
Abstract
Gender inequity persists within the anaesthetic workforce, despite approaching numerical parity in Australia and New Zealand. There is evidence, from anaesthesia and the wider health workforce, that domestic gender norms regarding parental responsibilities contribute to this. The creation of ‘family-friendly’ workplaces may be useful in driving change, a concept reflected in the gender equity action plan developed by the Australian and New Zealand College of Anaesthetists. This study aimed to explore the extent to which a family-friendly culture exists within anaesthesia training in New Zealand, from the perspective of leaders in anaesthesia departments. An electronic survey composed of quantitative and qualitative questions was emailed to all supervisors of training, rotational supervisors and departmental directors at Australian and New Zealand College of Anaesthetists accredited training hospitals in New Zealand. Twenty-eight of the 71 eligible participants responded (response rate 39%). The majority (61%) agreed with the statement ‘our department has a “family friendly” approach to anaesthesia trainees’; however, there was a discrepancy between views about how departments should be and how they actually are. Several barriers contributing to this discrepancy were identified, including workforce logistics, governance, departmental structures and attitudes. Uncertainty in responses regarding aspects of working hours, parental leave and the use of domestic sick leave reflect gaps in understanding, with scope for further enquiry and education. To redress gender bias seriously through the development of family-friendly policies and practices requires supportive governance and logistics, along with some cultural change.
Introduction
In November 2017 the Australian and New Zealand College of Anaesthetists (ANZCA) established a gender equity working group to ‘promote the importance of equal representation of women and men across our fellowship’, recognising the ‘ethical, social and economic benefits’ of gender equity to its workforce and community. 1 This occurred at a time when 45% of ANZCA trainees, 32% of ANZCA Fellows and 25% of Faculty of Pain Medicine (FPM) Fellows were women, with women under-represented in departmental leadership positions and considerably over-represented in the uptake of parental and carer leave. 2 More recently ANZCA has reported that the number of women who are supervisors of training has increased and that the gender disparity within ANZCA’s leadership and committees is ‘representative of the gender ratio in current fellowship numbers’, 3 suggesting that there has been improvement. ANZCA’s commitment to gender equity is laudable because it provides guidance that may help address the inequity or unfairness with which women are treated across the breadth of medicine. For example, female medical specialists employed by New Zealand’s publicly funded district health boards (DHBs) experience a gender wage gap compared to male counterparts of the same age, specialty and hours worked per week. 4 This is in the context of non-gendered pay scales and is symptomatic of underlying gender bias in promotion and advancement patterns. The gender wage gap in medicine is seen around the world, and is unrelated to seniority, career breaks and part-time work. 5 Other examples of gender inequity exist in academic practice, with women publishing less in anaesthesia journals 6 and having less representation in anaesthetic leadership positions. 7
It could be argued that the anaesthesia workplace merely reflects factors in wider society that contribute to maintaining gender inequity, including cultures and structures that reinforce gender norms related to domestic responsibilities and caregiving. 8 The present norms support a social system that is historically built around patriarchal domination, problematising childbearing and preventing gender equity,9–14 and until we address the ‘caregiver problem’ 11 we cannot meaningfully challenge gender inequity in the medical workforce. This requires an understanding of ‘family-friendly’ practices and policies, those ‘that help to balance and benefit both work and family life’. 15
The ANZCA and FPM gender equity resource kit 16 and gender equity action plan 17 include suggestions that challenge gender-based roles in caregiving, and to be fully implemented would require changes that extend beyond requirements currently embedded in employment law, employment contracts and ANZCA training regulations. The gender equity action plan has defined five focus areas. These include flexible and empowering workplaces (encompassing workplace policies and management practices that enable gender equity in part-time work, primary and secondary parental leave and other flexible work practices) and the identification of areas where substantial gender-based disadvantage exists, in addition to opportunities to close these gaps. 16 , 17 The extent to which these aspirations are currently enacted within anaesthesia training in New Zealand is unknown, nor are there data about barriers to addressing the ‘caregiver problem’ (one of the equity gaps) in ANZCA accredited training schemes. In a recent editorial ‘A call to action: gender equity in Canadian anesthesiology’, Mottiar and McVicar 18 assert that sustainable change towards gender equity in anaesthesia begins in anaesthesia training, and requires buy-in from department directors.
To obtain data about the attitudes and processes that reflect the culture of family-friendly work practices in anaesthesia training departments, and associated barriers to the implementation of ANZCA’s gender equity action plan, we undertook a survey of all supervisors of training (SOTs), including rotational supervisors, and heads of department (HODs) at ANZCA accredited training hospitals in New Zealand. Our aim was to contribute to the gender equity discussion by describing the current state of ‘family friendliness’ in New Zealand anaesthesia training and to identify gaps for further attention.
