
Abstract
Regional anaesthesia is a fundamental aspect of anaesthesia practice. Structured Fellowships in regional anaesthesia facilitate the development of expert clinicians, scholars and future leaders. The Australian and New Zealand College of Anaesthetists accredits training sites for the final year of Fellowship training but does not outline specific guidance for subspecialty training. Based on evidence from a systematic literature review and best-practice medical education principles, the ideal structure for a regional anaesthesia Fellowship programme in Australia and New Zealand is outlined in four categories: (a) structure and duration of training; (b) educational aspects; (c) institutional organization; (d) evaluation and improvement. Departments may use this resource to help design, implement and improve their Fellowship programmes while trainees may employ it as a reference to achieve their learning goals at any training stage. Continuing professional education plays a central role in achieving and maintaining mastery of regional anaesthesia competencies.
Introduction
The role of regional anaesthesia (RA) in clinical practice has evolved over the past decade, both in terms of its technique and clinical utility. There is evidence that ultrasound-guided RA improves block success rates, 1 onset speed, 2 block quality 2 and reduces some complications, 3 which has accelerated the uptake of RA in clinical practice. Ultrasound guidance has facilitated the development of novel techniques for truncal and limb surgery, such as the quadratus lumborum, pectoralis, transversus abdominis plane, erector spinae plane and adductor canal blocks. RA is an important alternative to general anaesthesia, and has a role in multimodal, opioid-sparing approaches to perioperative analgesia.
When launching their new curriculum in 2013, the Australian and New Zealand College of Anaesthetists (ANZCA) recognized RA as a core skill or ‘clinical fundamental’ to be taught to all anaesthesia trainees. 4 In the USA, the Accreditation Council for Graduate Medical Education (ACGME) has recognized ‘regional anesthesia and acute pain’ as a formal subspecialty and accredits Fellowship programmes, 5 a status shared only with adult cardiothoracic anaesthesiology, critical care medicine, obstetric anaesthesiology, pain medicine and paediatric anaesthesiology. These initiatives reflect the importance of RA within our specialty.
Structured RA Fellowships are more likely to allow delivery of a curriculum and learning objectives to develop experts, educators and future leaders, within Australian and New Zealand teaching departments. ANZCA currently accredits hospitals as appropriate sites for the final year of Fellowship training, termed the ‘provisional Fellowship year’ in training nomenclature, 6 but does not provide specific learning objectives or curricular guidance for subspecialty training.
This paper aims to outline the ideal structure for an Australian and New Zealand RA Fellowship programme, based on available evidence and conforming to best-practice medical education principles. Departments may use these recommendations to help design, implement and improve their Fellowship programmes, in order to produce future leaders, experts and scholars in RA. Trainees may use this resource as a reference to achieve their learning goals at any stage of their training. The evidential basis for selected recommendations is outlined in the Discussion section.
Methods
We undertook an electronic literature search up to May 2018 for articles on RA Fellowship and training programmes, using the Embase and Medline databases with the following search terms: (‘regional anaesthesia’ OR ‘regional anesthesia’) AND (‘fellowships’ OR ‘training’). To complement the primary search strategy, we performed a targeted search of institutions known to have published guides on RA subspecialty training and curricular documents from vocational training colleges in Australia and New Zealand, the UK and Canada. Returned records and their abstracts were collated and independently reviewed by all authors for relevancy. Included abstracts met the following criteria: endorsed accreditation or published curricula on RA training, expert consensus guidelines on RA training, review articles on RA training, any other relevant article related to RA training and education. The full-text versions of articles were read and summarized by each author independently. Articles were included if all three authors agreed. Articles without complete agreement were discussed using summary notes, and a consensus was reached between all authors to include or exclude.
Results
Literature search
There were 899 records identified from the database search after removing duplicates, 18 records from the targeted search of known training providers and 13 records from secondary sources; 183 records were shortlisted and 85 reviewed for qualitative synthesis (see Figure 1 for flow diagram). The complete list of reviewed records is included as supplementary material.
