
Abstract
The number of older, frail patients undergoing surgery is increasing, prompting consideration of the benefits of intensive treatment. Despite collaborative decision-making processes such as advance care planning being supported by recent Australian legislation, their role in perioperative care is yet to be defined. Furthermore, there has been little evaluation of the quality of end-of-life care in the surgical population. We investigated documentation of the premorbid functional status, severity of illness, intensity of treatment, operative management and quality of end-of-life care in patients who died in a surgical unit, with a retrospective study of surgical mortality which was performed across three hospitals over a 23-month period in Victoria, Australia. Among 99 deceased patients in the study cohort, 68 had a surgical operation. Preoperative functional risk assessment by medical staff was infrequently documented in the medical notes (5%) compared with activities of daily living (69%) documented by nursing staff. Documented preoperative discussions regarding the risk of death were rarely and inconsistently done, but when done were extensive. Documented end-of-life care discussions were identified in 71%, but were frequently brief, inconsistent, and in 60% did not occur until 48 hours from death. In 35.4% of instances, documented discussions involved junior staff (registrars or residents), and 43.4% involved intensive care unit staff. Palliative or terminal care referrals also occurred late (1–2 days prior to death). Not-for-resuscitation orders were frequently changed when approaching the end of life. Overall, 57% of deceased patients had a documented opportunity for farewell with family. We conclude that discussions and documentation of end-of-life care practices could be improved and recommend that all surgical units undertake similar audits to ensure that end-of-life care discussions occur for high-risk and palliative care surgical patients and are documented appropriately.
Keywords
Introduction
Surgery in the elderly is becoming increasingly complex, leading to a greater demand for healthcare resources and a higher risk of dying in hospital. 1 The UK National Confidential Enquiry into Perioperative Deaths (NCEPOD) reported high rates of mortality in the frail and elderly population. 2 Similarly, the REASON study in Australia (2015) reported a 20% complication rate in surgical patients over 70 years of age, 3 compared with only a 0.3% rate for the overall surgical population. 4
In perioperative medicine, end-of-life decision-making is often needed because of the prevalence of life-threatening issues in older surgical patients. Although half of patients over 60 years of age required treatment decisions in their final days of life in a US study, 70% lacked the capacity to make such decisions themselves. 5 This, and other barriers, results in difficulties in providing end-of-life care (EOLC) that is consistent with patients’ preferences. 6 EOLC is a multifaceted process involving psychological, physical, emotional and spiritual needs. Despite its importance, the quality of EOLC in acute hospitals has been found to be highly variable.7,8
The Australian National Standards of Quality and Health Safety for EOLC in acute hospitals, 9 and many US and UK best practice palliative care guidelines, recommend that older patients should have advance care planning (ACP) consisting of goals of care discussions, advance directives and an appointed healthcare proxy (substitute decision-maker), before undergoing surgery. 10
Although there are established surgical mortality audits such as the Victorian Audit of Surgical Mortality and Australia and New Zealand Emergency Laparotomy Audit 11 that collect medical and operative data in relation to deaths, little is known about the end-of-life discussions and communication with regard to surgical patients in Australian hospitals. In this study, we aimed to assess aspects of EOLC practices and documentation in the acute hospital setting via a retrospective audit of deceased patients who had been admitted into surgical units in three Australian hospitals. We evaluated documentation of factors related to EOLC, including premorbid functional status, severity of illness, intensity of treatment, operative management and rates of ACP.
Methods
Study design and setting
We performed a retrospective observational study of all patients who died while under the care of a surgical unit at each of three hospitals: tertiary, district, and community healthcare services at Eastern Health, Victoria, Australia, during a 23-month period (15 May 2015 to 16 April 2017). Participants were identified from each of the three hospitals’ compulsory surgical mortality reports. Data were extracted from Eastern Health electronic medical records (EMRs) by two independent investigators. Where classification disagreement arose, a third expert opinion was sought. Ethics approval was obtained from the Eastern Health ethics committee (#QA62-2017).
