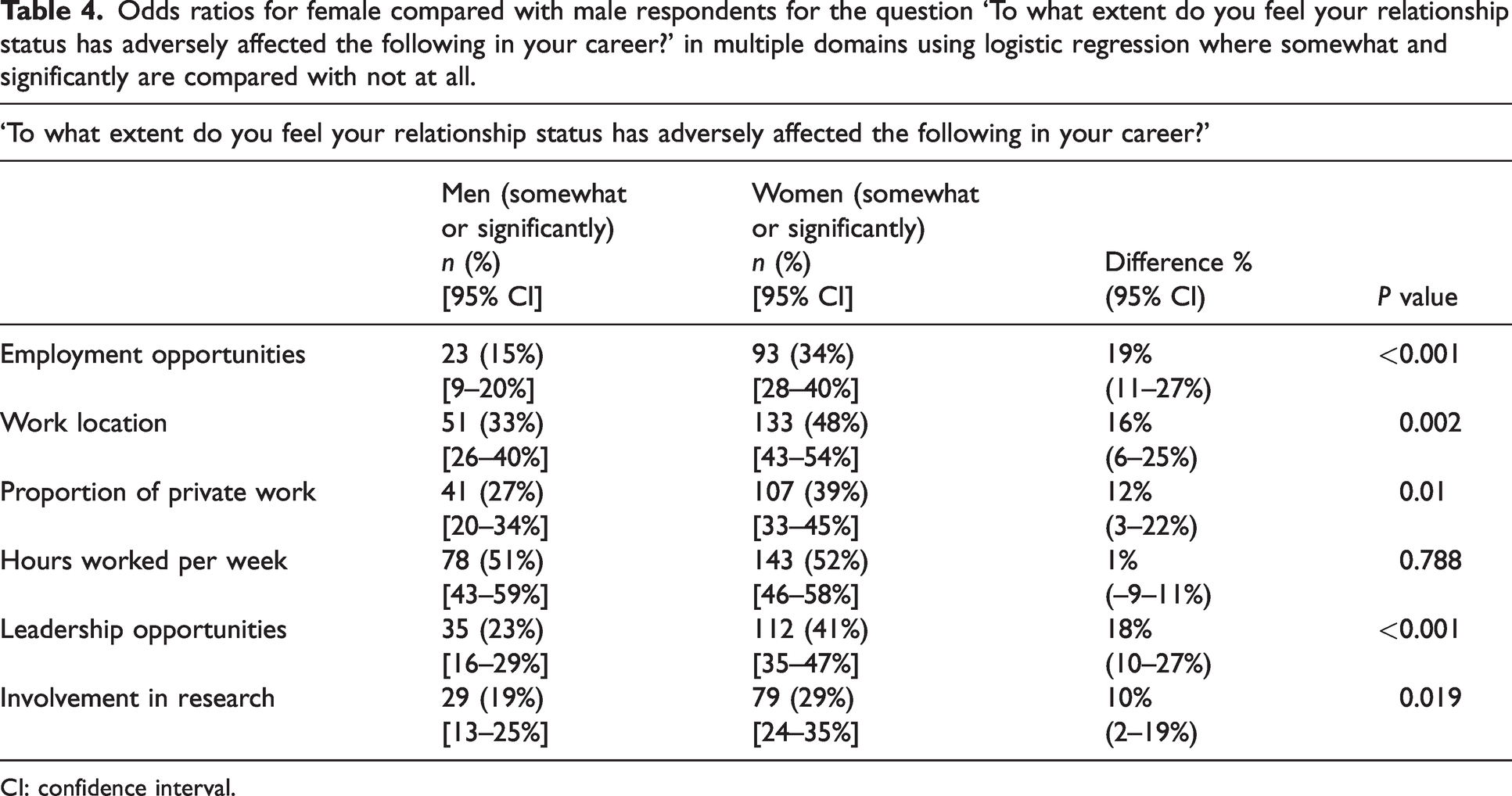
There was no difference in the relationship status of respondents by gender (Fisher’s exact P = 0.496). Figure 2 shows working hours of partners by gender. Using interval regression women’s partners worked 19 hours (95% CI 15 to 22, P < 0.001) more per week in paid employment than men’s partners. Women reported that their domestic partners contributed less to domestic responsibilities than those of men (Wilcoxon rank sum P < 0.001). Women also reported a greater adverse impact of their relationship status on employment opportunities, work location and leadership opportunities compared with men (Table 4).
Answers to the question ‘How many hours per week does your partner work in paid employment?’ according to the gender of the respondent.
Odds ratios for female compared with male respondents for the question ‘To what extent do you feel your relationship status has adversely affected the following in your career?’ in multiple domains using logistic regression where somewhat and significantly are compared with not at all.
CI: confidence interval.