Materials and methods
We developed a survey using the online platform SurveyMonkey (SurveyMonkey Inc., San Mateo, CA, USA) entitled ‘Understanding attitudes towards “family friendly” practices in anaesthesia training in New Zealand: a survey of anaesthesia supervisors of training and departmental directors’ (see Supplementary Appendix). The survey was peer reviewed by our departmental research committee, piloted on six members in our department, and prospectively approved by the Victoria University human ethics committee (reference 0000028055). In accordance with New Zealand legislative and ethical requirements the study was reviewed and approved by Wellington Hospital’s Maori Research Advisory Group. Maori engagement, advice and input are health priorities in New Zealand because of legal obligations under the Treaty of Waitangi, with Maori health outcomes far worse than for New Zealanders of European descent. Maori constitute 16.5% of New Zealand’s population 19 but only 3.5% of the medical workforce. 20
A confidential web-linked invitation was emailed to all SOTs, including rotational supervisors, and HODs at ANZCA accredited training hospitals in New Zealand. The email was sent by the New Zealand office of ANZCA at the beginning of December 2019 and a reminder email was sent after three weeks. The survey closed four weeks after the initial email. To ensure anonymity, no internet protocol addresses were recorded and before analysis all survey responses were de-identified by a member of our administrative staff (LK).
The survey (see Supplementary Appendix 1) consisted of a mixture of quantitative questions using either five-point Likert scales or yes/no/not sure answers, and qualitative questions to add depth to these responses. Within the survey, questions were grouped in the following clusters: family-friendly practices (15 questions addressing part-time work, breastfeeding facilities, childcare and mentoring); leave policies (seven questions addressing attitudes towards, and management of, parental leave and subsequent return to work, and two questions addressing the use of sick leave to care for sick children); working hours (three questions); free-text comments about ideas for improvement and personal experiences, and demographics (seven questions). The questions were developed to gather data that are aligned with the ANZCA and FPM gender equity resource kit 16 and a recent United Nations Children’s Fund (UNICEF) brief on family-friendly policies. 15
Quantitative data are presented as summary tables. A comparison of the importance placed on family-friendly practices with the extent to which these have been implemented was undertaken using Wilcoxon signed-rank tests to compare the Likert scale data using IBM SPSS Statistics version 26.0 (IBM Corporation, Armonk, NY, USA; 2019).
Qualitative data were analysed thematically, drawing on the inductive approach to grounded theory of Corbin and Strauss, 21 and deductive aspects of the ‘framework approach’ 22 and iterative analysis. 23 JCC categorised the free text according to themes that were predetermined and had been used in the grouping of questions in the survey and those that emerged during analysis. The thematic coding was then checked by ALG.
Results
Seventy-one eligible individuals were invited to complete the survey, comprising 54 SOTs (including five rotational supervisors --- referred to collectively as SOTs hereafter) and 17 HODs, and 28 participated (39% response rate). See Table 1 for respondent demographics.
Demographics of survey respondents.
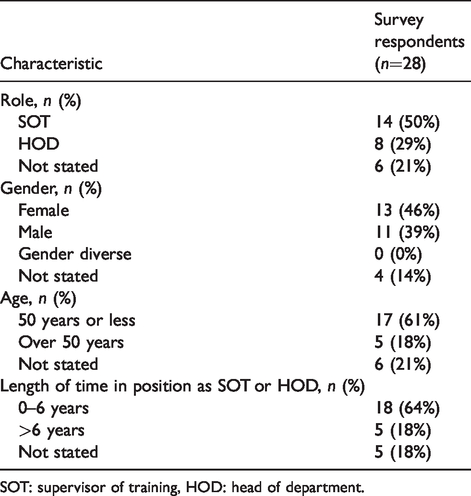
SOT: supervisor of training, HOD: head of department.
Question one asked respondents to agree or disagree with a global statement ‘Our department has a “family friendly” approach to anaesthesia trainees’. All participants responded: 61% agreed or strongly agreed with this statement (four strongly agreed and 13 agreed), three respondents disagreed (11%) and eight neither agreed nor disagreed (29%).
Table 2 summarises the scores from the Likert scales that were used to evaluate the perceived importance and perceived implementation of specific workplace practices. There were statistically significant differences between the importance placed on specific workplace practices and the extent to which they were perceived to have been effectively implemented, except for access to role models/mentoring in which there was no difference.