Variables collected
We developed an assessment framework for the quality of EOLC in the perioperative setting from both the NCEPOD
12
and UK VOICES (Views Of Informal Carers – Evaluation of Services) audit
13
to reflect the acute hospital setting. Variables adopted for perioperative risk assessment and planning for high-risk patients derived from NCEPOD included:
Perioperative assessment: demographics, level of cognitive and physical function, and functional independence. Planning and intraoperative management: level of training, surgical indications and group documentation of risk discussion, planning and use of intraoperative monitoring. Postoperative support: postoperative acute clinical management, destination of care, intensive care unit (ICU) referrals, rapid response team (RRT) calls, and complications.
Variables regarding documentation of quality of EOLC from the VOICES study included:
Documentation and timing of EOLC discussions and resuscitation status, including not-for-resuscitation (NFR), goals of care. Communication between medical teams and family, evidenced by documentation of discussions in progress notes or anaesthesia charts. Opportunity to prepare for death, evidenced by time between discussion and death. Documented location of death and access to palliative care. Timing of cessation of curative or active treatments and postoperative course as documented in the medical progress notes or medication charts.
More subtle and subjective measures such as symptom relief and aspects of hospital environment (such as access to quiet and private rooms), the degree of family support, dignity, and independence were considered but could not be measured directly.
Statistical methods
Descriptive data were analysed using commercial software (IBM SPSS Statistics, IBM, New York, NY, USA and VasserStats, Vassar College, Poughkeepsie, NY, USA). Continuous variables are described as median with interquartile range (IQR) and counts as raw numbers and proportions. No assumptions were made about missing data.
Results
Demographics and preoperative assessment
We included all patients who died following admission to a surgical unit, which totalled 99 patients over 23 months. The median age for deceased patients was 82 (IQR 74–88) years. Several surgical subspecialties were included, but the common specialties included orthopaedic (24%), general surgery (22%), and vascular surgery (13%). Demographic characteristics are summarised in Table 1.
Baseline characteristics of patients at admission to hospital who died in a surgical unit in the three audit hospitals.
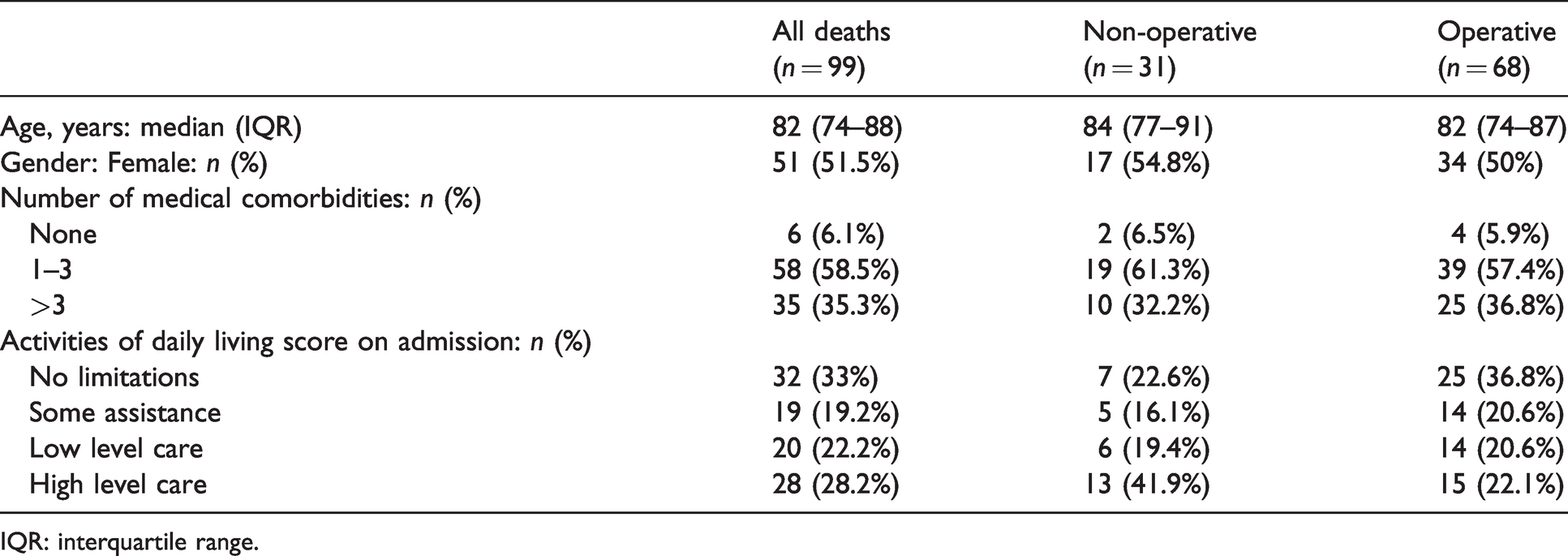
IQR: interquartile range.
