
Abstract
Corneal abrasions are an uncommon complication of anaesthesia. The aim of this study was to identify potential risk factors, treatment and outcomes associated with corneal abrasions reported to the web-based anaesthesia incident reporting system (webAIRS), a voluntary de-identified anaesthesia incident reporting system in Australia and New Zealand, from 2009 to 2021. There were 43 such cases of corneal abrasions reported to webAIRS over this period. The most common postoperative finding was a painful eye. Common features included older patients, individuals with pre-existing eye conditions, general anaesthesia and procedures longer than 60 minutes. Most cases were treated with a combination of lubricating eye drops or aqueous antibiotic eye drops. The findings indicate that patients who sustain a perioperative corneal abrasion can be reassured that in many cases it will heal within 48 hours, but they should seek earlier review if symptoms persist or deteriorate. None of the cases in this series resulted in permanent harm. Well established eye protective measures are important to utilise throughout the perioperative period, including the time until the patient has recovered in the post-anaesthesia care unit.
Introduction
It has been stated that in 1937 Guedel said ‘there was too much conjunctivitis and keratitis following anesthesia’. 1 As far as the authors were able to determine, corneal abrasions during anaesthesia were first formally investigated in 1977. 2 This study discovered that the incidence in patients without eye protection was as high as 44%. 2 The main risk factor for corneal abrasion was ‘lagophthalmos’, or incomplete eye closure, which was exacerbated by the use of anaesthetic drugs. More recent studies investigating the use of eye protection have demonstrated a reduced incidence of corneal abrasion from 44% to 0.023%–0.13%.2–5 Risk factors for corneal damage suggested by these more recent studies included older patients (>55 years old), general anaesthesia (due to decreased tear production and blunting of the corneal blink reflex), longer duration of a procedure (greater than 60 minutes), greater blood loss or prolonged hypotension, patient positioning (including lateral, prone or Trendelenburg) and the use of oxygen in transport to the post-anaesthesia care unit (PACU).3–5
Diagnosis of a corneal abrasion includes a focused history and eye examination. Typically, patients may experience painful, red, watery eyes, a foreign body sensation or blurred vision two hours postoperatively.6,7 Any blurred vision may result from ocular oedema, but corneal abrasion should not be causing significant loss of vision. 7 Pupil size, pupil reactivity and extraocular eye movement should all be normal.6,7 A corneal abrasion may be confirmed by cobalt blue light on the fluorescein dye test. Treatment for corneal abrasions includes lubricating eye drops, antibiotic eye drops or local anaesthetic drops for initial symptomatic relief.5–7 Abrasions of less than 25% of the cornea have been shown to heal within 24 hours. 6 If there is any ongoing or worsening of symptoms, patients should be referred to an ophthalmologist for ongoing management.
The objective of this study was to determine if there were any identifiable risk factors in this case series from individuals who experienced postoperative corneal abrasions and to document the treatment they received and the outcome.
Methods
The web-based anaesthesia incident reporting system (WebAIRS) is a voluntary de-identified anaesthesia incident reporting system, which was introduced in Australia and New Zealand in September 2009. 8 The methodology of the system has been described in previous articles. 8 WebAIRS is owned, managed, and funded by three organisations: the Australian and New Zealand College of Anaesthetists, the Australian Society of Anaesthetists, and the New Zealand Society of Anaesthetists. Registered anaesthetists across Australia and New Zealand have been invited to report anaesthetic incidents via the webpage www.anztadc.net from 2009 onwards. Data describing the incidents can be entered via non-mandatory data input web controls, and in the form of text allowing the reporters to describe the incident and enter their reflections regarding contributing and alleviating factors.
An overview of the first 4000 incidents was published in 2017, in which the methods of the de-identified data collection were described. 8 Data were collected in compliance with the National Health and Medical Research Council 2014 recommendations for de-identified quality assurance data. 9 In order to ensure that the project meets the requirements for de-identification, multicentre ethics approval is maintained at the Royal Brisbane and Women’s Hospital Human Research Ethics Committee (HREC/11/QRBW/311) and the Nepean Blue Mountains Local Health District (HREC/12/NEPEAN/18). In New Zealand, ethics approval has been obtained from the Health and Disability Ethics Committee (MEC/09/17/EXP). All ethics committees suggested that the data collected for age and procedure duration be grouped rather than an actual age or procedure duration to reduce the chance of surrogate identification.