Dependents and caregiving
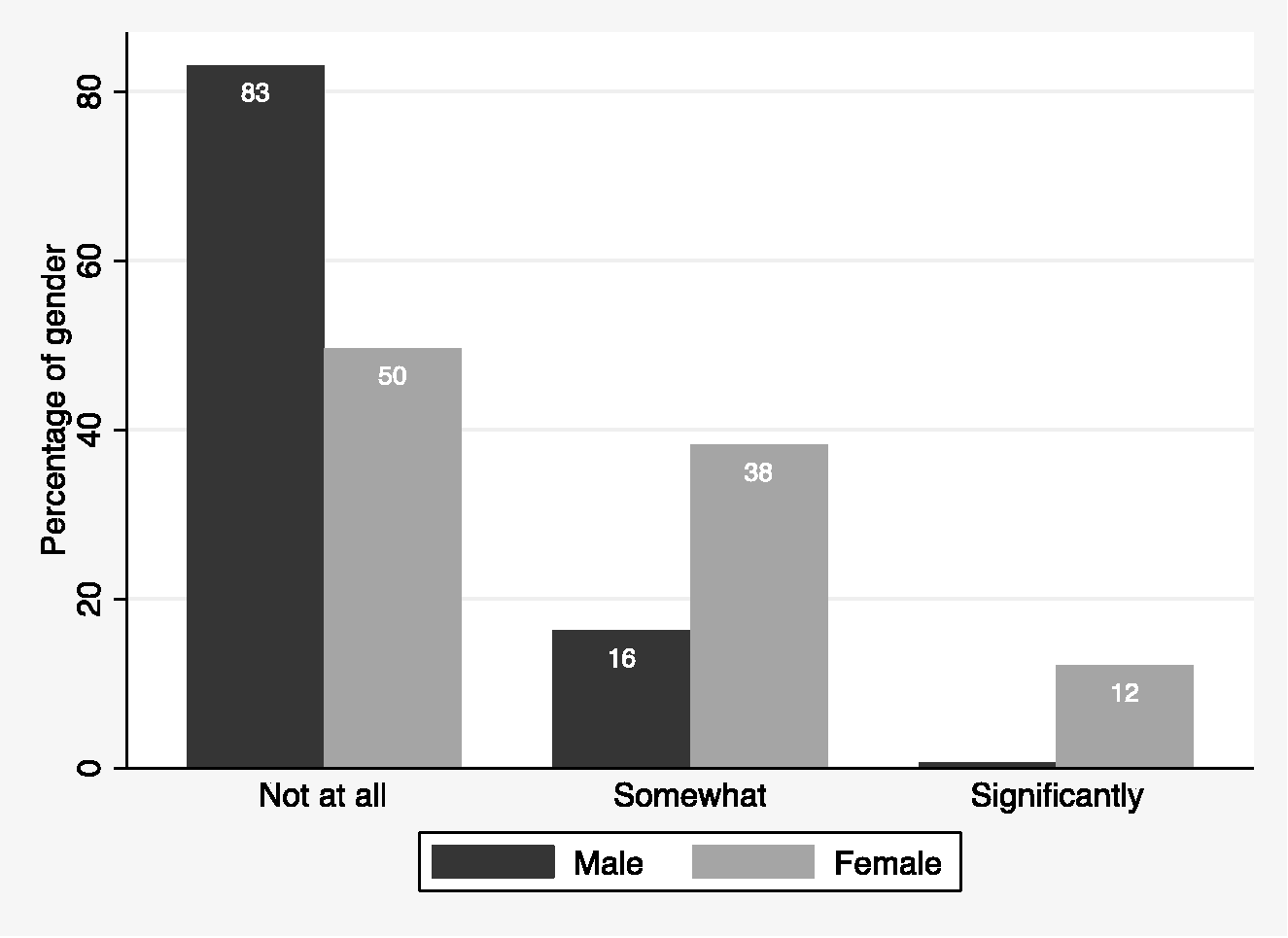
In respondents, 51% of men (78/154, 95% CI 43% to 59%) and 67% of women (185/278, 95% CI 61% to 72%) stated that they were a caregiver for dependents. The difference was 16% with 95% CI 6% to 26% (P = 0.0012). Figure 3 shows that 52% of women compared with 10% of men reported being the primary caregiver for any dependents in their household; 44% of men compared with 8% of women were not the primary caregiver and 46% and 39% of women reported equal responsibilities for caregiving in their household. Seventy-five percent of women reported that their anaesthesia career had somewhat or significantly affected the size or timing of their family while 60% of men reported no effect (Figure 4).