One-third of patients had more than three comorbidities prior to death (Table 1). Although one-third had no limitation to activities of daily living (ADLs), another 28% normally required high level care. Among the 68 patients with documented anaesthesia review, 70% had an American Society of Anesthesiologists physical status (ASA) score of 4 or 5, 28% ASA 3 and 1.5% were ASA 1 or 2 (Table 2). One additional patient had an anaesthesia review and did not proceed to surgery. Of the 69 patients who were referred for anaesthesia, anaesthesia risk assessment scores of functional capacities were infrequently documented in 7.1% (5/69). In contrast, ADLs were documented by nursing staff in 69.8% (69/99) of the total deceased patients and all of those who presented for surgery (Table 2). No documentation was identified from the hospital EMR by any anaesthesia teams to record and clarify or discuss if any patients had a pre-existing ACP on or during admission, despite other NFR documentation and orders or EOLC discussions being done by other clinicians (medical, surgical, palliative care or ICU) during the patients’ hospital stay.
Documentation of perioperative risk management and planning for patients who died in a surgical unit in the three audit hospitals.
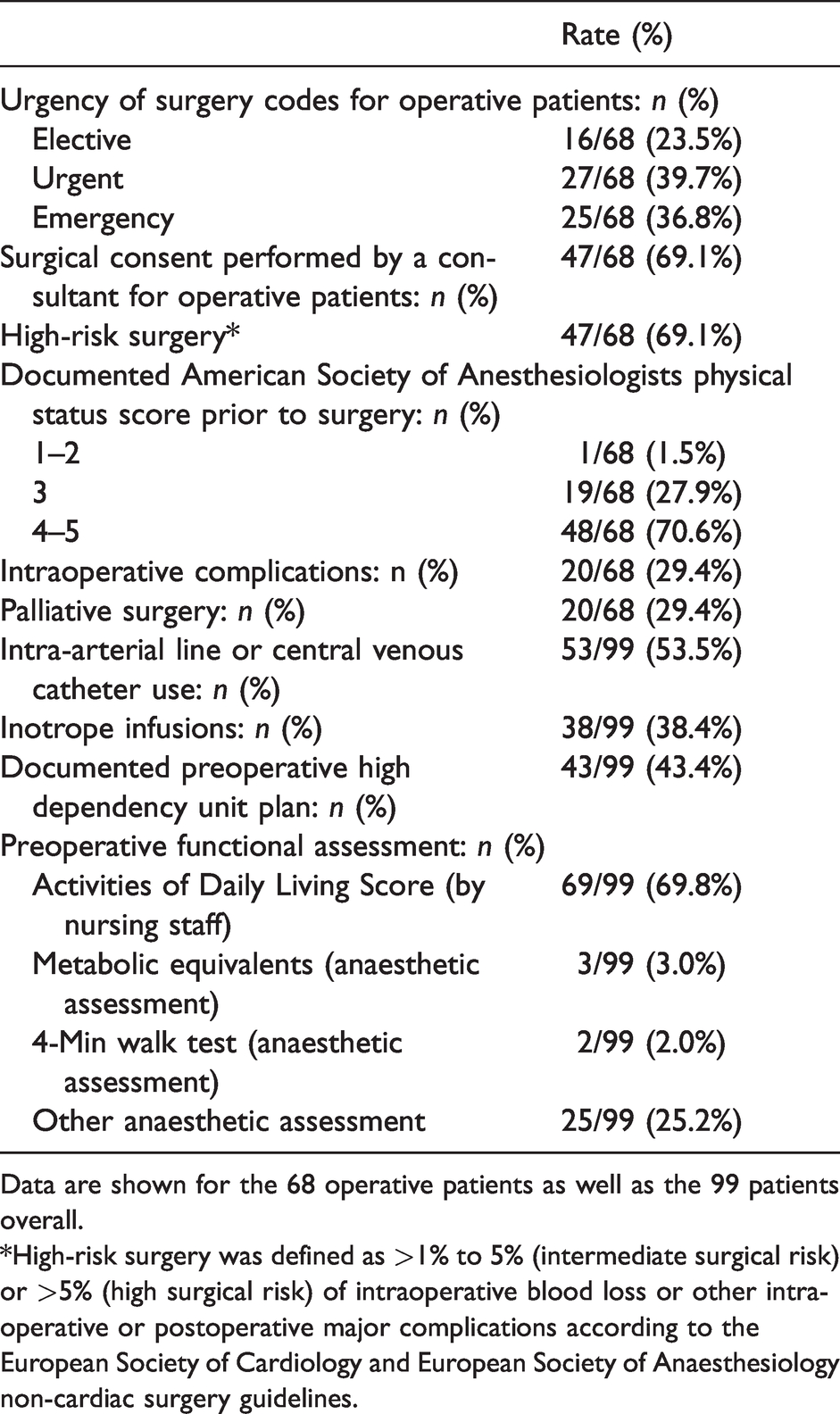
Data are shown for the 68 operative patients as well as the 99 patients overall.
*High-risk surgery was defined as >1% to 5% (intermediate surgical risk) or >5% (high surgical risk) of intraoperative blood loss or other intraoperative or postoperative major complications according to the European Society of Cardiology and European Society of Anaesthesiology non-cardiac surgery guidelines.
Surgery and critical care utilisation
