
Abstract

Anaesthesia is a waste-intensive specialty, mainly because of the use of many disposable products. 1 Waste production in anaesthesia is not consistent though, and this may be partially related to variation in the type and quantity of disposable products used to provide anaesthesia care.2,3 We undertook an observational study to identify factors related to waste and cost during anaesthetist-provided sedation for gastrointestinal endoscopy in our hospital. We felt that although differences in waste (and cost) for any given case might be relatively small, the cumulative total might be potentially significant.
Following approval by the University of Tasmania’s Human Research Ethics Committee (Project ID: 23043), a prospective observational study was conducted at the Launceston General Hospital, Australia, from 15 October to 19 November 2020. We included 57 patients, 13 anaesthetists and nine gastrointestinal endoscopists, each providing consent to participate. The primary outcome was waste generated per min of sedation time. Cost was also estimated.
Eligible patients were adults with American Society of Anesthesiologists physical status class 1–3, who were not pregnant, presenting for elective upper or lower gastrointestinal endoscopy under anaesthetist-provided sedation. They were between the ages of 23 and 88 years, being 58% male and 42% female. Thirty-nine percent of the cases had an upper gastrointestinal endoscopy alone, 51% had colonoscopy alone and 10% had both.
The anaesthetists included a mix of eight consultants, one senior anaesthesia trainee, two junior anaesthesia trainees and two other junior doctors in anaesthetic rotations. They were advised not to alter their usual sedation practice during the study. The term ‘lead anaesthetist’ is applied to any anaesthetist, irrespective of seniority, who led at least one sedation case.
Included waste was from disposable drug and fluid products used by anaesthetists for anaesthetic care purposes. It did not include waste from airway equipment, personal protective equipment or products administered for endoscopy purposes.
An independent observer completed an inventory of disposable drug and fluid products administered during each sedation. The observer collected data on eight days mostly by convenience sampling. The weight (grams) of waste of each item was obtained using a digital weighing scale while costs (in Australian dollars) were independently supplied by the hospital pharmacy and stores staff. 4 After all cases had been completed, anaesthetists were asked via a de-identified electronic survey about their motivating factors for choosing disposable products and their willingness to change practice to reduce waste if it did not affect clinical outcomes.
The descriptive analysis involved calculating medians, interquartile ranges and ranges for waste and cost production overall, and for subcategories of various disposable product choices. Average waste and cost production during and beyond the first ten min of sedation, and average sedation time were also calculated.
This study found a large range in waste production per min of sedation (0.66–21 g/min) among anaesthetists from disposable drug and fluid administration products used to provide sedations for elective gastrointestinal endoscopies (Table 1 and Figure 1). A large range was also calculated in the cost per min of sedation (A$0.04–3.18/min). All anaesthetists generated more waste and cost per min in the first ten min than later in the procedures. The average sedation time was 21 min.
Waste (grams per min) and cost (Australian dollars per min) production per min of sedation overall and per various subcategories in medians (interquartile range (range)).