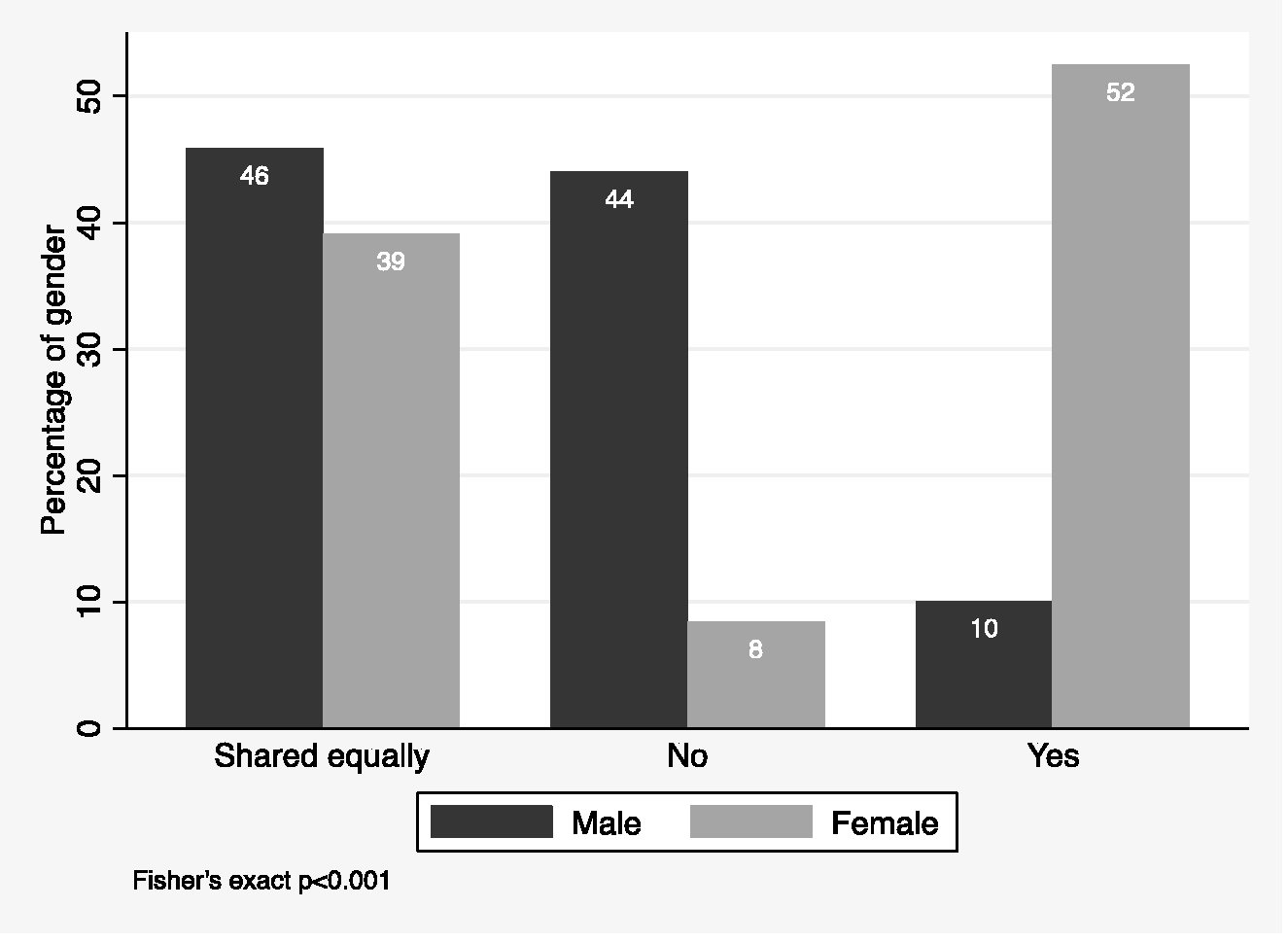
Answers to the question ‘If you have children or dependents, are you the primary caregiver in your household?’ according to the gender of the respondent.