Overall, 68 of the 99 deceased patients (68%) were treated operatively; of those, 23.5% (16/68) underwent electively booked procedures (Table 2). The remaining 31 patients did not undergo a procedure (non-operative). Of these, five patients entered the operating suite but did not undergo surgery. Most operations were classified as urgent (39.7%) or emergency (36.7%). In addition, 29.4% of surgery was classified as palliative (for the relief of symptoms caused by a life-limiting terminal illness). The median time from admission to theatre was nine hours (range three–27). The majority (79%) of the 68 patients who had a procedure had one operation, 16% returned once and 4.4% returned two or more times to theatre.
Most patients who underwent surgery received critical care resources and ICU perioperatively (58/68, 85.3%). Perioperative referrals to ICU were frequently unplanned, with half (29/59) occurring during or after surgery. At some point in their care, 62/99 (62.6%) of all patients were admitted to a critical care unit and 29.4% received an RRT or code blue call. The median interval between surgery and death in the operative group was four days. In the whole cohort of 99 patients, invasive monitoring use (central or arterial line) was documented in 53.5% and vasoactive (inotrope) medication infusion was required in 38.4% (Table 2).
Documented complications occurred in 29.4% (20/68) of patients during their care in the perioperative suite. More than half of patients (57.4%) who underwent procedures died in a high acuity care setting such as the perioperative suite or ICU (Table 3). Of the eight patients (12% of operated cases) who died in the theatre suite, six died in the operating room and two in the post-anaesthesia care unit (PACU). Of the six patients who died in the operating theatre, one died during induction, one during extubation and the remaining four died once surgery had commenced. Five of these were classified as ASA physical status 4E and one as 5E. Of the deaths in the PACU, one came directly from preoperative hold (and did not have surgery) and the other died after surgery.
Documentation of quality of end-of-life care in patients who died in a surgical unit in the three audit hospitals according to operative status.