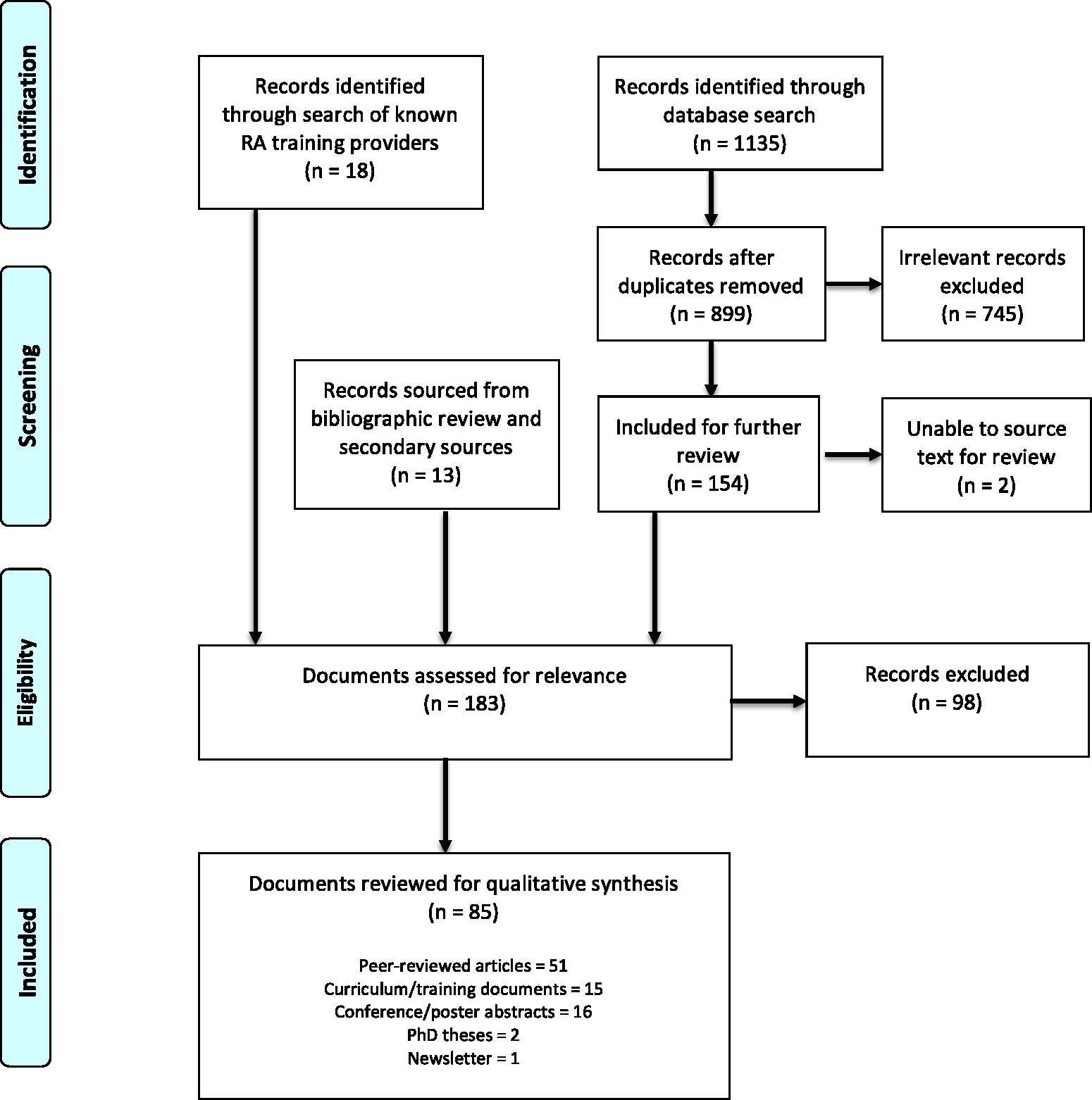
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart. RA, regional anaesthesia.
Structure and duration of training
Application requirements
In the context of ANZCA training, prospective Fellows should have completed all requirements of Advanced Training Year 2 and be eligible for Provisional Fellowship Training at the commencement of their Fellowship. 6 Suitability of overseas applicants should be evaluated on a case-by-case basis. The overall selection process should incorporate elements designed to maximize transparency and reduce the influence of unconscious bias. A position description should outline the desired qualities of applicants and follow institutional selection guidelines.
Duration
A duration of six to 12 months is recommended to obtain sufficient clinical exposure. A 12-month Fellowship is preferred because it presents more opportunity for engagement in scholarly activities. Close attention should be given to rostering practices in six-month Fellowships to ensure adequate opportunity to perform RA procedures, with a higher proportion of clinical sessions dedicated to RA lists (see ‘Fellowship structure’ below).
Fellowship structure
A minimum of 50% of clinical time should be allocated to sessions amenable to performing RA, including acute pain sessions. While spinal and lumbar epidural blocks are technically RA techniques, trainees should have attained an acceptable level of competence and these need not form a significant component of an RA Fellowship.
Optimal RA outcomes are best achieved with a comprehensive understanding of acute pain management. Fellows should have regular supervised acute pain ward rounds to assess the efficacy of RA, optimize postoperative analgesia, manage local anaesthetic catheter infusions and refine their approach to acute on chronic pain patients. In the latter part of their Fellowship, Fellows should be competent in leading acute pain rounds.