A narrative search using structure query language was performed on the whole database, which at the time of searching contained 9400 reports submitted from webAIRS inception in 2009 to 12 December 2021, to identify events that might have involved the cornea. The structure query language search was designed to return reports that contained the words cornea, corneal, abrasion, abrasions, ulcer or similar matching words. These reports were reviewed by the authors and separated into those which matched the selection criteria (analysis group) and those that matched the search criteria but did not meet the selection criteria (excluded group). Data were extracted from the database for the analysis group, which included patient demographics, information about the surgical procedure (urgency, specialty), as well as information regarding the anaesthesia administered (anaesthetic technique).
Results
There were 47 cases of perioperative corneal abrasions reported to webAIRS. Forty-three cases were eligible for inclusion in this case series. Four cases identified by the word search of the database were excluded. One case was a corneal abrasion that occurred three months postoperatively, which was unlikely to have been related to the procedure. Two cases of eyelid skin abrasion were excluded. No diagnosis of corneal abrasion was reported in the remaining case.
Of the 43 confirmed cases of corneal abrasions, 28 (65%) were women, 31 (72%) had a general anaesthetic and in 28 (65%) the duration of procedure was longer than 60 minutes. Two patients suffered from proptosis/exophthalmos and had difficulties closing their eyes. One patient presented with a pre-existing chronic ophthalmological condition. Eye protection was documented for 28 (65%) patients. Two patients were exposed to alcohol or to chlorhexidine surgical preparation fluid. Positioning was a large contributor, with nine lateral, four prone and three in the Trendelenburg position. Treatment included chloramphenicol antibiotic drops (n = 29), lubricating eye drops or saline (n = 13), local anaesthetic drops (n = 3) or steroid drops (n = 1). An ophthalmologist reviewed 28 (65%) of the cases. None of the cases involved permanent damage. A summary of the 43 cases is shown in Table 1 and in Figure 1, while a description of five notable cases (cases 2, 10, 19, 25 and 35, Table 1) is included below. These cases each involved either suspected corneal injury, despite standard care being performed, or injuries that occurred in the immediate postoperative period.