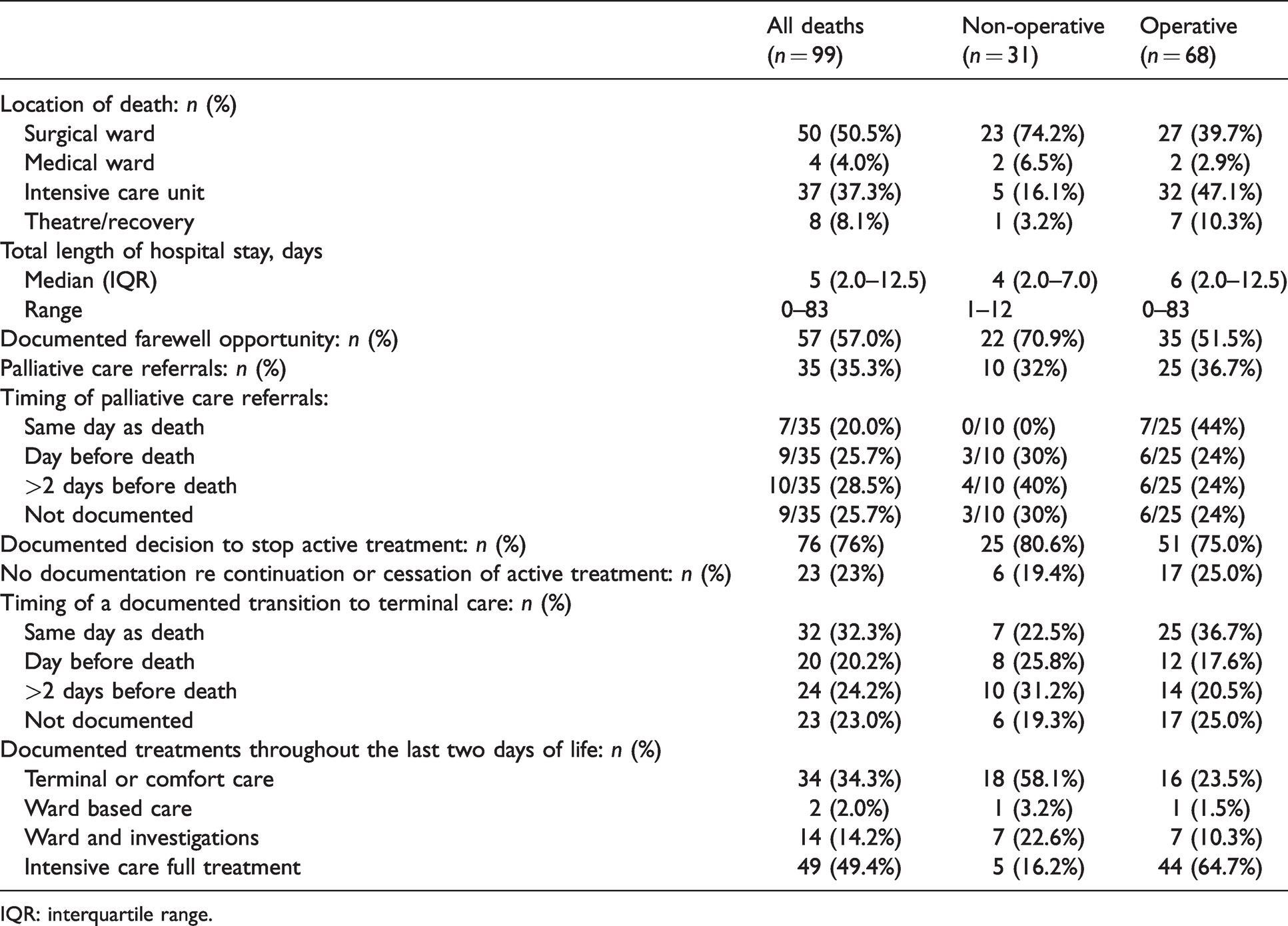
IQR: interquartile range.
Intraoperative cardiac emergency was reported in 15% of cases (10/68) and cardiac emergency in other perioperative locations (PACU and preoperative hold) was reported in 7% of cases (5/68). Cardiopulmonary resuscitation (CPR) was performed at least once in 22% (15/68) of patients undergoing surgery. Ten of these episodes of CPR occurred in theatre, two in the PACU room and three episodes with RRT calls. Direct current cardioversion was delivered to 4% of patients (3/68), all occurred in the theatre and all with concurrent CPR. Major transfusion was required in 13% of patients (9/68).