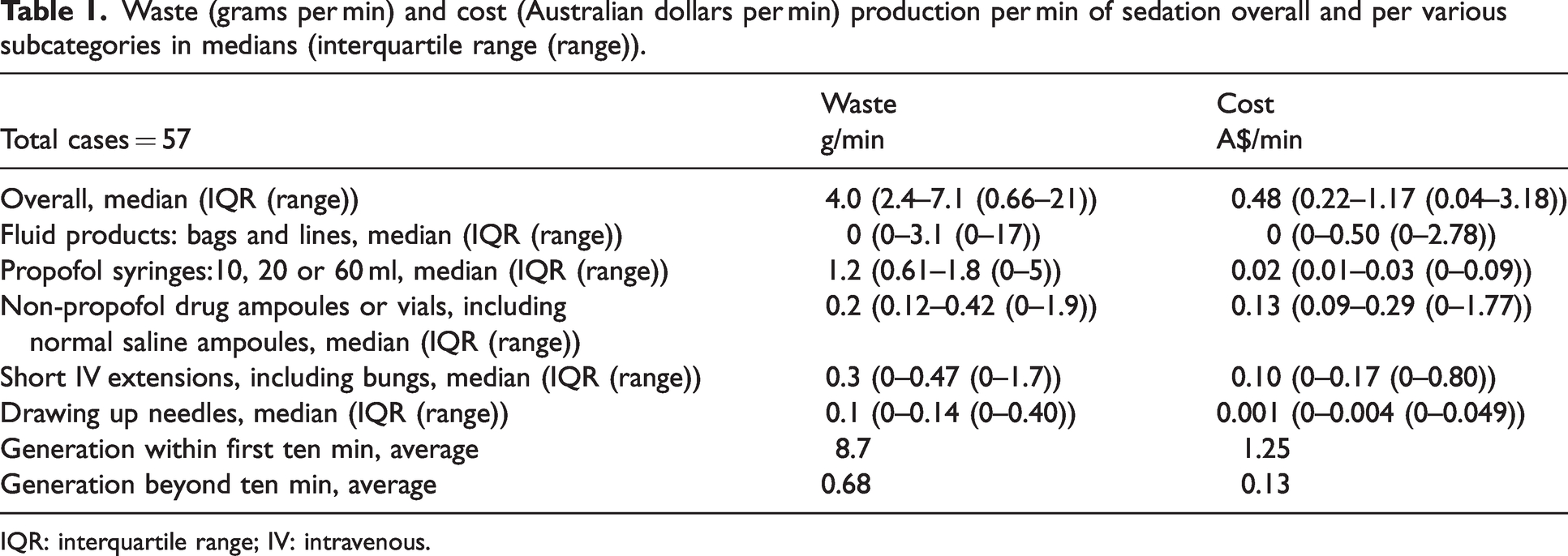
IQR: interquartile range; IV: intravenous.
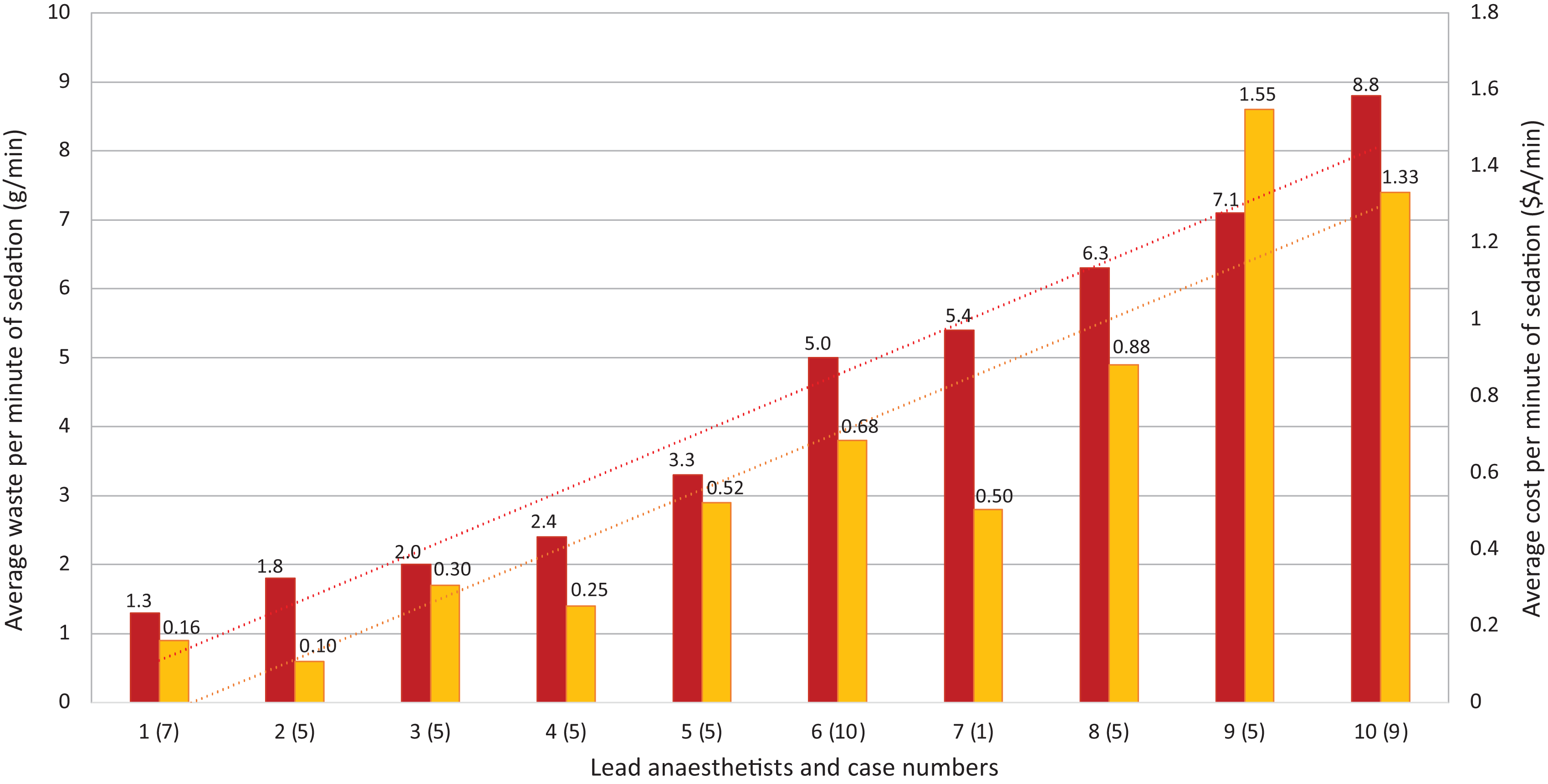
Average waste and cost per min of sedation.
A key observation was that intravenous fluid use substantially increased both waste and cost production. A 2014 observational study found no association between intravenous fluid use and adverse outcomes for colonoscopies. 5 A 2006 clinical trial showed no advantage from routine intravenous fluid use in preventing adverse events for colonoscopies. 6 Further research could better define waste and cost savings from varied intravenous fluid patterns for upper and lower gastrointestinal endoscopies, including any effect on patient outcomes.
Other potential contributors to waste and cost production were identified, but the magnitude of their contributions was far less than the use of intravenous fluids. Reuse of propofol syringes within a given case would clearly reduce waste production, but this practice cannot be condoned as it may increase the risks of iatrogenic bacteraemia. 7 Using short intravenous extension lines and drugs other than propofol were identified as contributors to cost production; these may be modifiable choices in many circumstances.
Fifty-four percent of anaesthetists replied to the survey and reported heterogeneously in terms of motivating factors for disposable product choices (clinical, economic or environmental). Most were open to altering their practices to reduce waste if it did not affect clinical outcomes.
We cannot comment on patient safety or satisfaction, proceduralist satisfaction or any clinical outcome measure, and can make no recommendation on anaesthesia choices as a result of this study due to its heterogeneity, unblinded nature and small sample size. Nevertheless, the information we have collected may be used as the basis for future studies.
In conclusion, we observed large ranges in waste and cost production from anaesthetist-provided sedation for elective gastrointestinal endoscopies in our hospital over the sampling period. Intravenous fluid use was the main factor associated with higher waste and cost production. Further studies would be required to determine whether anaesthesia techniques that involve higher waste and cost production (such as routine intravenous fluid use) are justified in terms of benefits to patients. Future research should ideally control for anaesthetist seniority, procedure type and sedation duration, and include disposable products from airway and personal protective equipment.
Footnotes
Acknowledgements
Iain Robertson – study planning, statistical advice, protocol reviewing; Kath Ogden – study planning advice, protocol reviewing; Jane Niecamp – protocol reviewing; Kate Bretzke – product weighing assistance; Sonia Mackenzie – product pricing assistance; Niki Dalton – product pricing assistance; Natasha Kelder – product pricing assistance; Nathan Bishop – product pricing assistance; Alistair Park – manuscript reviewing.
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.