Summary of cases of perioperative corneal abrasions identified from the webAIRS database.
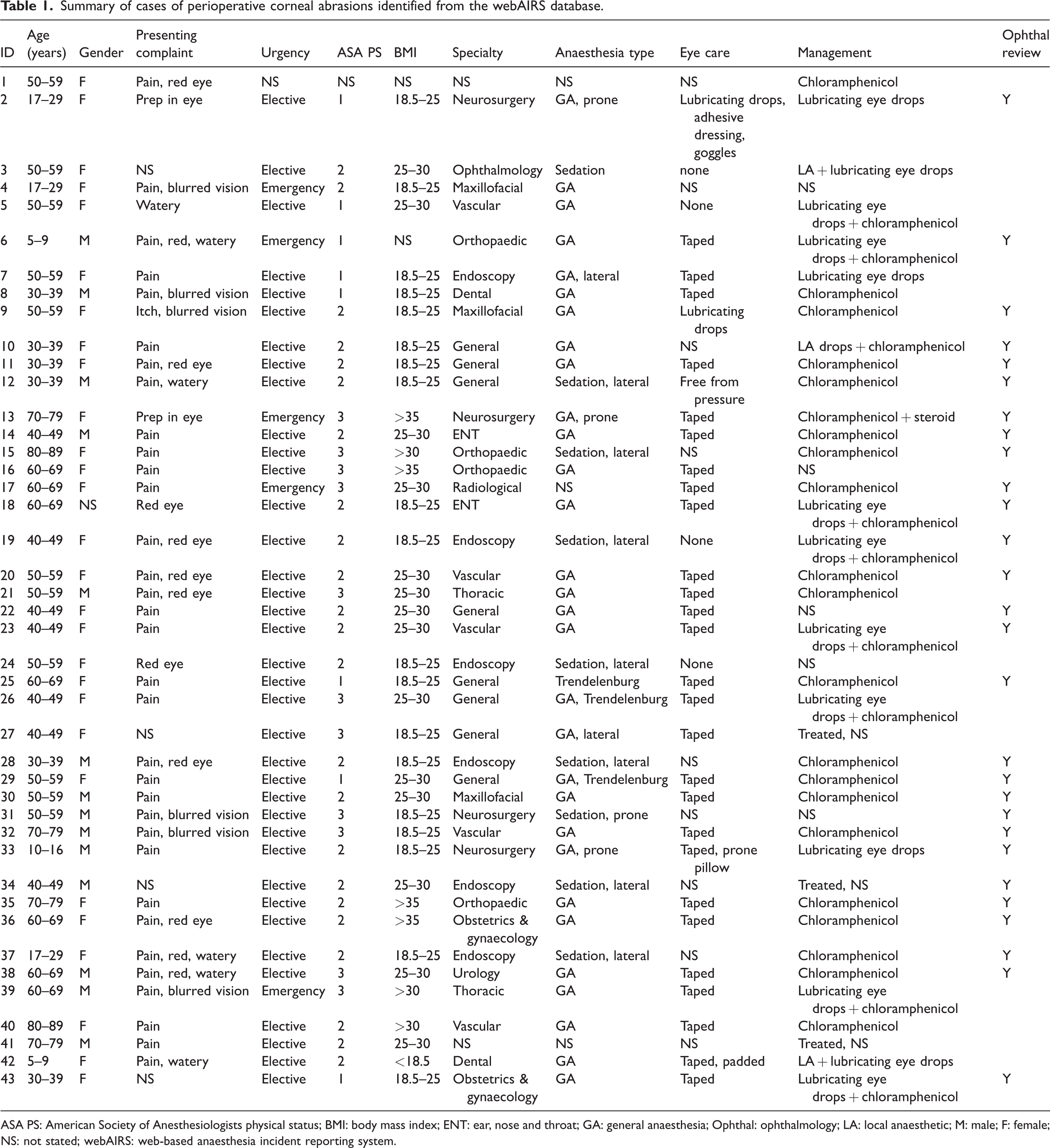
ASA PS: American Society of Anesthesiologists physical status; BMI: body mass index; ENT: ear, nose and throat; GA: general anaesthesia; Ophthal: ophthalmology; LA: local anaesthetic; M: male; F: female; NS: not stated; webAIRS: web-based anaesthesia incident reporting system.
Case 2
An adult American Society of Anesthesiologists physical status (ASA PS) 1 woman in the 17–29-year-old age group underwent an elective posterior craniotomy. For eye protection, corneal lubricant, two large adhesive dressings and adhesive goggles were applied after intubation. The patient was then positioned prone and the head held in place by Mayfield pins. At the end of the nine-hour procedure, the patient was noted to have chlorhexidine prep under the adhesive dressing with a thin stain on the lower conjunctiva. The eye was thoroughly washed with saline and ophthalmology was contacted for review.
Case 10
An ASA PS 2 patient in the 30–39-year-old age group underwent an elective laparoscopic abdominal procedure. No eye protection was stated for the procedure. On extubation, the patient rubbed their eyes with the back of their hand resulting in the cannula scratching their eye. In the PACU the patient complained about a red eye. The patient was reviewed by ophthalmology, who diagnosed a corneal abrasion and treated it with local anaesthetic drops and antibiotic ointment (chloramphenicol). Symptoms resolved within 24 hours.
Case 19
An ASA PS 2 patient in the 40–49-year-old age group underwent an elective colonoscopy. No eye protection was used in the case, but both eyes were completely closed throughout the procedure while lying in the left lateral position. In the PACU the patient complained of a painful, red eye. On an eye examination, visual acuity, movement and fields were normal. Both pupils were equal and reactive to light. Pain resolved on administration of local anaesthetic drops. Fluorescein examination revealed a less than 25% corneal abrasion. The case was discussed with ophthalmology, who suggested treatment with lubricating eye drops and antibiotic ointment (chloramphenicol) for four days and to seek further assistance if symptoms persisted beyond four days.