Assessment of quality of end-of-life care
We adapted the UK VOICES study methodology to assess the quality of EOLC across several variables. In this study cohort, the median length of hospital stay was five days (range 0–83) and the location of death was 50.5% on a surgical ward, 4.0% on a medical ward and 37.3% in the ICU (Table 3). The majority of patients (71%) had documented in-hospital EOLC discussions with either themselves and/or their family (Table 4). However, documented EOLC discussions, referral to palliative care services and transition to goals of comfort care all occurred late in the hospital course, with nearly half of palliative care referrals (45.7%) occurring on the day of, or the day before, death (Table 3). Several types of NFR or ‘goals-of-care’ forms were identified in the medical records, and these were often altered or updated throughout the patient’s hospital stay. Documented resuscitation status at the time of death was 13.1% for full resuscitation, 40.4% for limited resuscitation and 37.4% for palliative care (Table 4). No resuscitation or goals-of-care hospital-specific forms were identified in 9.1% of the cohort. Nearly a third of these forms (29%) were completed concurrently with a code blue or RRT call with a median time of completion of 2.5 days before death (Table 4).
Documentation rates of discussion of goals of care for patients who died in a surgical unit in the three audit hospitals.
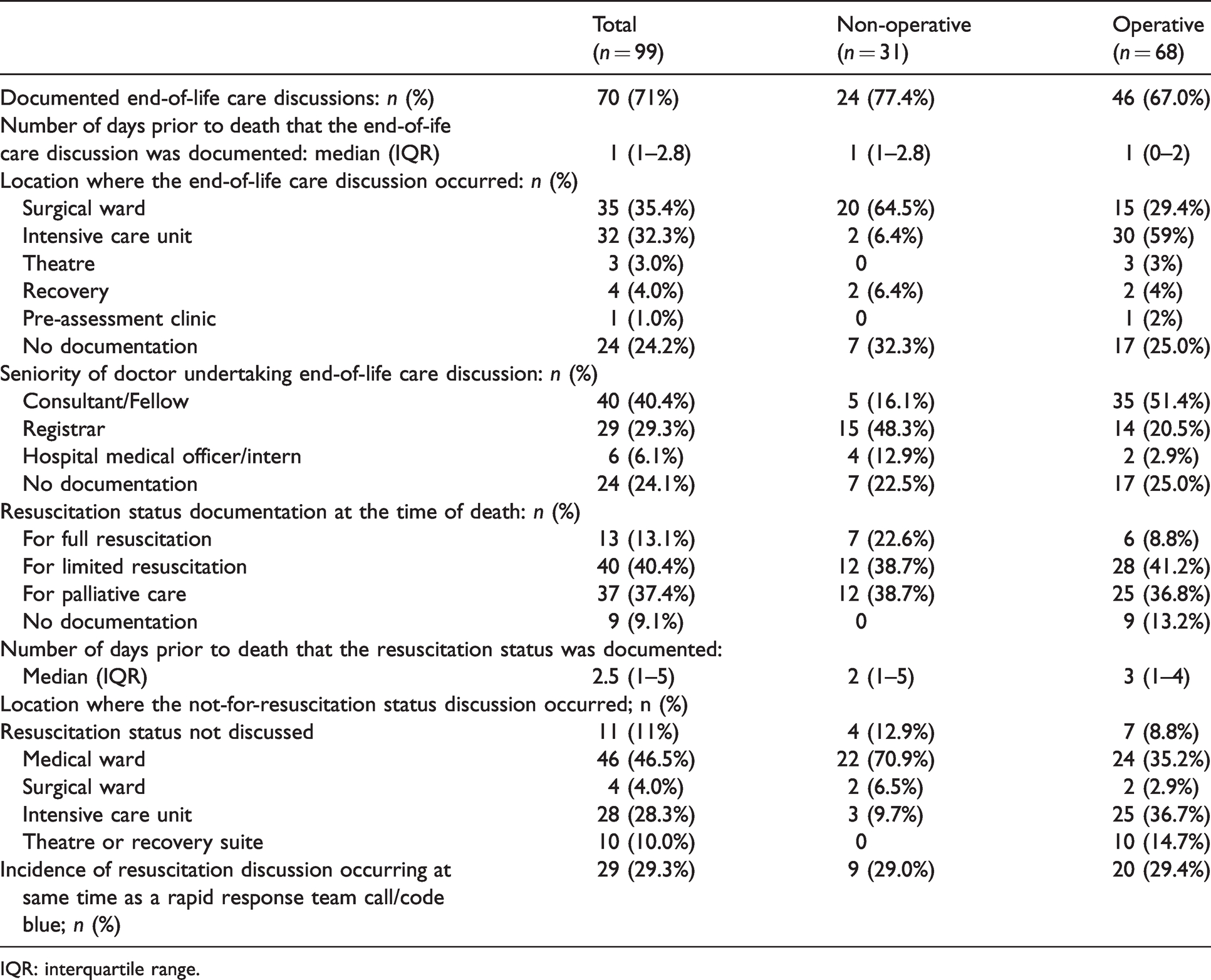
IQR: interquartile range.