Summary statistics and comparison of Likert scores for perceived importance of specific workplace practices with how effectively they were perceived to have been implemented.
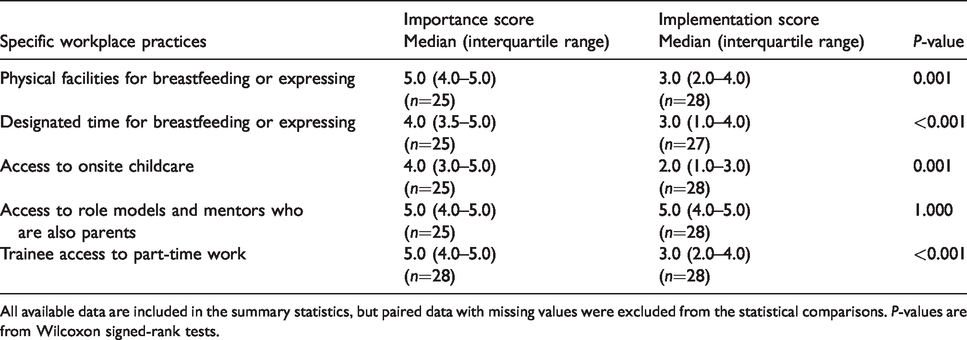
All available data are included in the summary statistics, but paired data with missing values were excluded from the statistical comparisons. P-values are from Wilcoxon signed-rank tests.
Table 3 summarises the responses to the yes/no/not sure questions. Question 24 of the survey (see Supplementary Appendix) asked if participants thought that trainees with children take more sick leave than trainees without children, and while it could be argued that this is outside the scope of the survey, we have included the responses because they contributed useful free comments about existing attitudes.
Responses to yes/no/not sure questions relating to use of parental leave, re-entry to training, sick leave and length of workday: perceptions of supervisors of training and heads of departments.
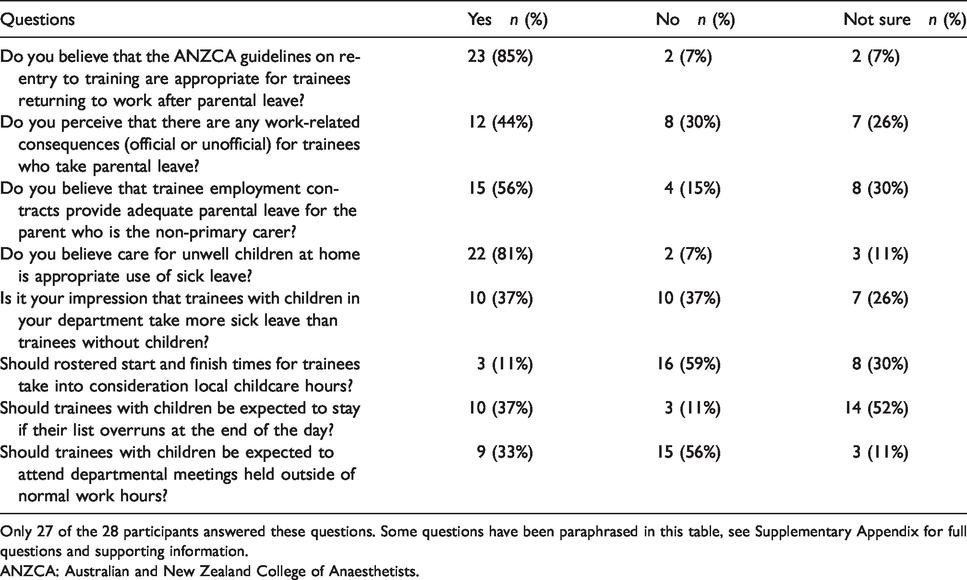
Only 27 of the 28 participants answered these questions. Some questions have been paraphrased in this table, see Supplementary Appendix for full questions and supporting information.
ANZCA: Australian and New Zealand College of Anaesthetists.
Most of the free-text comments fitted within the thematic framework that had been developed during the design of the survey and that had been used to cluster the questions. However, other themes and subthemes emerged from the free-text comments, and emergent themes of fairness, organisational support and governance and personal experience were added to the thematic framework.
Theme 1: Family-friendly practices
Free-text responses to ‘What makes your department “family friendly” (or not)?’ were mostly related to part-time training and job-sharing, in which 11 respondents provided affirmative examples of these and six commented on their absence. Eight commented favourably about the provision of parental leave and five about breastfeeding facilities. In answer to the follow-up question ‘What do you perceive to be the main barriers to implementing “family friendly” practices within anaesthesia training in your department?’, 19 respondents identified the challenges of staffing after-hours rosters with trainees, including workforce limitations, cost and training requirements.
