
Abstract
Patients presenting for elective surgery in the Bay of Plenty area in New Zealand are increasingly elderly with significant medical comorbidities. For these patients the risk–benefit balance of undergoing surgery can be complex. We recognised the need for a robust shared decision-making pathway within our perioperative medicine service. We describe the setup of a complex decision pathway within our district health board and report on the audit data from our first 49 patients. The complex decision pathway encourages surgeons to identify high-risk patients who will benefit from shared decision-making, manages input from multiple specialists as needed with excellent communication between those specialists, and provides a patient-centred approach to decision-making using a structured communication tool.
Introduction
Bay of Plenty District Health Board is situated in the central north island of New Zealand, and serves a population of just over 234,000. We have a growing and ageing population, with 19% currently over the age of 65 years, predicted to increase to 24% in 2026. The fastest growing age group in our population is those aged 75 years and above, growing at 3.6% per annum. 1
Across its various facilities the district health board undertakes approximately 12,000 elective operations annually. 1 Reflecting population trends, the number of very elderly patients presenting for surgery in our region is increasing (unpublished internal audit data). Advanced age is associated with an increased likelihood of perioperative complications and poor outcome. 2
Description of the quality improvement initiative
In 2017, a multidisciplinary quality improvement working group comprising anaesthetists, intensive care specialists and surgeons recognised a gap in our pre-assessment pathways for our highest risk patients. Existing high-risk pre-assessment pathways were focused on optimisation and preparation, which are important for good perioperative outcomes, but occur after a decision has been made to operate. We identified a need for shared decision-making earlier in the perioperative journey when the risk–benefit balance of an operation was uncertain. This led to a quality improvement initiative using small scale tests of change culminating in the development of a complex decision pathway (CDP).
Referrals to the CDP come from surgeons, who rather than booking patients for surgery and awaiting feedback from anaesthetists (our traditional approach), suggest to the patient that further specialist input is required to help with decision-making prior to booking. These referrals are then triaged by anaesthetists with other specialist input and investigations requested as needed. Once the necessary investigations and opinions have been collated, the patients are booked to a clinic appointment with an anaesthetist and intensive care specialist. Two hours are reserved for each patient to allow specialists to review medical histories, undertake risk scoring (which has evolved during testing of the project and now includes American Society of Anesthesiologists physical status classification, 3 American College of Surgeons national surgical quality improvement programme surgical risk calculator, 4 , 5 nzRISK 6 , 7 and the clinical frailty scale), 8 , 9 consult with other specialists by phone or in person and to provide adequate time for documentation. Approximately one hour of this time is spent with the patient and their family/whanau or support persons. As well as a standard medical assessment the clinicians engage the patient in a goals-of-care conversation using a structured communication tool called the serious illness conversation guide (Aotearoa serious illness conversation guide (SICG), adapted with consumers in New Zealand, August 2018, Supplementary Appendix 1, reproduced with permission from the New Zealand Health Quality and Safety Commission). Where appropriate, other staff members, including members of our cultural liaison team, also attend this appointment.
As well as offering training, we provide the SICG for clinicians to use in the clinic along with a suggestion for how these questions/prompts may fit around standard pre-assessment questions. A documentation template is provided for clinicians to document the information elicited from the SICG questions, as well as other medical information and risk scores. As part of the documentation a recommendation is made to the surgeon and patient and this is able to be framed in terms of the patient’s healthcare goals.
When appropriate, those patients likely to proceed to surgery are supported to engage in perioperative advanced care planning. For these patients the escalation of care that could occur in the event of a perioperative complication is discussed and the patient’s wishes, along with the advice of the intensive care clinician, are documented. Optimisation planning is commenced at this time and continued further once the patient is booked for surgery and enters standard pre-assessment pathways.
Those patients who choose not to pursue surgery are often referred to other specialty services such as Health in Aging (geriatricians), allied health services, chronic pain specialists and occasionally palliative care.
Methods
During this quality improvement initiative, we prospectively collected audit data from patients participating in the CDP at the Tauranga campus in order to understand better patient demographics, decisions and referral sources. An out-of-scope exemption was obtained from the Health and Disability Ethics Committee (HDEC) for collection of this data (19/NTB/177), and locality approval was obtained from the Bay of Plenty Clinical School (2020-59).
Results
Between commencement of the pathway in August 2018 and January 2020 (18 months) 49 patients have participated in the CDP at the Tauranga campus. Additional patients have participated in the pathway at the Whakatane campus but are excluded from this audit.
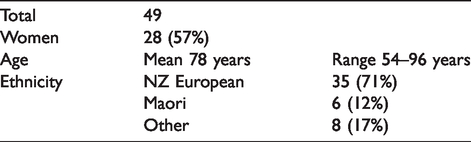
The demographic descriptors of the patients seen in the pathway are listed in Table 1.