Educational aspects
Learning outcomes
Each Fellowship should have a list of learning outcomes that relate to how the Fellowship is structured. A set of clear and concise learning outcomes allows both learners and teaching staff to have a clear and shared understanding of the competencies expected of the former at the end of the Fellowship. It also allows the department to state what it is they want the learner to achieve. The details of the Fellowship structure should be tailored to meeting these learning outcomes. Prospective applicants may use these learning outcomes to gain insight into the Fellowship structure when evaluating their career options. Learning outcomes should be periodically reviewed as new developments occur and clinical practices evolve. An example of learning outcomes for an RA Fellowship is shown in Table 1.
Learning outcomes for the Regional Anaesthesia Fellowship in North Shore Hospital, Auckland. 7
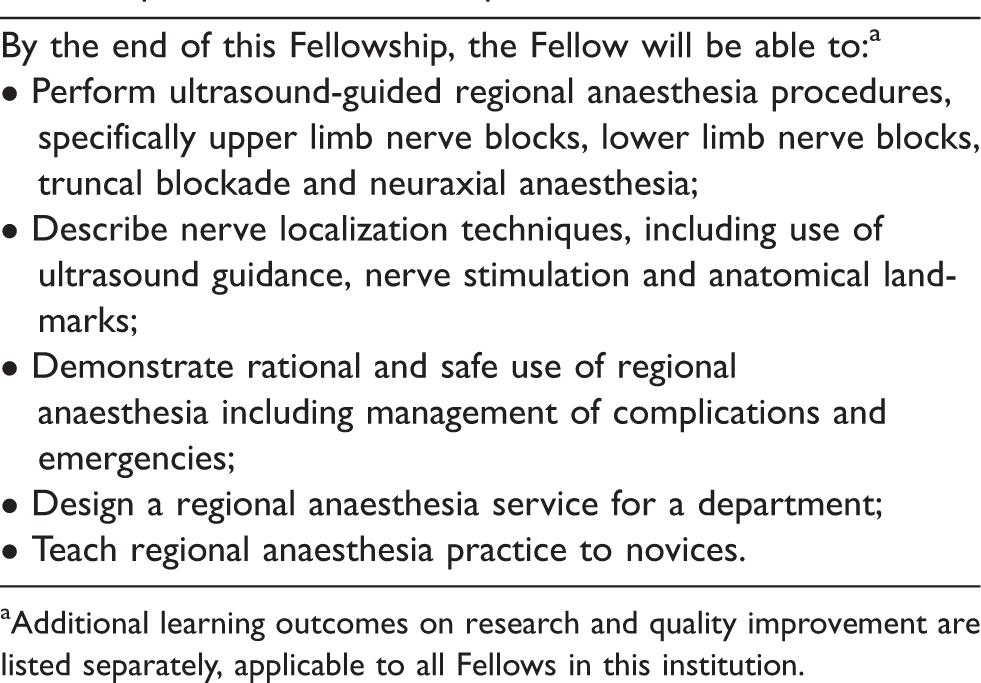
aAdditional learning outcomes on research and quality improvement are listed separately, applicable to all Fellows in this institution.
RA procedure volume
Minimum volumes for different RA cases or procedures are required to ensure Fellowships provide the appropriate clinical exposure necessary to develop RA expertise (Table 2). However, case volumes are not the sole marker of clinical competence, as individual learners will exhibit differences in their learning curves with variable prior RA experience. While learner-centred progression is an important aspect of training, minimum volumes ensure exposure to the range of complexity encountered in clinical practice. All items described in this section complement each other and should be viewed collectively when designing and evaluating a fellowship programme.
Recommended minimum volumes for Australian and New Zealand regional anaesthesia Fellowships.