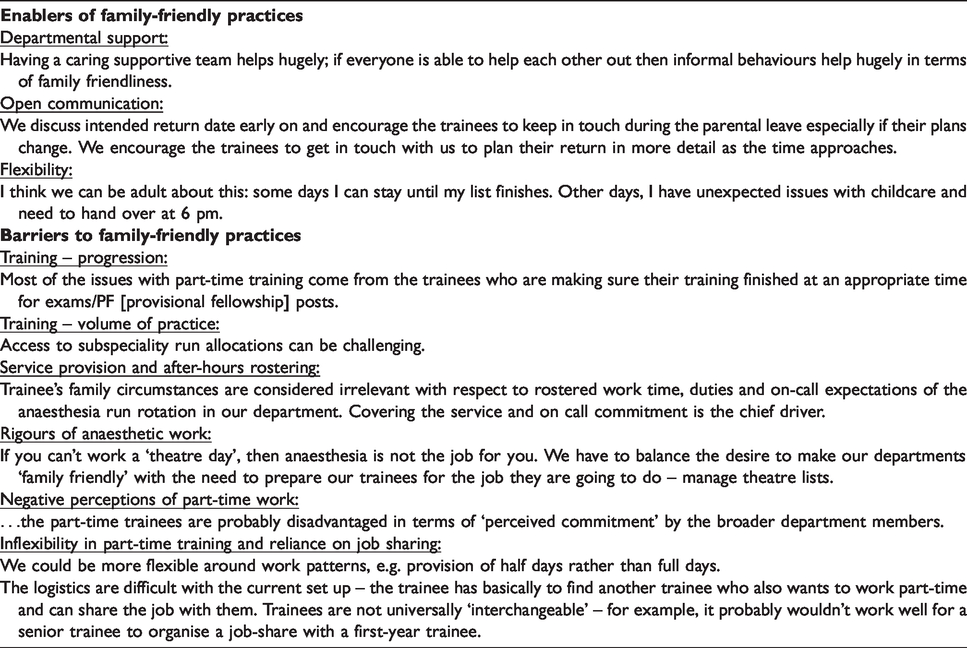
Three dominant subthemes emerged from free-text comments as enablers of family-friendly practices: a culture of departmental support; open communication between trainees and leadership; and flexibility. Departmental support included access to mentors and role models with children. Open communication and flexibility were considered important in both day-to-day running of lists --- including navigating childcare commitments and list overruns, and a broader approach to finding case-by-case solutions for part-time work and parental leave.
Subthemes that recurred as barriers to family-friendly practices, and particularly to the provision of part-time training, were training requirements (including training progression and the ability to meet volume of practice), the logistics of staffing an after-hours service provision roster, workforce limitations (a finite number of registrars able to staff the roster) and the rigours of anaesthetic work. The latter theme emerged in comments reflecting early start times, the unpredictable nature of patient care and difficulties posed by uncertain finishing times that need to be balanced with childcare considerations. Specific to part-time training, perceived barriers included the reliance on job-sharing to accommodate part-time hours and negative perceptions from departmental members. Illustrative quotes for these subthemes are included in Table 4.
Family-friendly practices: subthemes and representative quotes from respondents.
In response to the question ‘Overall, with regards to “family friendly” practices within anaesthesia training, what changes or improvements would you like to see?’, seven participants raised improved support from DHB management, three mentioned greater guidance from ANZCA, five called for better access to part-time work, three for greater flexibility in working patterns and four for more accessible childcare facilities. Two respondents suggested an increase in trainee numbers. Breastfeeding rooms, longer paid parental leave and greater uptake of parental leave by male trainees were each mentioned once.
Theme 2: Parental leave
Subtheme 2.1: Parental leave for the primary caregiver
This theme is largely covered by legislation, and most of the free comments related to how to ‘fill the gap’ of the absent trainee, in the context of fixed financial resources around employment. Although New Zealand legislated parental leave can be shared between parents, comments noted limitations in flexibility and low uptake by male trainees. To improve gender inequality – greater support of men taking parental leave as the primary carer…
Subtheme 2.2: Parental leave for the non-primary caregiver
Comments expressed a range of views regarding the adequacy of parental leave for the non-primary caregiver. I think this [adequacy of leave entitlements] will depend a lot on individual circumstances, e.g. other supports available, first versus subsequent child, health of mother and baby. How much time does one need off? It’s a baby, it doesn’t know who is there.