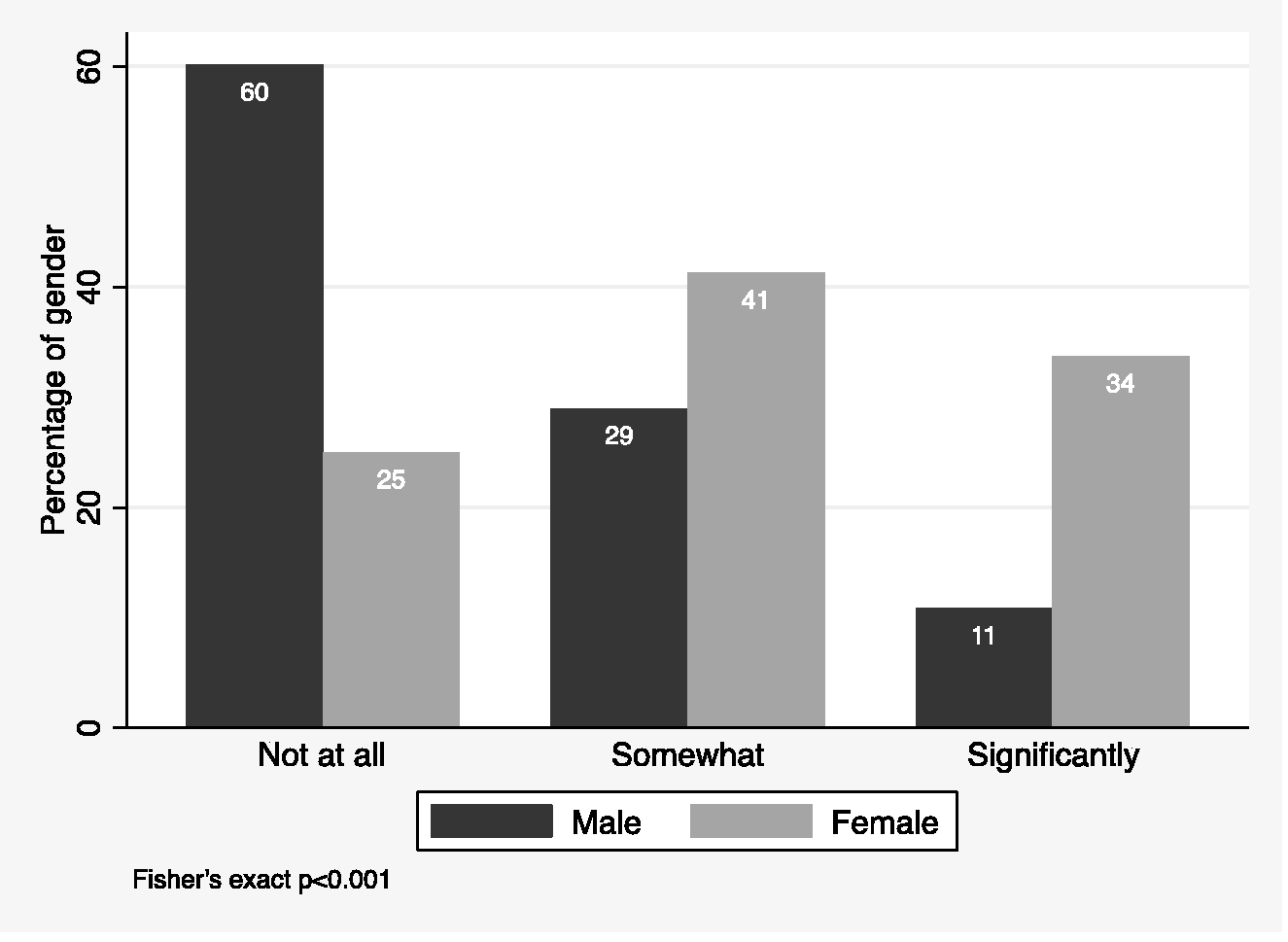
Responses to the question ‘Has your anaesthesia career negatively affected the size or timing of your family?’ according to the gender of the respondent.
Women were more likely to report that having children or dependents had adversely affected their career in terms of employment opportunities, proportion of private work, hours worked, leadership opportunities and involvement in research compared with men (Table 5).
Odds ratios for female compared with male respondents for the question ‘To what extent do you feel having children or dependents has adversely affected the following in your career?’.
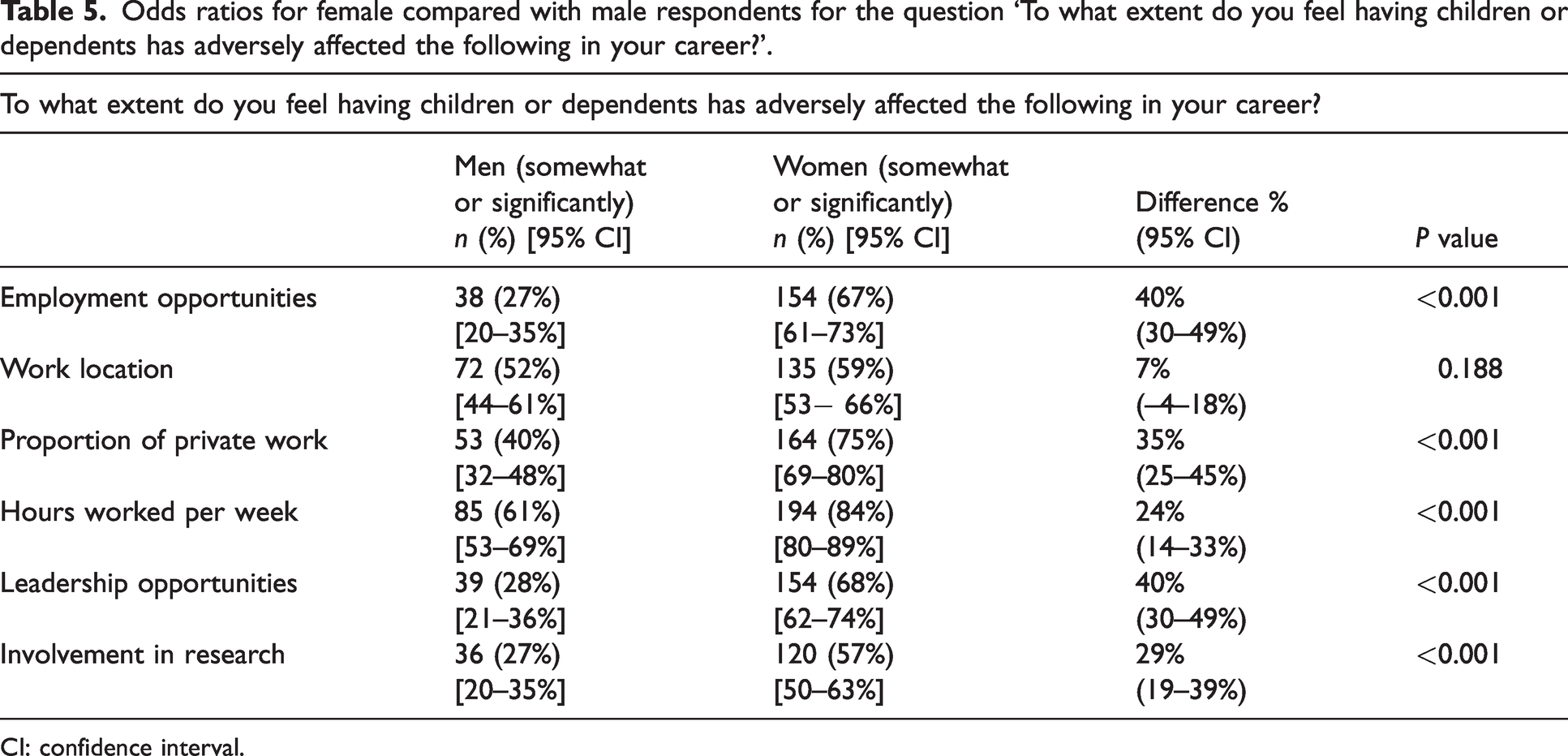
CI: confidence interval.
In 2022, do you believe your gender is a barrier in the pursuit of a career in anaesthesia?
Figure 5 shows the distribution of responses for the final question asked in the 2022 survey. Of the respondents, more women reported that their gender was a barrier to a career in anaesthesia, with an ordinal odds ratio of 5.20 (95% CI 3.22 to 8.41, P < 0.001).
Responses to the final survey question ‘In 2022, do you believe your gender is a barrier in the pursuit of a career in anaesthesia?’ according to the gender of the respondent.
Discussion
Anaesthetists across Australia and New Zealand work in diverse environments, but all are governed by some form of anti-discrimination law.11,12 Despite this, our survey confirms that many respondents still perceive and experience differences based on their gender. Progress towards numerical parity over the past 20 years has not in itself resolved the issues reported in the surveys conducted by Strange Khursandi and Smith and Ashes.1,2 Our results identify areas of gender inequity within anaesthetic workplaces, and have also identified broader societal issues particularly around relationships and caregiving. While individual workplaces, or even larger anaesthetic societies, cannot change deeply entrenched societal beliefs and attitudes, or influence an individual home or family unit, there is no doubt that caring responsibilities and the level of domestic support available at home have a direct impact on a person’s capacity to contribute at work. It is therefore important to document and understand the broad range of factors contributing to gendered effects on anaesthetic careers and thereby identify and implement effective strategies to reach a position of gender equity.