Overall, only 57% of patients had a documented opportunity for a farewell, which was defined as a period of time prior to death when the patient was conscious, aware of the imminent risk of dying and was able to speak with loved ones or next of kin (Table 3). This was mostly due to the fact that 49% of patients received full intensive care treatment throughout the last days of life, and most of these patients had no opportunity for a farewell with family or carers while intubated and sedated.
Most documented EOLC discussions involved more than one hospital team from palliative care, medicine, surgery, ICU or anaesthesia (Table 4). Fifty-one percent of EOLC discussions in operative patients involved senior (either Fellows or consultant) medical staff (Table 4). For operative patients, the majority of resuscitation directive forms and discussions were completed in the ICU (37%) and medical wards (35%), another 15% in the operating suite and only 3% in the surgical ward. In non-operative patients a much higher proportion of forms were completed and discussions occurred in the medical ward (71%) and much lower (9%) in ICU. Of the 24% (16/68) of patients who were booked for elective surgery, only one had an EOLC discussion in the anaesthesia pre-assessment clinic (Table 4).
Features of non-operative patients
The baseline characteristics for both operative and non-operative groups were similar (Table 1). Non-operative patients predominantly died on a surgical or medical ward (80.7%) (Table 3). In this group, most EOLC discussions (64.5%) occurred on the surgical ward, more typically with end-of-life discussions performed by junior staff members of the surgical unit or palliative care service (Table 4). An opportunity for farewell (70.9% versus 51.5%) was more common in non-operative patients (Table 3). Only 16.2% of the non-operative patients versus 64.7% of the operative patients received full intensive care treatments throughout the last two days prior to death (Table 3).
Discussion
We evaluated documented patterns of EOLC and perioperative planning for 99 deceased patients admitted to a surgical unit, 68 of whom underwent a procedure (most of which were non-elective or urgent) and 31 of whom did not have a procedure. We found very infrequent documentation of the presence of ACP. In addition, referral to palliative care services occurred in one-third and was often provided late.
Comparison with previous studies
The median age in the whole cohort in this study was 82 years, consistent with other Australian surgical mortality audits. 4 Our study revealed a much higher fraction of patients receiving critical care compared to the UK NCEPOD study (83% versus 22%), 12 and somewhat higher than the SNAP-2 EPICCS audit in the UK, Australia and New Zealand. 14
Although ADLs were documented in many cases, functional assessment and anaesthesia risk scores were only documented in 4%. Low rates of usage of risk prediction tools have also been found in other international and Australian studies, in which the majority of clinicians in the real world rely primarily on clinical judgement. 15
The vast majority of patients died outside the operating suite. These high-risk patients needing predominantly emergency care, would be the most likely to benefit from preoperative goals of care and shared decision-making discussions. Surgical subgroups of these high-risk patients are currently being investigated, such as those requiring emergency laparotomy surgery, 11 and those investigating neck of femur hip fracture. 16
Our study found major differences in the location of death within the hospital depending on operative status; the most common location of death for operative patients was the ICU, whereas the majority of patients in the non-operative group died on a ward.
Overall, 71% of patients had an EOLC discussion. Published studies suggest that patients expect doctors to discuss EOLC, 17 yet in this study we found that these discussions often did not happen until terminal stages of life. For patients who underwent an operation, almost all documented discussions were performed after surgery, with one-tenth of these discussions occurring urgently or in the operating theatre suite, and only one in the pre-admission clinic.