Case 25
An ASA PS 1 patient between 60 and 69 years of age underwent an elective laparoscopic abdominal procedure. Despite both eyes being taped, at the end of the procedure it was noted that the left eyelid remained half open. Ophthalmology reviewed the patient after the procedure and diagnosed a 30%–40% corneal abrasion and commenced antibiotic ointment (chloramphenicol).
Case 35
An elderly ASA PS 2 patient in the 70–79-year-old age group underwent an elective major lower joint replacement. Eyes were taped after intubation. On extubation, the patient was combative, delirious, and removed the Hudson mask. Once they settled in the PACU, they had a painful left eye and were found to have a less than 20% corneal abrasion at the lateral canthus. The anaesthetist commenced antibiotic ointment (chloramphenicol) and suggested the patient follow up with an optometrist on discharge.
Discussion
We have analysed 43 cases that were reported to webAIRS that have had a corneal abrasion in association with anaesthesia. The most common postoperative finding was a painful eye. Common features included older patients, individuals with pre-existing eye conditions, general anaesthesia and procedures longer than 60 minutes. Most cases were treated with a combination of lubricating eye drops or aqueous antibiotic eye drops. The findings indicate that patients who sustain a perioperative corneal abrasion can be reassured that in many cases it will heal within 48 hours, but they should seek earlier review if symptoms persist or deteriorate. It was reassuring that none of the cases in this series resulted in permanent harm.
There have been two recent publications on corneal abrasions in association with anaesthesia; one reporting 118 cases in 2015 and another reporting 86 cases in 2014.4,5 There was also a series of 34 cases published in 1996. 11 A brief review of these papers reveals that corneal abrasions are an uncommon (0.023%–0.13%) complication of anaesthesia that appear to be readily recognised after a procedure. Corneal abrasions can occur at any stage of anaesthesia from induction until discharge from the PACU. The usual cause has been stated to be lagophthalmos resulting in dry eyes, which may be exacerbated by oxygen masks in the early postoperative period. Lagophthalmos, which is the clinical term for eyes failing to close completely, might be an existing medical condition or may be secondary to the effects of anaesthetic drugs. Recently, it has also been suggested that patients might rub their eyes as they awaken and either scratch their cornea directly or with intravenous cannulae, arterial oxygen saturation (SaO2) probes or other attached devices. Therefore, the use of eye protection throughout the perioperative period is paramount. In the event that a corneal abrasion does occur, then supportive measures such as lubricant eye drops and aqueous antibiotic drops are usually effective. In refractory cases or where the injury appears severe at the outset, an ophthalmic review should be sought at an early stage. This paper reinforces the importance of implementing eye protective measures, the recognition of corneal abrasions postoperatively by medical staff, commencing simple management to relieve the symptoms and assisting in the healing, while engaging in follow-up to monitor for deterioration. While it is not possible to compare our study and these reports directly, the findings were broadly similar. The webAIRS system is also voluntary, and therefore the results might be affected by the reporting process. There was a higher incidence of corneal abrasion under sedation in our study compared with the literature. However, this may reflect the variation in case-mix between the above single centre studies and the webAIRS binational anaesthetic incident reporting database.4,10