Our survey received a better response rate than other ANZCA surveys, 3 with a notably skewed population of more female responses. While there are many possible explanations for this, one such possibility is that this reflects a societal expectation that equity and inclusion are ‘women’s work’. This phenomenon has been well described including in the Harvard Business Review. 13 Responder bias may exist in our results. The authors had proposed that the CTN distribute the survey according to the total ANZCA fellowship gender breakdown of 34% women, 62% men, 1% another gender and 3% preferred not to say. The CTN recommended against this, instead 49.5% men, 49.5% women and 1% other were selected. Future surveys may reduce responder bias by distributing according to the gender breakdown of fellows in the database. It is essential that other genders are brought into the discussion as no balance can be achieved without all players in a system being engaged. Several of our questions asked whether respondents believed differences exist based on gender (e.g. in leadership representation and career trajectory) and interestingly for each one the female respondents believed a difference existed while male respondents did not. We propose that these conflicting views indicate that many male anaesthetists will not perceive gender imbalance as an issue requiring correction. Further exploration is required to confirm this proposition, but we would argue that this idea underlines one of the many challenges facing gender equity, in which members of one group in the workplace fail to see the challenges faced by another, and therefore do not consider their contribution to positive improvement. We hope the results of this survey highlight to anaesthetists of all genders that there is ongoing work to be done to achieve gender equity.