Subtheme 2.3: Staffing and rostering for parental leave
Participants were asked how they managed staffing and after-hours rostering of trainees within their department to accommodate parental leave. There was a range of answers and some departments employed more than one strategy. Most used locums paid at a higher extra-duty rate to fill gaps on the after-hours roster. Eighteen used other trainees from their own department, eight used trainees from other hospitals and three described specialists picking up unfilled registrar shifts. Some filled the entire position, for example 12 stated that their departments advertised fixed-term positions and four over-appointed (above their establishment) during the annual appointment round based on historical trends. Comments acknowledged the unpredictable nature of parental leave and the limited number of non-training anaesthetic registrars available to fill vacancies. …there isn’t really a pool of suitably qualified, non-training registrars out there without jobs to fill gaps. We are only allowed to advertise when a parent to be gives their notice, and obviously, plans can change. Our management has allowed us to appoint to expected parental leave vacancies when the trainee lets us know they are pregnant and before they need to give official notification of their intentions. We have managed to foster a culture where trainees largely feel able to tell us about their pregnancies early on….
Subtheme 2.4: Return to work after parental leave
Respondents highlighted the dual priorities of providing trainee support, both emotional and educational, as well as ensuring appropriate competency for patient safety in the return to work period. Return from parental leave is a huge personal challenge for the trainee and we need to strive to improve the culture of the profession to be as supportive as possible around this time. Priority is patient safety and wellbeing needs of the anaesthetist. The guideline allows sufficient flexibility to design a re-entry programme that suits the circumstances and maintains oversight of the process by trainees and SOTs throughout. I think this should be able to take into account issues specific to returning from parental leave. More explicit guidance from ANZCA might be helpful regarding the types of arrangements that we should consider for trainees returning from parental leave.
Subtheme 2.5: Consequences for trainees who take parental leave
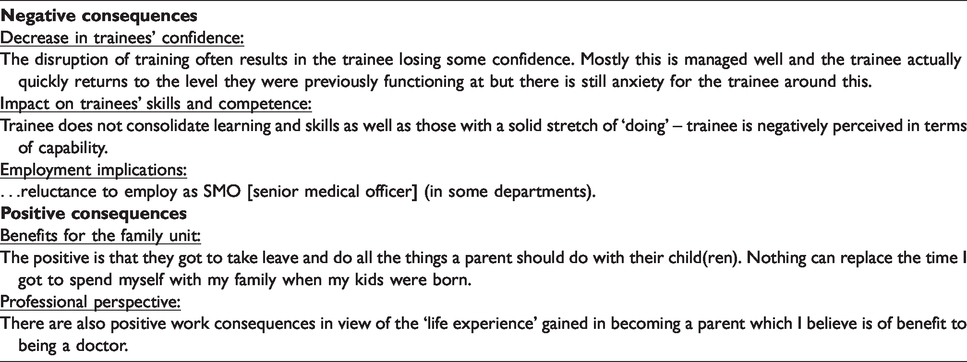
Participants were asked if they perceived any work-related consequences (official or unofficial) for trainees who take parental leave. Of the 12 respondents who perceived there to be consequences, 11 believed them to be negative. Free-text comments allowed expansion, with identified consequences and representative quotes in Table 5.
Consequences for trainees who take parental leave: representative quotes from respondents.
Subtheme 2.6: Domestic sick leave
The two multi-employer collective agreements (MECAs) under which most New Zealand anaesthesia trainees are employed contain provisions for the use of personal sick leave to care for unwell children at home, referred to as ‘domestic leave’ within the Specialist Trainees of New Zealand (SToNZ) MECA (section 26.8)
24
and ‘leave on pay’ within the New Zealand Resident Doctors Association (RDA) MECA (section 21.6).
25
Most participants believed that this is appropriate and there was no obvious agreement with the proposition that trainees who are parents might take more sick leave than trainees without children. The rostering and staffing difficulties of short-notice sick leave were acknowledged, and there was a range of opinions about the locus of responsibility for managing this. This should be encouraged and absorbed by the department. Unwell children with working parents can be a very stressful situation if not supported by the workforce. Endless expectations on the employer to ‘pay’ for an unlimited scope of issues in the name of sick leave are not fair and reasonable. You are employed to work. It’s reasonable for an employer to expect you to do so.
Theme 3: Working hours
Comments highlighted the tension between the practicalities of the job and its hours, and the challenges of childcare that may not align with the operating theatre working day. Staying late is part of the job, and will certainly be required as an SMO. But obviously you can’t expect someone to abandon their child. Trainees need to be encouraged to prepare for this eventuality, but supervisors need to be flexible and acknowledge that it won’t always be possible.