EOLC discussions were more frequently done by consultants when patients had more invasive treatments such as ICU or surgery. This is consistent with known barriers to EOLC, 18 and highlights the need for further education in the surgical palliative care setting. 19
Similar findings were reported by Wilson et al. in a study from Oregon, USA. 20 In that study, the median time from palliative care referral to death was only ten hours. In another study of 150 elderly hip fracture patients, 86% had no documented EOLC planning discussions, despite the known high mortality rates after surgery in this population. 21
Generalisability, limitations and strengths
The results of this study are potentially generalisable to other general community hospitals. All surgical patients were eligible, and thus our study captured a cohort of surgical patients who, due to their very high risk of mortality (ASA physical status scores of 4 or 5) undergoing emergency surgery or conservative surgical management, are rarely included in trials, studies and are under-represented in the literature. The retrospective nature of the study exposes it to selection bias from convenience sampling and data collection was limited to documentation of discussions and clinical care events that are recorded in the EMR.
Implications for clinicians and policy makers
Surgery prior to death or dying in hospital is an increasingly common scenario; nearly a third of all patients will have inpatient surgery in their last year of life.22,23 It can be confronting and difficult to discuss openly a patient’s preferences for care when in an emergency surgical situation, especially when more than 46% of patients aged over 70 years are found to have impaired cognition due to their acute illness or underlying comorbidities.24–26
In the USA, 80% of patients die in a medical institution, 23 despite 67% stating a preference to die at home. 27 The consequence of a failure to identify and appropriately care for dying patients is burdensome care with substantial economic and emotional cost to all involved. ACP is a collaborative patient-centred process that enables more timely, personalised and appropriate care, and leads to improved patient end-of-life care, reduced distress, and improved family satisfaction. 28 ACP has been shown to increase the uptake of palliative care and reduce the provision of life-sustaining treatments at the end of life. In addition, hospice care and ACP can save 25%–40% in costs in the last month of life. 29
Despite recent supportive Australian legislation, the role of ACP in the surgery and anaesthesia setting remains to be clearly defined.30,31 Our findings support a need for guidelines and increased education and training in the recognition of dying patients in the three hospitals audited, and potentially in hospitals more broadly. 32 Implications include the need to have increased shared decision-making and ACP discussions led by senior clinicians and staff for high-risk patients, increased education of staff and community awareness around ACP, the need to explore opportunities for improved quality of EOLC and earlier transitions to incorporate shared palliative care in surgery. Importantly, since this study was conducted, several jurisdictions in Australia have introduced legislation emphasising the binding nature of advance care directives and plans.
Surgeons are becoming more receptive to shared decision-making when deciding to operate. 33 In Australia and the USA, an audit and survey of surgeons reported that 26% would change the decision to operate in retrospect after a death, 34 and that more than half of surgeons would not operate in the context of a do-not-resuscitate order. 35 However, barriers to ACP in surgery remain and include limited community awareness, reluctance of healthcare professional involvement, 36 the short-term nature of surgical goals and planning, limited education in ACP and the inherent nature of resuscitation in anaesthesia. 30 ACP and perioperative shared decision-making could be integrated into the routine surgical consent process, ideally in the pre-admission clinic.17,37 A protocol for incorporating patient-centred ACP into the surgical pathway has been developed and obtained ethics approval at Townsville Hospital in Queensland. 38 Stratifying patients who enter the perioperative care pathways in a more routine and clearer manner, according to risk, resource requirements and goals of care may assist multidisciplinary teams to provide proactive surgical planning 39 and collaborative palliative care. 40
Conclusion
Among 99 surgical patients who died in three hospitals, documentation of collaborative patient-centred discussions and appropriate goal-directed care was limited. Furthermore, documented discussions were often in the last days of life. In surgical patients at high risk of dying, early EOLC discussions, led by senior clinicians and palliative care referrals, should be considered. Our discussions and documentation of EOLC practices could be improved and we recommend that all surgical units undertake similar reviews or audits to ensure that EOLC discussions occur for high-risk and palliative care surgical patients and are documented appropriately.
Footnotes
Author contributions
Acknowledgements
The authors acknowledge Eastern Health for ethics approval and EMR patient record access, Monash University for access to RedCap and SPSS statistical software.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the Australian Society of Anaesthetists and a PhD support grant 2019.