The serious consequences of gender bias for women are put into sharp focus with the observation that there was a tenfold higher rate of perceived difficulty in obtaining a consultant position for female anaesthetists compared with men. Although the reasons underlying this perceived discrimination were not interrogated in this study, relevant research suggests it is likely to be due to a combination of male culture, unequal standards, insufficient support and devaluation of the contribution of women as well as various degrees of hostility, often in association with gender stereotyping. 14 The observation that gender has the strongest correlation with the perception of workplace discrimination for female anaesthetists confirms the findings from previous Australian and New Zealand data.1,2 It also confirms that our local setting reflects international observations with respect to the significant gender bias in anaesthesiology and many other medical specialities.15,16
Multiple recent studies from around the world confirm the under-representation of female anaesthetists in formal leadership roles.5,6 Unsurprisingly, this trend was reflected in our survey responses from female respondents. Gender research suggests this is due to both explicit and implicit barriers that continue to hinder women’s progress to high-level leadership. 14 All directors and senior managers have responsibility to ensure that women are represented meaningfully at all levels of the hierarchy. It also highlights the importance of ensuring concerted efforts to prevent women from being appointed to tokenistic roles in which influence is qualified and limited, and male leaders remain the gatekeepers of participation. The observation that the female respondents were more likely to be enrolled in or hold a higher qualification than their male counterparts support findings from previous research that women are arguably held to a higher standard before they are considered of equal eligibility for sought-after roles.14,17 Combining a need to seek higher levels of education than male colleagues with more time in unpaid caregiving roles, women have less time available for seeking paid working opportunities.
The difference in female representation in anaesthetic research is supported by international data. 18 Although it might be suggested that anyone can offer to undertake research, the challenges faced by a novice researcher lead to an inference that success in leading a project will be heavily reliant on the support and mentorship available to such a researcher, and unconscious biases may affect opportunities and networking. Furthermore, time for research may be limited for female anaesthetists who perform more hours of unpaid caregiving and non-clinical work.
A gender pay gap was identified in this survey, acknowledging limitations (small sample size, gender differences in our respondents, potential responder bias, and the untested nature of the regression model used), the gender pay gap is consistent with other publications. Of note, an observational study of New Zealand senior medical specialists found an hourly wage gap of 12.5%, when women were compared with men of the same speciality, age and working hours, despite working within the public system on a collective employment agreement. 19 The data used in this study were based on completed 2013 census results and government tax records. A more recent survey sent to 28,000 American Society of Anesthesiologists (ASA) members with a response rate of 7.2% found a wage gap of 8.3–8.9% among US anaesthesiologists. The gender pay gap identified in our study is also not unique to anaesthesia, and is consistent with the ubiquitous pay gap identified in many workplaces—the Australian government’s Workplace Gender Equality Agency (WGEA) confirmed in 2022 that Australia’s national gender pay gap is 14.1%, 9 despite gender discrimination being illegal for many years in both Australia and New Zealand.
There are many potential explanations for this pay gap in anaesthesia, and it is likely to be complex in nature, given that in Australia and New Zealand, anaesthetic income can be drawn from multiple sources and is highly varied. In Australasian public hospitals, specialists are subject to national (NZ) or state-based (Australia) employment contracts, which may vary between facilities but would offer little difference based on a practitioner’s gender. Meanwhile the private healthcare system allows individual practitioners to bill patients or their health funds at whatever rate they determine appropriate for their services. There was no statistically significant difference in mode of billing between men and women identified in this survey to explain the pay gap. One limitation of this finding is that we asked respondents to report their ‘most frequent mode of billing’ if applicable to them. As such, some respondents may most frequently have a no-gap or known-gap practice but less frequently do highly lucrative, higher gap work which would not have been recognised by this question. Selection to work in the private health system is based primarily on surgical selection of anaesthetists and networking among anaesthetists. One explanation for the pay gap is that male anaesthetists are more likely to work on lucrative surgical lists; however, this theory is outside the scope of this survey and requires further investigation. Of note, working hours in the private system are determined by surgical bookings, and can involve long hours which may not be amenable to those with caregiving responsibilities. In our survey, the hours per week worked in the private system were lower for women; however, satisfaction with the availability of private work was not different between genders. This may imply that women self-select to work less in a system with demanding hours because the pay benefit does not compensate for the need to fulfil other commitments. The unregulated nature of the private healthcare system is also subject to many unconscious biases that could not be explored by our survey but warrant further investigation.