Theme 4: Fairness
Fairness emerged from multiple comments. Respondents were concerned about creating a two-tier system if trainees with children received work-associated leniencies not afforded to those without children (such as not staying to the end of the operating theatre session). In addition, there was concern that family-friendly practices, particularly access to parental leave and part-time training, should not come at a cost or burden to the remaining trainees in the department. Either: NO trainee should be expected to stay if their list overruns at the end of the day or: ALL trainees should be expected to stay. Otherwise this negatively discriminates against childless trainees. We have a small registrar establishment. This means that if someone wanted to work part-time particularly the after-hours roster becomes difficult to manage and the burden on the others would increase.
Theme 5: Organisational support and governance
Participants provided non-specific comments seeking greater structural support from DHB management and from ANZCA, including in the domains of part-time training and return to work after parental leave. It was also noted that there is regional variability in practices. We need to change the way we think in our college and across the board in our NZ [New Zealand] DHBs, with leadership from ANZCA. There are big differences in attitudes in different DHBs in NZ. Some accept and try to help. Others are very non-child friendly with ‘traditional’ attitudes to training.
Theme 6: Personal experience
Examples of personal experience recurred in several open questions, reinforcing the emphasis participants placed on their own experiences in informing their views. This theme was evident in respondents’ appreciation of positive departmental and collegial support that had allowed their careers to progress. …I have spent many years juggling work and family commitments; I understand very well the demands of busy parenthood and busy work. Raising children requires heavy involvement of both parents and hospitals make this challenging. As a new mum to my first child, I was accused by a misogynistic old male consultant (allocated as my mentor by the way) that the SMOs didn’t think I was taking my child care responsibilities seriously enough! I told them when it impacted on my work then they could call me on it but until then it was none of their business. I worked my arse off to prove I was as good and better than my male counterparts and didn’t take a single day off related to childcare issues. It scarred me for life and I’ve been proving myself ever since.
Discussion
This research provides a starting point from which to better understand the attitudes and processes related to family-friendly practices, as perceived by those in leadership positions in anaesthesia training in New Zealand. It adds to the gender equity discussion within anaesthesia by describing predominantly positive attitudes towards family-friendly workplace practices as well as identifying barriers to the implementation of ANZCA’s gender equity action plan and identifying gaps in understanding. The majority of respondents believed that their department has a family-friendly approach to trainees, and responses were overall supportive of practices that enable family-friendly workplaces. This is very reassuring in terms of the ANZCA goal of creating flexible and empowering workplaces and addressing the ‘caregiver problem’. For the purposes of this survey we adopted the UNICEF definition of ‘family-friendly’: those ‘policies that help to balance and benefit both work and family life that typically provide three types of essential resources needed by parents and caregivers of young children: time, finances and services’. 15 Although it is impossible to know the extent to which participants interpreted the questions in the context of that definition, which was included in the survey, the perspectives in the free-text comments provide valuable data.
The data from the Likert scales and associated free-text comments from questions comparing what respondents considered important with what they perceived was actually being delivered within their departments highlight that supportive leadership attitudes, although necessary, are not sufficient to ensure that processes and practices are enacted. Several contributory barriers were identified as potential reasons for this gap between importance and implementation. These include obvious areas of tension; for example, the non-interchangeability of registrars in job-share arrangements and the practical constraints of trainee numbers and rostering. Other barriers include the stigmatisation of part-time training (from trainees and departmental members), and perceived negative consequences of extended training due to parental leave. These stigmatising attitudes, although not the main finding, when held by people in leadership positions do illustrate attitudes that undermine the implementation and uptake of family-friendly policies and reinforce restrictive gender norms. In addition, the presence of logistic barriers such as the high cost and low availability of locums creates the perception of a lack of managerial buy-in, and this may contribute to the observed discrepancy between the ideal and the real. The domain of mentors and role models with children was an exception, being perceived as both important and well implemented in departments. This is encouraging, and may be linked to the themes of personal experience, flexibility and open conversations that emerged from the free-text comments. The low cost of mentoring programmes, and the development of the ANZCA fundamentals of mentoring, may provide some explanation for this perceived implementation success.