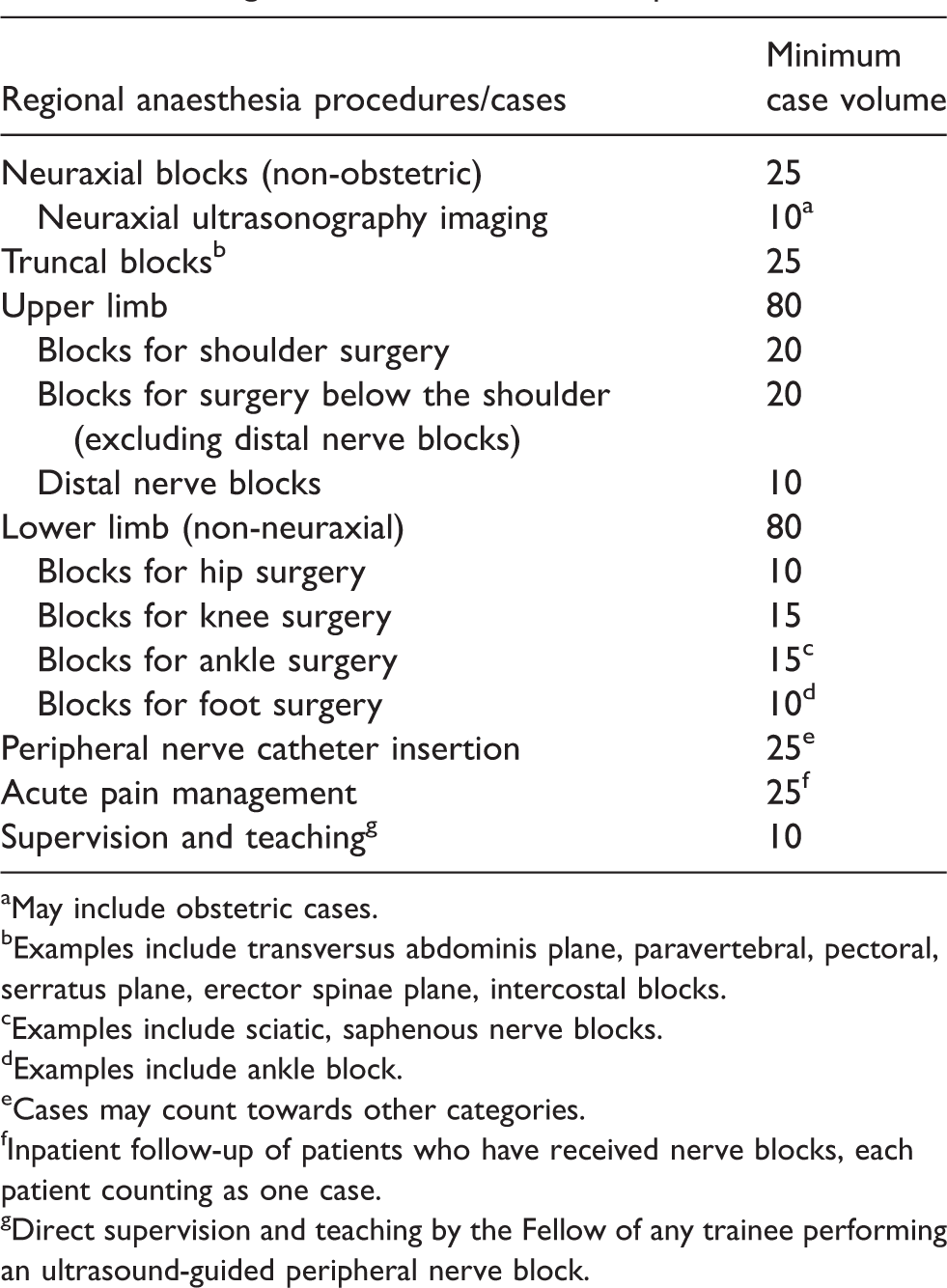
aMay include obstetric cases.
bExamples include transversus abdominis plane, paravertebral, pectoral, serratus plane, erector spinae plane, intercostal blocks.
cExamples include sciatic, saphenous nerve blocks.
dExamples include ankle block.
eCases may count towards other categories.
fInpatient follow-up of patients who have received nerve blocks, each patient counting as one case.
gDirect supervision and teaching by the Fellow of any trainee performing an ultrasound-guided peripheral nerve block.
Instructional activities
Teaching and learning for RA Fellows should not be confined to the clinical environment. Exposure to structured teaching is important to develop the Fellow’s own framework of knowledge. Fellowship programmes should incorporate multiple modes of instruction, such as part-task trainers and high-fidelity simulation. Part-task trainers and phantom models should be used to teach ultrasound needling techniques and simulate nerve blocks; high-fidelity simulation may be used to teach patient safety, emergency management and non-technical skills; cadavers or anatomical models may be used to teach clinical anatomy. Fellows should also be encouraged to attend a formal RA skills workshop or cadaver workshop, as these are opportunities to learn nerve blocks which may not be regularly practised in their department, and to experience a range of different clinical teaching styles. Attendance at a national or international RA conference should be strongly encouraged. Formal qualifications such as the European Diploma in Regional Anaesthesia or the MSc in Regional Anaesthesia, offered by the European Society of Regional Anaesthesia and the University of East Anglia, respectively, are available via distance-learning. Their curricula may be useful to guide learning but participation should be at the discretion of the Fellow.