Another major contributory factor to the gender pay gap is likely to be caregiving. Women were more likely to identify as having dependents according to our data, and far more likely than men to identify as the primary caregiver of their dependents. This is in keeping with trends associated with professional careers observed in society at large, as documented by the Australian government’s WGEA in their 2022 gender equality scorecard. 20 It has also been recognised in the Harvard Business Review as occurring throughout many workplaces. 13 While the effect documented in our survey reflects an overall societal trend with broad socioeconomic drivers, anaesthetic workplaces should strive to optimise equity given the investment made when training anaesthetists of all genders. It was not surprising that women took on average 10 months more parental leave than men. This is a trend also seen in ANZCA trainee data, with men contributing to only 1% of the applications for interrupted training for parental leave in 2018 and 2019. 3 This leads to two issues. First, the ANZCA gender equity action plan 2018 − 2022 endorses all genders to engage in key societal roles such as caregiving and breadwinning, identifying this as a gender inequity, and specifically aiming to increase the adoption of carer roles among male trainees, specialist international medical graduates (SIMGs) and fellows. 7 Second, the career progression of women is significantly impacted by the ‘parenthood factor’. Parenthood has a greater negative impact on women’s medical careers than men’s, including advancement in training, number of hours worked and career support experiences. As such, pregnancy status remains a common source of perceived workplace discrimination. 21 Although well documented previously, this study aligns with other recent research that demonstrates there is still much unconscious bias and practical disadvantage experienced by women of child-bearing age in the medical profession. 22 Research has shown that pregnancy is associated with increased workplace stress, and efforts directed at preserving professional legitimacy can increase the harm experienced. 23 The detrimental impact of pregnancy discrimination is exacerbated by the fact that it usually occurs at a crucial stage of career development. ANZCA has tried to address discrimination by developing an unconscious bias toolkit that interview panels can use to reduce sources of bias when interviewing candidates. Further work could include formalising minority quotas for trainee positions, more structured scoring systems for hiring fellows and more flexible parental leave allowances. The solutions remain complex due to the nature of anaesthesia workplaces being within public healthcare facilities or private hospitals over which ANZCA has little control.
Despite the requirements of an anaesthesia career, many anaesthetists seek to have families. Fertility and complications of pregnancy in physicians is currently topical.23 –25 Our results show that women were more than four times more likely to report their anaesthetic career having a negative impact on the size or timing of their family (OR 4.43). A recent survey of Australian and New Zealand doctors found that structural biases and a strong paternalistic culture resulted in many women delaying childbearing. 24 Training often occurs during prime reproductive years, and women doctors are more likely to experience fertility issues, pregnancy loss and complications of pregnancy compared with the general population. This likely reflects the physical demands of anaesthesia, including manual handling and the extended working hours. In a survey of US surgeons, women were more likely to use artificial reproductive technology, experience major pregnancy complications, and have unplanned caesarean sections than male surgeons’ non-surgical partners. Forty-two percent of their female respondents had experienced a miscarriage, reported as over twice the rate of the general population aged 30–40 years. 26 After experiencing a pregnancy loss, 75% of these women returned immediately to work, without any leave. 25 This highlights the need for ANZCA, supervisors of training, and employers to support employees wishing to start or add to their family, through addressing issues such as safer work conditions, availability of reduced hours and on-call requirements, and considering barriers to advancing in training such as the single centralised location for viva examination at each exam sitting, which may be inaccessible in later gestation. The aim of achieving true equity in workplaces may mean that employees are treated differently in some circumstances in order to provide equality of opportunity.
Intersectionality refers to the increased risk of workplace disadvantage if an anaesthetist identifies with more than one minority status attribute. This study demonstrates the importance of intersectionality for the anaesthetic profession because it showed that non-gender attributes such as relationship status, ethnicity, sexual orientation and age could further exacerbate the baseline negative impact of female gender. This finding is congruent with recent research from the US which found that intersectionality for under-represented minorities continued to result in lower faculty academic rank in anaesthesiology, fewer partnership opportunities in private practice, and disparate research funding. 27 Diversity and inclusion are vital to ensure workplaces reflect the communities they serve, thereby minimising healthcare disparity and improving patient-centred care. 28
While so far the gender equity differences have been highlighted, there were positive effects reported in this survey. Satisfaction with overall working hours was high for both male and female respondents. We are looking forward to publishing qualitative data which may allow a deeper level of understanding into true satisfaction levels despite the recorded differences in working hours and pay. In contrast to research indicating lower rates of mentorship for women, 6 this study showed that mentor relationships were established equally between the genders. Mentoring has proved benefits for both mentors and mentees, as well as the anaesthetic departments with active mentoring programmes. 29 ANZCA strongly encourages mentoring and has many resources on its website to facilitate those seeking to establish a programme. It is also a welcome finding that the rate of sexual harassment reported in the survey by female anaesthetists is lower than previously reported; however, it is obviously a metric in which zero tolerance must be the aim. 1 Of concern, the response by 21% of women that they had experienced sexual harassment was much higher than the 3% reported in the equivalent survey of fellows of the College of Intensive Care Medicine. 30 This may be explained by slightly different definitions of the conduct at issue, which makes direct comparisons difficult. Of note, legislation already exists at a state level and is about to be introduced at a federal level in Australia that will result in legal consequences for employers who fail to protect employees from sexual harassment in the workplace. 11 New Zealand’s Employment Relations Act 2000 also holds employers liable for sexual harassment complaint handling within workplaces. 12
Unfortunately, rates of bullying reported were disturbingly high, and this should be considered a call to action at both a college and department level. Significantly, the question specified events that occurred since qualifying as a specialist anaesthetist—this means the years of particular vulnerability during unaccredited and accredited medical training (specifically covered in other surveys) are excluded from our data. The rates reported also compare unfavourably with other critical care specialities. 30 These findings suggest that pathways for dealing with unprofessional behaviours need to be strengthened.