Demographics.
The 49 referrals to the service have come from 23 individual surgeons (61% orthopaedic surgeons, 27% general surgeons and 12% other surgical specialties).
The primary indication for surgery in the majority of patients was relief of pain and/or improvement in mobility (63%), but a number of patients had treatment of cancer as the indication for surgery (18%). The remaining indications (19%) included recurrent infections, incarcerations of herniae and functional indications.
Twenty-one (43%) patients received input from other specialties or services as part of their journey through the CDP. These services included geriatric medicine, cardiology, respiratory medicine, renal medicine, neurology and allergy specialists.
Just over half of the patients seen through the CDP chose a non-operative course (26 patients, 53%). Nineteen patients (39%) decided to proceed with surgery and were supported to undertake perioperative advance care planning as part of the process. A final four patients (8%) remain undecided at the time of this audit.
Five (10%) of the patients have died over this 18-month period. One of these patients had decided to proceed with an operation and died three and a half months postoperatively, and the other four patients had chosen not to have surgery.
Discussion
There is an increasing recognition in perioperative medicine of the importance of shared decision-making and multi-specialist input into perioperative assessment and care. 10 We have designed and tested a perioperative pathway allowing surgeons and patients to access multi-specialist input, detailed medical assessment and shared decision-making prior to making the decision to book patients for surgery.
Helping patients understand perioperative risk is an important part of perioperative communication. However, shared decision-making is more than the process of providing information to the patient for the purposes of informed consent. 11 In order for shared decision-making to occur the clinician must understand the patient’s goals and fears and explore how these relate to the risk–benefit balance of the proposed surgery. This allows for a bespoke recommendation to be made to each individual patient based on an understanding of what matters to them.
The importance of having structures and processes in place in order to facilitate shared decision-making is increasingly recognised. As part of the Aotearoa New Zealand ‘Choosing Wisely’ campaign, the Australian and New Zealand College of Anaesthetists has emphasised the importance of having discussions that focus on goals of care and patient preferences when the perioperative risks are high. 12 In the USA the Agency for Healthcare Research and Quality promotes the use of the SHARE approach, 13 which encourages exploring risks and benefits of treatments through meaningful dialogue about what matters most to the patient.
Our traditional anaesthesia pre-assessment processes presented numerous barriers to shared decision-making for high-risk patients. These included the timing of the initial assessment (often once surgery was confirmed from the patient’s perspective), time constraints, lack of clear communication between specialists and a lack of education and training in the conduct of goals-of-care conversations. We have successfully piloted a pathway that has overcome some of these hurdles with dedicated referral processes, sufficient clinic time and the use of a structured communication tool and training programme.
Goals-of-care conversations are facilitated with our patients using the SICG. Many anaesthetists have had little formal training in shared decision-making and the clinicians involved in our pathway indicated a desire for education and tools to assist with goals-of-care conversations. The SICG gives clinicians specific questions and prompts using patient-tested language, which can be read from the guide during conversations with patients. The guide also lends itself well to a documentation template which we use to facilitate written communication with the surgeon and the patient’s primary care physician.
The serious illness conversation programme was initially developed in the USA by Ariadne Labs 14 and subsequently adopted and adapted for use in New Zealand by the Health Quality and Safety Commission. The programme includes the SICG as well as training and implementation resources (national advance care planning and clinical communication training programme supported by the Health Quality and Safety Commission). Pioneers of this work in the USA, Rachelle Bernacki and Susan Block 15 emphasise that clinicians should be trained in serious illness communication and take a structured approach to discussions of serious illness care goals, as well as documentation of these conversations. Although their original work has been outside the field of perioperative medicine, their advice seemed directly applicable to the work we were contemplating in our shared decision-making clinic with high-risk patients.
During our pilot programme we have found the SICG a useful tool for facilitating perioperative shared decision-making. Feedback from staff and patients has been positive, and the use of a structured approach to communication and documentation has been well received by clinical staff.
We are undertaking further research in this area to understand better the experiences and outcomes of the patients participating in our CDP. A prospective observational study of this patient cohort was commenced in May 2019.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20960734 - Supplemental material for Perioperative shared decision-making in the Bay of Plenty, New Zealand: Audit results from a complex decision pathway quality improvement initiative using a structured communication tool
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20960734 for Perioperative shared decision-making in the Bay of Plenty, New Zealand: Audit results from a complex decision pathway quality improvement initiative using a structured communication tool by Heidi C OFranklin mundsen Vicki L Higson Mark S Omundsen Jeremy I Rossaak in Anaesthesia and Intensive Care
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.