An interesting observation was the variability of responses to the ‘yes/no/not sure’ questions as summarised in Table 3. A question addressing the appropriateness of ANZCA re-entry to training guidelines, and another about the appropriateness of using sick leave to care for unwell children, were answered in the affirmative by 85% and 81% of respondents, respectively. This contrasted with the remainder of the responses in which there was considerable variability, with 25%–30% of respondents unsure about the appropriate answer to several of the questions. The heterogeneity and uncertainty in these quantitative answers, and the extensive accompanying free-text comments, suggest that these are either controversial areas or areas where those in positions of influence lack important information. Either way, we propose that these domains are ‘challenge areas’ in family-friendly practices, sitting on the edge of accepted norms. These areas where approximately 30% of respondents did not take a clear position included the initial global statement ‘our department has a “family friendly” approach to anaesthesia trainees’, as well as questions about parental leave for the non-primary carer and consideration of working hours with respect to childcare access, list overruns and out-of-hours departmental meetings. To understand these responses where participants did not take a clear position would require a different data collection approach, such as in-depth interviews. Variability in responses also applied to a question about the consequences of taking parental leave, in which 12 respondents thought there were consequences of taking parental leave, 11 of whom thought there were negative consequences. Some of these negative consequences included temporary reduction in technical competence, whereas others were more disturbing given the statutory obligation for job protection. Another area where findings were disturbing was where five respondents disagreed with, or were unsure about, the use of personal sick leave to care for sick children. This suggests a discrepancy between attitudes and contractual obligations, and possibly an educational gap for those in leadership positions.
Despite majority agreement with the appropriateness of the ANZCA guidelines on re-entry to training, 26 there was considerable diversity in the accompanying qualitative comments. The guidelines are not specific to parental leave; rather they are applicable to any trainee who has taken leave from training for 26 weeks or longer during basic training, or 52 weeks or longer during advanced training. Consequently, some of the broader issues that usually accompany the parenting of young children, such as sleep loss, or childcare stresses, are not directly addressed. The essence of the guidelines is the completion of a learning needs analysis and an initial period of level one supervision, with the duration at the discretion of the SOT. The flexibility within the guidelines was mentioned by respondents in both positive and negative framings. The flexibility allows individualisation of the return to work process, but at the risk of potentially problematic and burdensome onus on SOT discretion, and there may be scope for more prescriptive recommendations from ANZCA.
By highlighting gaps in understanding and barriers to the progression of gender equity, we also identified opportunities for the evolution of new cultures to support family-friendly workplaces. Personal experience emerged as a significant driver in attitudes and behaviours, and this is important to recognise if cultural change is to occur, alongside open conversations between trainees and their leaders and commonsense approaches to policy implementation. In re-imagining a culture of family-friendly practices, there needs to be cognisance of personal bias and the use of transparent processes to mitigate this risk (such as a committee rather than an individual to allocate priority specialised study units). In addition, there is a requirement for a clear understanding of contractual and statutory obligations, such as unbiased job protection and the use of personal sick leave to care for unwell children. This needs to be coupled with financial commitment from DHBs and governance from ANZCA to promote elimination of important barriers, accepting that the challenges are different in small departments. Potential strategies include creating truly independent part-time training positions that are not reliant on job-share arrangements, and efforts to destigmatise ‘extended training’ by including ‘parental leave’ as a specific category of leave outside ANZCA training time. The ANZCA curriculum currently allows a maximum of 16 weeks of leave for any purpose during the combined introductory and basic training period, an additional 16 weeks during advanced training and an additional eight weeks during provisional Fellowship training. ANZCA does not distinguish between parental leave and other forms of leave, therefore any leave beyond these limits requires a trainee to enter interrupted training and that may be associated with stigma.
The need for structural support for family-friendly workplaces is not new, nor is it unique to anaesthesia trainees. Literature from the Australasian context is limited in this regard, but a survey conducted by the Royal Australian and New Zealand College of Obstetricians and Gynaecologists found health service deficiencies in establishing systems to support the uptake of parental leave. 27 They described a tension between the expectations of their college, as a vocational training body, and the practicalities of the workplaces which employ their trainees. To provide a framework for pragmatic employer engagement, there may be value in scoping work by ANZCA into projected implementation costs of different interventions within a family-friendly agenda. These would likely range from low cost, such as mentoring programmes, to more complex workforce-related ones.
Strengths and weaknesses
This study explored the views of those in positions of responsibility and influence in anaesthesia training and management within New Zealand, thus providing some insight into the current culture as it affects trainees. The survey’s anonymity enabled frank comments from respondents, and the mixed methods design addressed a limitation in survey research by adding depth to answers, identification of new themes and direction for implementable change.