In keeping with previous literature, our results reflect the common postoperative complaints from corneal abrasion including the characteristic painful red eye. In 28 cases, there was documented ophthalmology specialty input. The most commonly recommended management strategy (Figure 1) was aqueous antibiotic drops (n = 27) and lubricating eye drops (n = 8). In the event of a suspected corneal abrasion, an eye examination should be performed by either the attending anaesthetist or an ophthalmologist. Local anaesthetic drops can be used to facilitate an eye examination. However, the patient should not be sent home with local anaesthetic drops, as it may mask pain that would indicate progression to ulceration or infection and warrants specialist review. 7 An ophthalmologist should be contacted if the patient is found to have a foreign body in the eye, there is a significant reduction in visual acuity, the cornea is hazy/opaque or there is any other clinical concern.6,7
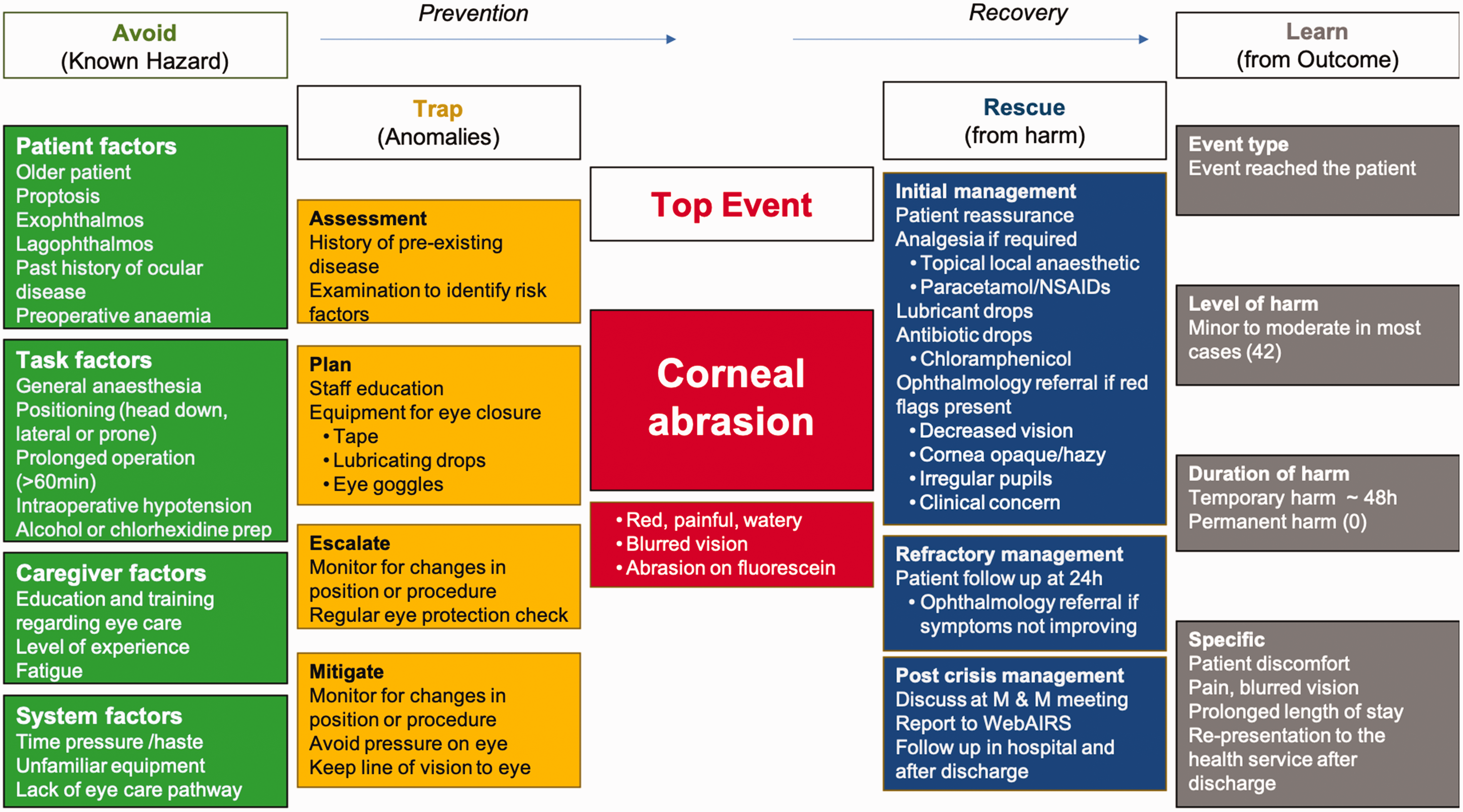
In order to present all of the known considerations collectively regarding the hazards, prevention, rescue and outcomes regarding corneal abrasions, the authors have created a bowtie diagram (Figure 1). 11 It should be noted that some of the content of bowtie diagrams include points for consideration as well as data from this study or from published material.11,12 Except where data are derived from this study, the level of evidence would therefore be expert opinion and be regarded as factors for consideration rather than the presentation of facts. Hazards that can increase the risk of corneal abrasion shown in Figure 1 include patient factors (patients with eyes that are difficult to close due to proptosis/exophthalmos or pre-existing chronic ophthalmological conditions).5–7 In our cases series, older age was not a risk factor for developing perioperative corneal abrasions. Although women appear to have an increased risk, with almost twice as many cases of corneal abrasions compared to men, this is likely to be an incidental finding, as other papers report either a greater proportion of men or a similar distribution.4,10 Task factors include the procedure task factors (head or neck procedures, surgical preparation (prep) fluid containing alcohol or chlorhexidine, procedure longer than 60 minutes, lateral/prone/Trendelenburg positioning, surgeons putting pressure on eyes through drapes)5–7 and anaesthetic task factors (general anaesthetic–induced lagophthalmos, intraoperative hypotension). General anaesthesia and sedation, as well as regional or local anaesthesia affecting the eye, may either abolish or suppress the eyelid reflex. Under normal circumstances the eye blinks every 3–4 seconds to provide moisture and lubrication to the cornea. Corneal epithelium is extremely sensitive to dryness, and even short periods of exposure leads to dryness and ulceration (exposure keratopathy). The risk is increased in exophthalmos which might leave exposure areas of the eye even though the eye has been taped. Caregiver factors include education and awareness of the complication, level of experience, and fatigue. System factors include time pressure, unfamiliar equipment, and lack of a specific eye care pathway. In addition, if the eye is not completely closed the tape might stick to the surface of the eye. Rough removal of eye tapes can result in small skin tears or abrasions resulting in irritation and patients vigorously rubbing their eye postoperatively that may result in abrasion. 4 The effects of lagophthalmos from a general anaesthetic will reduce during the immediate postoperative period; however, the use of regional anaesthetics for ophthalmological procedures can be longer lasting and eye care should be taken for the duration that the local anaesthetic is expected to last.