Scholarly activities
Expertise in RA includes competence in related scholarly activities. The Fellowship programme should be structured to provide guidance and facilitate involvement in teaching, research, quality improvement initiatives and leadership roles. Presentations to journal clubs or departmental meetings should occur as part of the role. While it may not be possible for a department to offer all these opportunities, teaching responsibilities and audit activities should be mandatory. The ANZCA Educators Program is a short course offered by ANZCA as a basic introduction to medical education and is recommended for all RA Fellows. Sufficient regular and protected non-clinical time should be allocated for scholarly activities to take place.
Assessment
All RA Fellows should maintain logbooks to determine minimum case volumes and breadth of experience. However, logbooks on their own are a less than ideal measure of competence. Formative assessment (assessment for learning) should be incorporated into the Fellowship programme through the provision of directly supervised lists for the duration of the programme, at a minimum frequency of two sessions (one day) per week. Direct supervision should be more frequent at the start of a Fellowship programme, as the Fellow begins their learning and is introduced to what may be an unfamiliar clinical environment. Informal feedback should be provided to the Fellow during these supervised sessions, and the Fellow should, from the outset, be encouraged to seek feedback from supervising clinicians. Workplace-based assessments, such as a Direct Observation of Procedural Skills (DOPS) tool or multi-source feedback, may be used if a formal written record is preferred. The Fellowship programme director should collate feedback on the Fellow’s performance from department members, including the Acute Pain Service team, and provide a summary to the Fellow at regular intervals during the Fellowship programme.
Institutional organization
ANZCA Provisional Fellowship accreditation
RA Fellowship programmes should seek prospective accreditation from the ANZCA Provisional Fellowship Subcommittee to ensure that all training requirements of the Provisional Fellowship year are met.
Institutional resources
The department should provide sufficient resources to facilitate an RA Fellowship. This includes relevant equipment (ultrasound machines, appropriate needles, equipment for training) and space for performing RA procedures, if not done in the operating room. A minimum of one session a week should be set aside as protected non-clinical time to allow for scholarly activities. Rostering practices should be flexible in order to incorporate regular and adequate exposure to a variety of RA lists, with the required levels of supervision. A system for follow-up of RA complications should be in place within the department.
Staff
A specialist anaesthetist with RA expertise and vocational registration in Australia or New Zealand should be appointed as the Fellowship programme director, to oversee the RA Fellowship programme. They are responsible for appointments, programme structure, monitoring progress with learning, provision of feedback and supervision of scholarly activities. Some responsibilities may be delegated to other members of the department, with appropriate oversight. There should be a minimum of three department members possessing RA expertise who are available to teach and supervise the RA Fellow.
Evaluation and improvement
Logbook review
Final logbook reviews will help determine if a programme is able to deliver the clinical experience necessary for an RA Fellowship, in terms of volume and variety. Departments may use this information to determine if allocation to RA sessions correspond to actual RA procedure performance, and to make adjustments for the future.
Feedback from Fellow
Fellows should be given the opportunity to provide formal feedback on the structure of the programme, quality/quantity of teaching, staff interaction, non-clinical activities and any other aspects of their employment. Positive experiences can be reinforced and should be fed back to the department. Fellows should be allowed to air grievances, complaints, or reports of negative experiences in a safe environment, free of punitive repercussions. Departments should investigate negative reports and take necessary action if warranted, in order to provide the optimal educational experience for their Fellows.
Departmental review
Wider departmental reviews should incorporate a review of the Fellowship programme, and how it interacts with other departmental functions. Evaluation and improvement opportunities should aim to improve the educational experience, while balancing obligatory service requirements. Short observation attachments at other departments that offer RA Fellowships may help inform the review process. The frequency of departmental reviews is at the discretion of each department, but these should be at regular intervals.
Discussion
This paper outlines a recommended structure of an RA Fellowship in Australia and New Zealand, in order to produce future experts, scholars and leaders in RA. It is modelled on similar documents produced in the USA,8–10 evidence-based, and incorporates the most recent developments in RA education. Complete mastery of all RA competencies during a Fellowship training period is unlikely, and the role of continuing professional education and lifelong learning cannot be over-emphasized. The recommendations in this document are not absolute requirements, as Fellowship programmes should be designed according to the context of local institutions (local skill-mix, cases performed, surgeon preferences and department organization). This document serves as a guide for this heterogeneity in practice and structure. Novel approaches to education and clinical practice should be encouraged. For example, while uncommon in Australia and New Zealand, instituting RA block teams allows for more focused training opportunities with the added benefit of increased workflow efficiency,11,12 improved block effectiveness as measured by pain scores 13 and decreased failure rate. 12
Volume of practice
The RA knowledge and skills outlined in the ANZCA training curriculum reflect the requirements of a competent generalist with some basic knowledge of peripheral nerve blocks. A minimum of three RA workplace-based assessments, in the form of a DOPS tool, are required throughout ANZCA training—one each for a spinal block, upper limb plexus block and lower limb plexus block. 4 In addition, two neuraxial block DOPS are required specifically for obstetric anaesthesia, one for paediatric inguinal or penile surgery and one for regional eye blocks. 4 The minimum volumes of practice for different blocks are described in Table 3. We stress that these are minimum requirements, and trainees may well exceed these volumes. Data on ANZCA trainee RA caseload has not been published but recent data from the USA show large variations between training sites. 14 While sufficient procedural opportunities are necessary to develop expertise, they should not be used as the sole metric. A defined period or volume of clinical exposure does little to advance trainees beyond minimal competence unless accompanied by quality assessment and educational feedback. 15 Targeted formative assessment and feedback is necessary to account for the large variability in the learning curves of individual learners, 16 and can in itself result in shorter learning curves and decreased technical errors. 17 In addition to clinical skills, non-clinical leadership and scholarship competencies are required to manage an RA service, advance the quality of care and teach future RA clinicians.