Although the response rate (39%) is typical of survey research, it is disappointing in the context of individuals who are invested in the professional affairs of anaesthetists, and our findings reflect the views of a small number of respondents. The risk of non-response bias infers that those with strongly held views towards family-friendly practices (sympathetic or otherwise) may have been more likely to complete the survey. The results describe attitudes and perceptions of respondents, but are not corroborated by objective evidence to support responses (for example, whether workplace practices perceived to have been implemented are actually implemented). Results have been interpreted within this limitation.
The use of closed questions carries the risk that nuanced responses are impossible to capture. For example, most questions were presented as multiple choice (either ‘yes’ or ‘no’ or ‘not sure’), which did not allow respondents to indicate that both ‘yes’ and ‘no’ may be applicable answers. This could account for the higher rates of ‘not sure’ responses to some questions, although this was not evident through our piloting or peer review processes. The richness of information we were able to collect through the free-text sections provided some depth and allowed extremes of opinion to be expressed. However, these could not be explored as fully as they would have been through interviews or focus groups, and this would have been useful when answers lacked specificity --- such as those addressing DHB governance.
Another limitation was our inability to attribute responses to the respondents’ roles. This occurred for several reasons: six individuals did not identify their role, the rotational supervisors were grouped with the SOTs, and de-identified free-text comments were uncoupled from the respondent role. It would have been interesting to see if responses were related to different roles because of the differences in responsibilities and reporting lines (ANZCA for the SOTs, and hospital management for the HODs). Furthermore, it may have been useful to delineate the role of rotational supervisors from SOTs; however, the small number of rotational supervisors (five in New Zealand, two of whom are also SOTs) would have potentially compromised anonymity. We do not know why relatively few SOTs responded, and speculate that because the survey was distributed in December it coincided with the annual changeover date for rotating registrars, a time of increased SOT workload.
Caution should be applied before generalising these results to jurisdictions other than New Zealand. At the time of survey distribution, the New Zealand Parental Leave and Employment Protection Act provided up to 22 weeks of paid leave for the primary caregiver, and up to a further 30 weeks of unpaid leave with job protection. Paid parental leave around the time of birth for the non-primary caregiver is determined by employment contracts, with up to two weeks provided for within the SToNZ MECA and six weeks within the RDA MECA. This contrasts with Australia where there are significant differences in paid parental leave between the Australian states, ranging from ten weeks in Victoria to 20 weeks in South Australia (after five years of continuous service). 28 In addition, the survey responses do not reflect trainee experiences, and a similar survey of New Zealand trainees would contribute to a broader perspective and deeper understanding of this subject.
Conclusion
This study adds to the gender equity dialogue in anaesthesia training by describing current attitudes and processes related to a family-friendly culture within the New Zealand anaesthesia training system, from the perspective of leaders in anaesthesia departments. Most of the responses, both quantitative and qualitative, indicate widespread supportive attitudes by those in positions of influence in anaesthetic training in New Zealand. However, the data do expose gaps in current understanding and potential areas of controversy such as work hours, domestic sick leave, return to work processes and paid parental leave for the non-primary carer. These illustrate areas where work needs to be done, and where energy should be placed for further enquiry. This research demonstrates broad conceptual support for family-friendly practices but highlights a discrepancy between the ‘ideal’ and the ‘real’, both attitudinally and structurally. The barriers identified prevent the realisation of a family-friendly workplace and thus perpetuate gender inequity. To redress gender bias seriously requires changes that mostly relate to governance and resources that are needed to enable the widespread implementation of existing family-friendly policies and practices, as well as cultural changes to foster new and creative approaches to managing the ‘caregiver problem’.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20958716 - Supplemental material for The gap between attitudes and processes related to ‘family-friendly’ practices in anaesthesia training in New Zealand: A survey of anaesthesia supervisors of training and departmental directors
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20958716 for The gap between attitudes and processes related to ‘family-friendly’ practices in anaesthesia training in New Zealand: A survey of anaesthesia supervisors of training and departmental directors by Jane C Carter and Alexander L Garden in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
The author(s) are grateful to the study participants for their time and insights, and for the support and assistance from the Wellington Department of Anaesthesia and ANZCA New Zealand Office. Thanks to Daniel Frei for his assistance in the survey development, Liam Kavanagh for de-identifying comments in the raw data prior to analysis and Lisa Woods, School of Mathematics and Statistics, Victoria University of Wellington, for providing statistical advice.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JCC is a member of the ANZCA Gender Equity Sub-Committee, although her membership postdates the conduct of this research and submission of the initial manuscript. All opinions presented in this manuscript belong to the authors alone. ALG has no conflict of interest to declare.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.