A list of possible preventive measures is shown in column 2 of Figure 1 under the headings assessment, plan, escalate and mitigate. Employing simple eye protective measures can significantly reduce the risk of corneal abrasions, including goggles to prevent compressions, ocular lubricants to prevent ocular desiccation, and occlusive dressings to keep the eye closed and provide protection from chemical irritation. 7 In the prone position there is increased intraocular pressure despite the use of pinned head-holders or prone pillows, which may contribute to the risk of developing a corneal abrasion. 13 In the present case series of 43 patients, 28 corneal abrasions occurred despite the implementation of these measures. Current evidence indicates that there is no advantage to combining lid taping and lubrication over using lid taping alone in low-risk cases. 7 In four cases included in this series, the corneal abrasion was suspected to occur in the postoperative period. Common mechanisms in which medical equipment contributed to corneal injury on emergence were the patient rubbing their eyes with an oxygen saturation probe on the index finger or a peripheral intravenous cannula on the dorsum of the hand, or from the Hudson mask being placed too high either covering the eyes resulting in dry oxygen or the plastic scratching the eye. On emergence some authors have suggested placing the oxygen saturation probe on the ring or fifth finger. 14 Therefore, eye protection measures should be continued until the patient is awake in the PACU.
After the top event (corneal abrasion) there is still an opportunity to rescue the situation and minimise the harm. Strategies for rescue are shown in Figure 1 under the headings: initial management, refractory management, and post crisis management.5–7 Initial management for corneal abrasions may include lubricating eye drops, local prophylactic topical aqueous antibiotic drops, and monitoring of the resolution of symptoms.6,7 In keeping with Australian guidelines, chloramphenicol aqueous antibiotic drops have been used for the treatment of corneal abrasions resulting from exposure. 15 With prompt management, pain will significantly improve over the first 24 hours, with superficial injuries healing over 48–72 hours. 7 However, if symptoms become worse, patients should be reviewed by a specialist for ongoing management. These simple measures can be used in any department if a corneal abrasion is suspected (i.e. no equipment formally to diagnose corneal abrasion or no in-hospital ophthalmology service available). It should be noted, if there is any indication of chemical damage from alcohol or chlorhexidine-containing preparation fluid, the eye should be thoroughly irrigated with saline and ophthalmology contacted for urgent review. 16 In addition, care should be taken to protect the eyes during the application of preparation fluids around the head or to avoid solutions that could lead to eye irritation. Therapeutic contact lenses might be considered in conjunction with an ophthalmologist for cases that do not respond rapidly to simple measures. 17 To the authors’ knowledge, there are no standardised national or statewide specific eye care pathways used in Australian anaesthetic departments to facilitate independent management of corneal injuries. This would especially be the case for private practice in which there might not be a formal anaesthetic department, and where anaesthetic services are provided by one or more private anaesthetic groups, or by individuals. Anecdotally, it is believed that some anaesthetic departments have developed their own pathways for eye protection during anaesthesia and for the management of any eye injuries that might accidentally occur.