Limitations
There are many limitations to the data presented and the nature of survey data. Of note, non-binary and other gender data were collected but the number of results were insufficient for statistical analysis. Concerns were also raised that the low frequency meant the inclusion of these respondents could be potentially identifiable. While we were disappointed by this limitation, we are passionate that future surveys will continue to expand the focus on gender diversity.
The response rate to this survey was satisfactory for publication standards 31 and similar or higher than other ANZCA CTN-distributed surveys.10,32 –34 The voluntary nature of survey research and the named focus of research into gender equity may have also resulted in significant responder bias. Those who have experienced gender inequity were more likely to complete the survey. Alternatively, those who believe that no inequities exist or who are invested in the current system may have also been more likely to respond. Please note that the respondents were matched to the 2021 ANZCA fellow population for all demographic categories except gender, for which the number of female respondents was higher than the ANZCA population. This creates the potential for random bias particularly for male respondents. We will recommend that future surveys are distributed to a sample representative of the gender breakdown for ANZCA fellows. The time to complete the survey or technical access may have also been a limiting factor for the response rate.
There is a large potential for self-reporter bias, particularly when respondents were asked to estimate hours worked and their income. Despite this, the differences found in this study have been correlated with data from similar populations overseas and are consistent with the historical surveys of ANZCA fellows.
Many of the statistical analyses were exploratory, may have been underpowered, and include multiple simultaneous comparisons so should be interpreted with caution. We used a P value of less than 0.05. We encourage readers to consider that a high number of tests were applied, but also that each question represents a new dataset.
Differences with previous surveys
While we were inspired by the works of Strange Khursandi and Smith and Ashes,1,2 there were significant differences with how our survey was designed and distributed. Most importantly, this is the first gender equity survey endorsed and distributed through ANZCA, the governing body for almost all anaesthetists practising in the region. The previous surveys were distributed through the Australian Society of Anaesthetists, which is a voluntary membership body with fewer members. Furthermore, both previous surveys had lower respondent numbers and sample sizes. As such, we hope that the data presented here more closely represent the experiences of anaesthetists across the wide variety of workplaces in Australia and New Zealand. ANZCA have committed to repeating this work on a regular basis to maintain longitudinal tracking of gender equity.
Conclusions
The results of this survey reflect the current opinions and perceptions of a large group of anaesthetists, giving an updated focus on potential areas of gender inequality in our profession which require further investigation and can be actively addressed moving forward. Gender is perceived by female respondents to be a significant barrier in achieving multiple professional goals relevant to a career in anaesthesia in 2022. However, the differences we have documented in the professional experience of fellows of different genders is only likely to be meaningfully improved if it is widely acknowledged by all members of the anaesthesia community. It is also imperative to create a culture of inclusion such that fellows who identify as non-binary or other gender feel safe and supported. We have identified societal factors influencing anaesthetic careers, as well as areas for policy improvements at both ANZCA and local departmental levels, and hope that widespread dissemination and discussion of our results will raise awareness and promote action addressing the gender issues still present in anaesthesia. Further resources on addressing gender inequity include the unconscious bias toolkit and library resources on the ANZCA gender equity website. 35
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X231212210 - Supplemental material for Does gender still matter in the pursuit of a career in anaesthesia?
Supplemental material, sj-pdf-1-aic-10.1177_0310057X231212210 for Does gender still matter in the pursuit of a career in anaesthesia? by Claire H Stewart, Jane Carter, Natalie Purcell, Maryanne Balkin, Julia Birch, Greta C Pearce, Timothy Makar in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to thank Dr Karen Byth from the University of Sydney and Westmead Hospital who helped with the early statistical analysis. They must also acknowledge the guidance provided by Dr Lindy Roberts from ANZCA in preparing this manuscript—many thanks for her generosity.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.