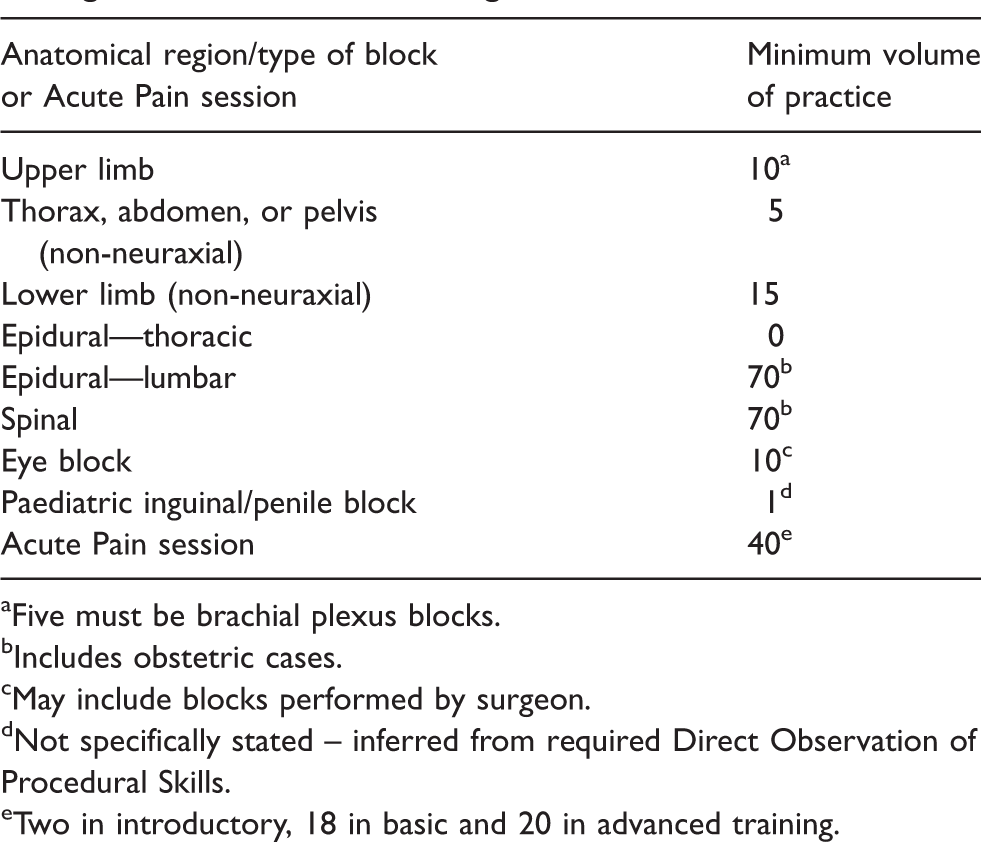
aFive must be brachial plexus blocks.
bIncludes obstetric cases.
cMay include blocks performed by surgeon.
dNot specifically stated – inferred from required Direct Observation of Procedural Skills.
eTwo in introductory, 18 in basic and 20 in advanced training.
The recommended minimum case volumes in this paper are based on the assumption that an acceptable level of competence has been achieved for lumbar epidural and spinal blocks, as expected of a trainee at the end of their vocational training. We have not stated minimum requirements for eye blocks, head and neck blocks, and paediatric blocks. While experience with these blocks is desirable, they are not essential for an RA Fellowship, based on international guidelines. Minimum case volumes for other RA programmes are outlined in Table 4 for comparison. Similar to the ACGME, we have taken the approach of classifying blocks by site of surgery. It is impractical to impose minimum case volumes for each possible nerve block due to local practice and expertise. For example, surgery on the forearm is amenable to supraclavicular, infraclavicular, or axillary nerve blocks. New research or novel approaches may result in a particular nerve block to be demonstrably superior in the future, but the site of surgery is unlikely to change.