These protocols and clinical pathways are generally developed at the local level in collaboration with nursing administration, healthcare facilities management, and anaesthetists for the preventive measures as well as follow-up and open disclosure. An anaesthetic department from the USA developed an anaesthetist-led protocol initially to manage corneal abrasions, despite an expected incidence of 0.13% corneal abrasions over a five-year period from 91,064 operations. 5 In that study, the anaesthesiologist managed the majority of corneal injuries independently after receiving training from the ophthalmology department using a corneal abrasion protocol, and escalated care to ophthalmology in only 6.8% of reported cases. 5 Establishing these pathways would require commitment from ophthalmology, anaesthetic and perioperative staff and ongoing training to be an effective tool to recognise and manage simple corneal abrasions. The higher incidence of ophthalmology involvement demonstrated by these data may reflect the lack of such protocols being developed by local anaesthetic departments.
Finally, the possible outcomes and learning points are shown in the right-hand column of Figure 1 under the headings: type of event, level of harm, duration of harm and specific outcomes that might occur. None of the cases in this series resulted in permanent harm, with rapid identification and treatment of corneal injury. With prompt recognition, treatment and follow-up there was no evidence from this series or from the papers identified by authors that there were any long-lasting sequelae from corneal abrasions.4,5
This study has similar limitations to previous publications using webAIRS data from voluntary reporting of adverse events. 18 As reporting is voluntary and so few cases were reported, it is not possible to determine numerators and denominators or calculate a positive predictive value for any hazards identified. Therefore, this study can only represent those cases that were reported to the webAIRS database and it is possible that other more serious corneal abrasions were not reported. In addition, the information is limited by what is documented by the treating anaesthetist and is therefore at risk of reporter bias. Finally, as webAIRS reports represent a cross-section of time in the event reported, there is no information regarding follow-up or long-term outcomes.
In conclusion, anaesthetists take part in routine eye care for patients under anaesthesia to mitigate the risk of damage to eyes. It is a problem that was readily identified over 80 years ago. However, despite the implementation of numerous preventive measures, some patients still sustain corneal abrasions. This might indicate the need for more standardised pathways for; first, assessment of risk factors and implementing routine eye care during anaesthesia, and second, for perioperative management of anaesthesia-related corneal injury. The information available from the Royal College of Anaesthetists 19 and hopefully the bowtie diagram included in this article (Figure 1) might provide a useful source of information to assist with the creation of these pathways in Australia, which will include the risks, the prevention and how to manage this complication. Patients can be reassured that with prompt treatment, most cases will improve within 24 hours. None of the cases identified in this series resulted in permanent damage. Those who have worsening symptoms on follow-up should be referred to an ophthalmologist for ongoing management.
Supplemental Material
sj-jpg-1-aic-10.1177_0310057X221099032 - Supplemental material for Perioperative corneal abrasions: A report of 42 cases from the webAIRS database
Supplemental material, sj-jpg-1-aic-10.1177_0310057X221099032 for Perioperative corneal abrasions: A report of 42 cases from the webAIRS database by Matthew R Bright, Leigh D White, Sandra I Concha Blamey, Yasmin Endlich and Martin D Culwick in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-2-aic-10.1177_0310057X221099032 - Supplemental material for Perioperative corneal abrasions: A report of 42 cases from the webAIRS database
Supplemental material, sj-pdf-2-aic-10.1177_0310057X221099032 for Perioperative corneal abrasions: A report of 42 cases from the webAIRS database by Matthew R Bright, Leigh D White, Sandra I Concha Blamey, Yasmin Endlich and Martin D Culwick in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to acknowledge the contribution of all members of the Australia and New Zealand Tripartite Anaesthetic Data Committee (ANZTADC), past and present, and the large number of anaesthetists reporting incidents to webAIRS in the interests of greater patient safety.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.