Minimum volume of practice requirements for other regional anaesthesia Fellowship or training programmes.
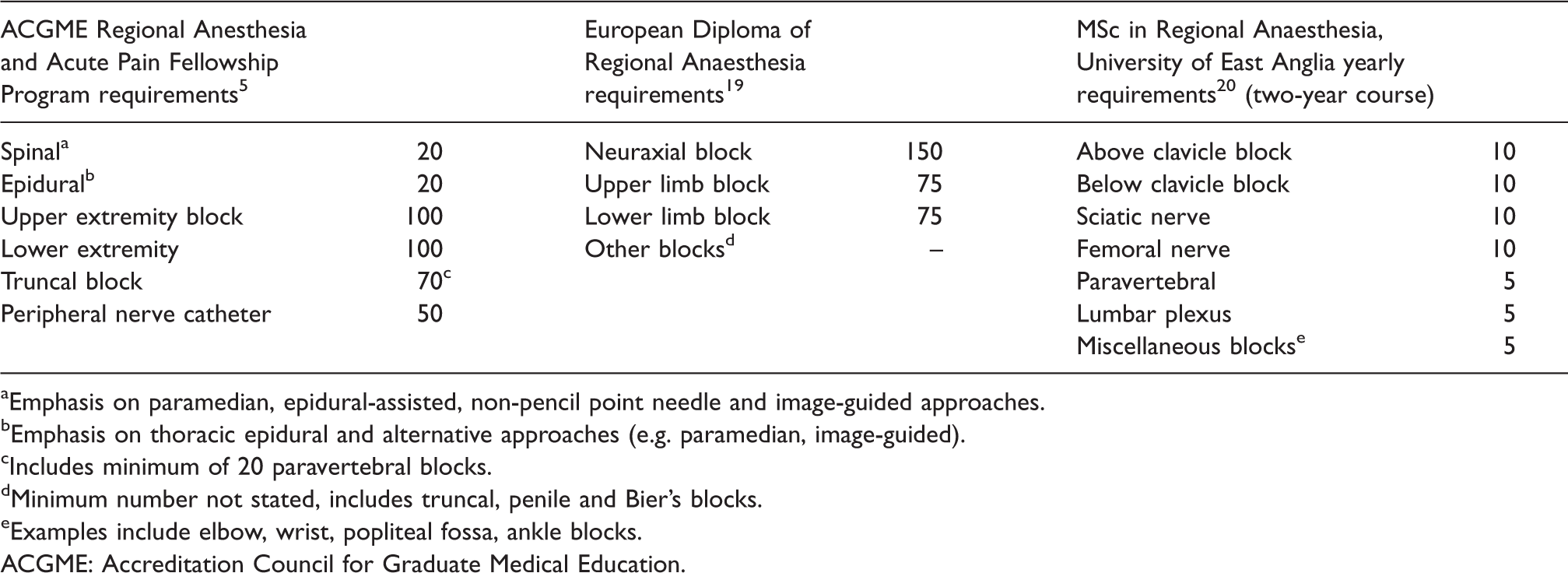
aEmphasis on paramedian, epidural-assisted, non-pencil point needle and image-guided approaches.
bEmphasis on thoracic epidural and alternative approaches (e.g. paramedian, image-guided).
cIncludes minimum of 20 paravertebral blocks.
dMinimum number not stated, includes truncal, penile and Bier’s blocks.
eExamples include elbow, wrist, popliteal fossa, ankle blocks.ACGME: Accreditation Council for Graduate Medical Education.
Instructional methods
A variety of instructional activities may be utilized to supplement core teaching in the clinical environment. There is acknowledgement that the old adage of ‘see one, do one, teach one’ is an outdated and inferior method for teaching complex technical procedures and impairs patient safety and quality of care.21,22 Each mode of instruction has its own benefit and cost profile, and simple cost-effective instructional methods are not necessarily inferior in all aspects. In a study comparing meat-based models with human cadavers, there was no difference in learning between groups of novice trainees. 23 Multiple other cost-effective teaching models have been described. 24 The most commonly utilized formal teaching tools in RA Fellowships are live models and phantoms, though just over half of RA Fellowships worldwide incorporate cadaver dissection. 25 It is likely that different levels of training require emphasis on different modes of instruction. 26 Simulation-based RA training is associated with improved knowledge and skills acquisition. 27 Web-based RA training is becoming increasingly feasible but has not been shown to be superior to traditional teaching, with older evidence indicating that the time and expense for developing complex web-based training modules may not be justified. 28 Newer methods of instruction, such as virtual reality simulation, 24 may be considered if feasible although no evaluation studies have been published.
Competency-based medical education
It has been proposed that trainees should be competent at ultrasound image interpretation, needle visualization and local anaesthesia injection prior to performing RA in the clinical setting.22,29 RA Fellows may have differing competence backgrounds at the start of their Fellowship, and departments should be prepared to accommodate this with a brief period of teaching and assessment in parallel with initial clinical exposure. Recently, 28 competency-based assessment tools in RA were reviewed against consensus ideal characteristics. 30 Validated multiple-choice question assessments are useful to check theoretical knowledge recall. 31 Procedural performance is best assessed using either of the two validated checklist-global rating scale tools, published by Cheung et al. (2012) (ultrasound-guided procedures only), 32 and by Chuan et al. (2015) (all RA procedures). 33 These tools have sufficiently high reliability to be used for either summative or formative assessments. In the latter, better educational outcomes are found if deliberate practice techniques are paired with structured feedback from expert faculty. 34
Scholarly activities
Incorporation of scholarly activities in a Fellowship is essential to develop future RA experts. Teaching should not be confined to the clinical environment. As future experts, RA Fellows should gain competencies and experience in teaching. Once a certain level of clinical expertise has been achieved, RA Fellows should take responsibility for teaching junior trainees the basics of RA. This should include needling skills, ergonomics and the performance of basic blocks. The personal goals of RA Fellows conducting research are to participate in different types of research (leading to publication in peer-reviewed journals), gaining experience and a broader knowledge in research-related topics, and practical experience with the publication and presentation process. 35 Some pure research Fellowships in anaesthesia instruct prospective applicants to submit proposals for research projects, including supporting literature, along with their formal application. 35 Research projects should be presented at national meetings (or larger), where possible. 36 Research may be difficult to complete within the period of a Fellowship but many tasks can be completed with forward planning from the point of the job offer being accepted (e.g. initial discussion with supervisor, determining the research question, literature search, ethics submission, funding application). 35 The design of larger research projects may necessitate cooperation between successive Fellows over a longer period. Some have suggested that RA Fellowships be extended to two years in order to incorporate a compulsory research component. 37 Departments with less research expertise and resources may seek to forge links with other departments to jointly conduct research projects. Clinical audit is an important component of quality improvement and the RA Fellow should be leading departmental RA audits. These may include collaboration with surgical teams, especially with topics related to patient outcomes. Experience in positions of responsibility with scholarly activities will assist in developing leadership skills, the intent of which should be made explicit to the Fellow.
Limitations
The recommendations in this document are based on current published evidence and requirements of other bodies offering RA subspecialty training. As evidence and practice evolve, these recommendations will require periodic review. Structures of current RA Fellowship programmes in Australia and New Zealand were not evaluated when drafting these guidelines, as current practice need not influence recommendations for best practice. However, current RA Fellowship structures should be considered in any mandatory guidelines for them to be feasible, including the incorporation of programme evaluations and input from RA Fellowship programme directors.
Ultrasound-guided RA is a relatively new skill and departments are still learning how to best teach Fellows. It is unlikely that any current RA Fellowship programme delivers all the ideals outlined in this document. However, having a reference standard will enable programmes to evaluate strengths and weaknesses, compare against other programmes and improve their structure to provide a better educational experience for Fellows.
Fellowships structured to only provide exposure to RA caseload may still be a pathway to individual competency but are not ideal in supporting the development of future RA leaders. Working in a high-quality RA Fellowship is the preferred vehicle for exposure to the breadth of RA education and practice, however it is only the start of the journey. This document does not discuss methods for lifelong learning of RA, but the general principles are well addressed by most continuing professional development programmes.
Conclusion
This paper is a blueprint for departments to set up, develop and refine RA Fellowship programmes. It supplies clear objectives for Fellows to direct learning efforts, and develop clinical and non-clinical expertise. The structure is designed to improve the quality of RA training and develop future leaders in RA. Institutions should consider local practice and context when using this paper. All RA Fellowship programmes should emphasize self-directed learning, continuing professional education and lifelong learning.
Supplemental Material
Supplemental material for Recommendations and resources for regional anaesthesia Fellowships in Australia and New Zealand
Supplemental Material for Recommendations and resources for regional anaesthesia Fellowships in Australia and New Zealand by Navdeep S Sidhu, Alwin Chuan and Christopher H Mitchell in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
We would like to acknowledge of the Regional Anaesthesia Special Interest Group (RASIG) executive committee for their feedback on this guideline.
Declaration of conflicting interests
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All authors are RA Fellowship programme directors in their respective institutions. Two authors (NS and AC) have advanced qualifications in medical education.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.